Start with the first abnormal surface: meninges, retina, ring abscess, or white matter. That single choice usually tells you the organism before the stem finishes talking.
Choose the presenting door
Four Organism Locks
Each lock has its own board fingerprint: CD4 gate, tissue target, image pattern, diagnostic move, and treatment move.
Cryptococcus neoformans
encapsulated yeastmeningitis
Thick polysaccharide capsule from soil and pigeon droppings.
Inhaled into lungs, then hematogenous spread to meninges.
Indolent fever and headache over weeks, often with increased intracranial pressure.
Best diagnosis: cryptococcal antigen in CSF or serum. India ink can show a clear halo.
Board treatment: amphotericin B plus flucytosine induction, then fluconazole.
Cytomegalovirus
retinitisCD4 50 to 100 range
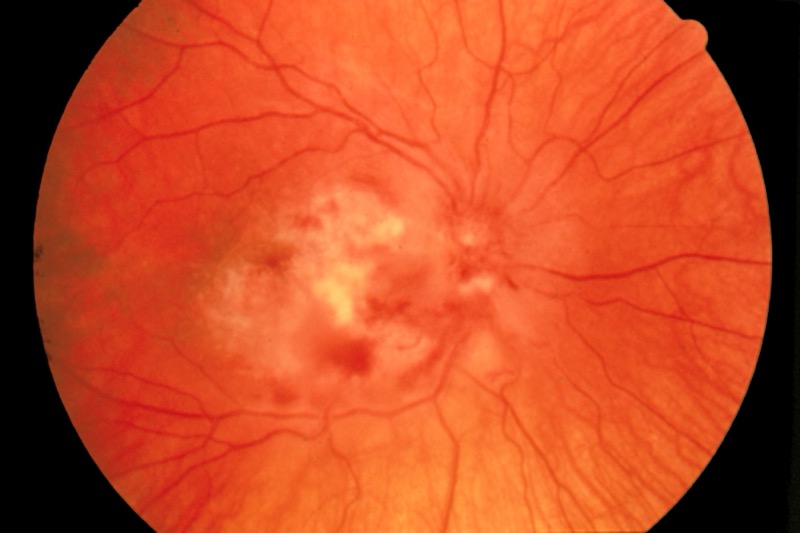
Retinal edema and necrosis with hemorrhage and cotton-wool exudates.
Floaters, blurred vision, visual field loss, or decreased vision.
Classic advanced AIDS threshold is usually below 50, often taught around 50 to 100.
Owl-eye inclusions are the histology memory hook.
Treat with ganciclovir or valganciclovir. Foscarnet is a classic alternative.
Toxoplasma gondii
ringsCD4 below 100
Reactivated latent cysts in advanced HIV cause brain abscesses.
Imaging shows multiple ring-enhancing lesions, often basal ganglia, with edema and mass effect.
Toxo IgG supports reactivation in the right clinical setting.
Active treatment is pyrimethamine plus sulfadiazine plus leucovorin.
Prophylaxis is TMP-SMX when CD4 is below 100 and Toxo IgG is positive.
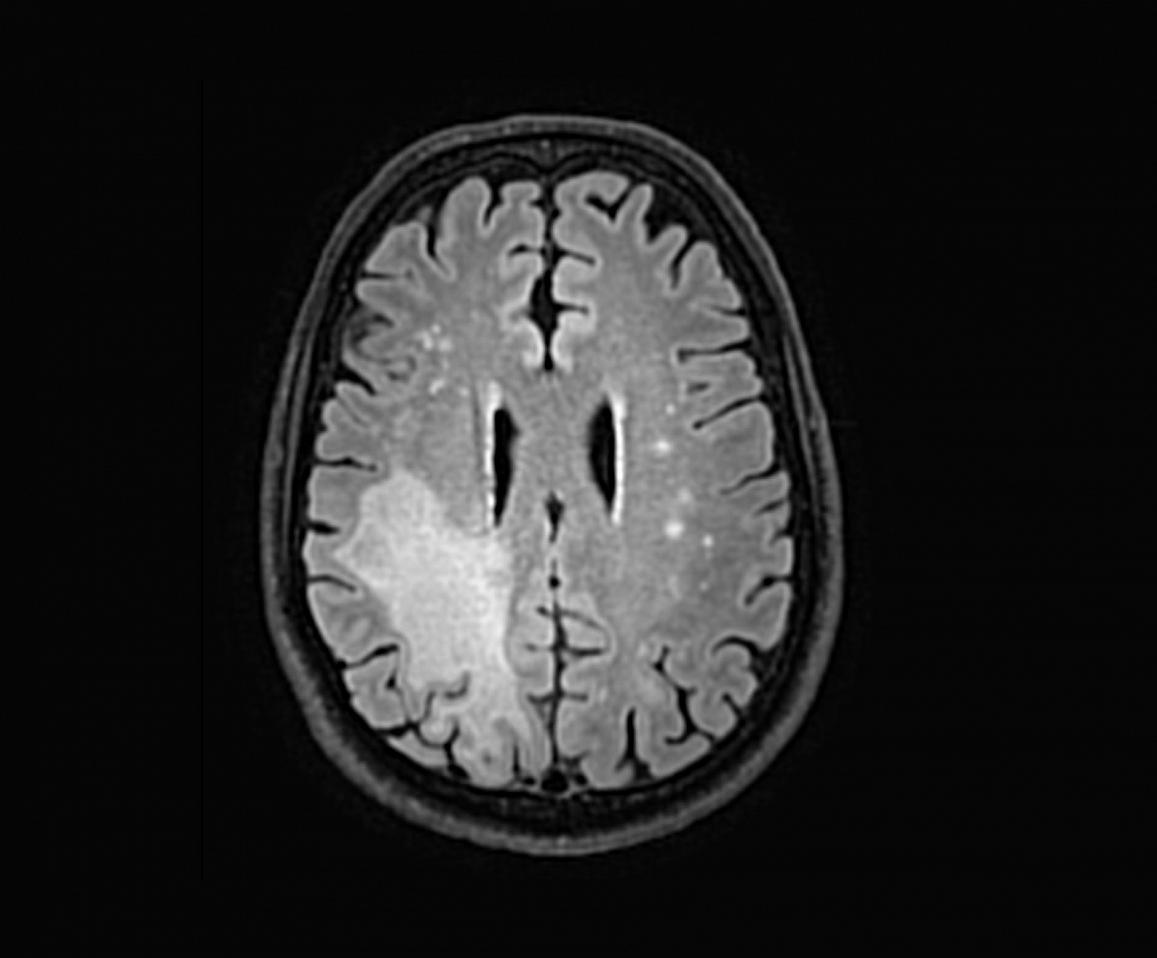
Slow encephalopathy, gait change, weakness, visual symptoms, or focal deficits.
MRI shows nonenhancing white matter lesions without the abscess ring pattern.
Diagnosis: JC virus DNA in CSF, or brain biopsy when needed.
Visual Anchors
The image is not decoration here. It is the shortcut: halo yeast, hemorrhagic retina, ring abscess, white matter plaques.
Crypto halo The capsule is why India ink shows a halo and antigen tests work.CMV retina Floaters plus necrotic hemorrhagic retina points to CMV.Toxo rings Multiple ring-enhancing lesions in AIDS means treat toxo first.PML white matter JC virus demyelination gives white matter disease, not ring abscesses.
CD4 And Imaging Match
Match the clue to the disease, then force the next action. The board loves swapping active treatment with prophylaxis and ring enhancement with demyelination.
Match game
Disease
CD4 Gate
Image Or Exam Pattern
Answer Move
Cryptococcus
Advanced HIV, often below 100
Meningitis, high opening pressure, soap bubble lesions
CrAg test, CT or MRI before LP when pressure signs exist, amphotericin B plus flucytosine
CMV retinitis
Usually below 50, taught around 50 to 100
Floaters, retinal edema, necrosis, hemorrhage
Ganciclovir or valganciclovir, foscarnet alternative
Toxoplasmosis
Below 100
Multiple ring-enhancing lesions with edema
Pyrimethamine, sulfadiazine, leucovorin
PML
Below 200
Nonenhancing white matter lesions, slow focal deficits
JC virus DNA in CSF, immune restoration with ART
Cryptococcus LP Safety
The exam trap is not "never LP." The move is imaging first when the patient has clues that pressure or mass effect could make LP unsafe.
Select the next move
Clinical Walkthrough
One case at a time. Right-click or long-press to cross out a choice. Double-click or double-tap to mark the one you are torn on. The bank shuffles and uses currentOrder never-repeat tracking until the set is spent.