The most potent biological toxin on earth breaks the blue slinkies at the NMJ. Descending flaccid paralysis, three clinical forms, and every board trap that confuses it with tetanus, MG, GBS, and Lambert-Eaton.
A 6-month-old infant is brought to the emergency department with progressive weakness, poor feeding, and constipation for 2 days. The parents report the babysitter recently gave the infant honey on a pacifier. On exam, the infant is hypotonic with a weak cry and diminished deep tendon reflexes.
What is the most likely diagnosis?
Guillain-Barre syndrome
Infant botulism
Werdnig-Hoffmann disease
Myasthenia gravis
Infant botulism = honey exposure + floppy baby + constipation + weak cry. The spores germinate in the immature gut and produce toxin in vivo. This is the most common form of botulism in the US. As soon as you see 6 months and honey, this is the answer.
Explore
Clinical Photos
What Botulism Looks Like
The organism, the food sources, and the clinical signs.
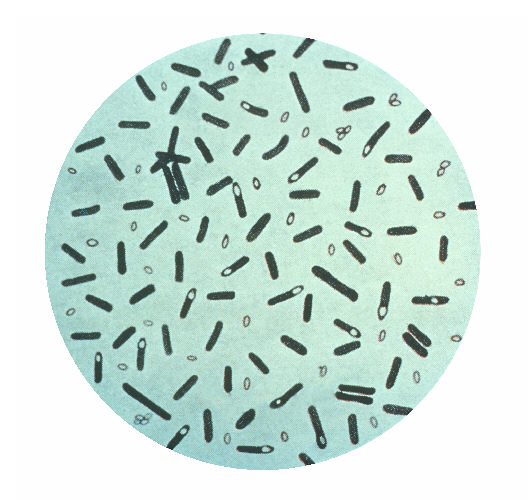
C. botulinum gram stain
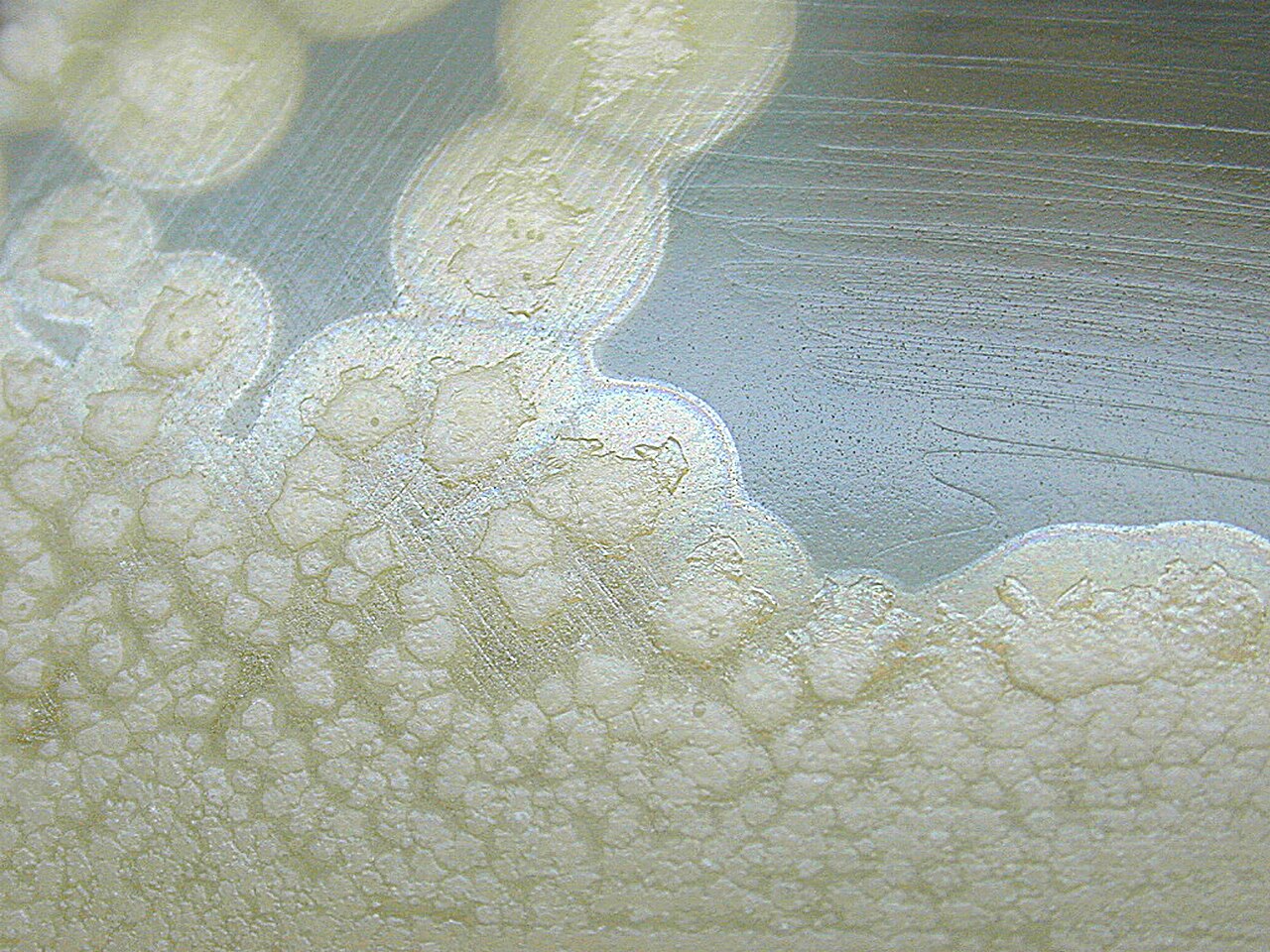
Colony morphology
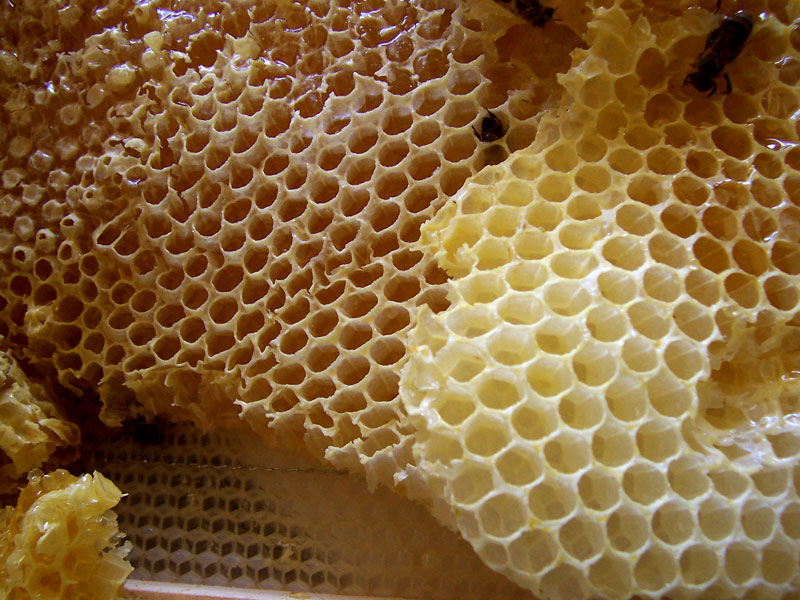
Honey: spore source for infants
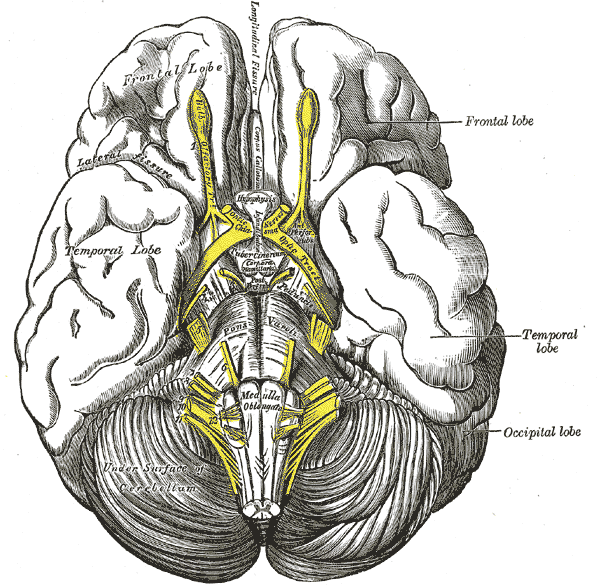
Cranial nerves: paralysis starts here
Canned goods: foodborne source
SNARE Mechanism
Breaking the Blue Slinkies
Tap each numbered element to learn how botulinum toxin blocks ACh release at the neuromuscular junction.
ACh Vesicle
Acetylcholine is packaged into vesicles in the presynaptic terminal. These vesicles must dock and fuse with the presynaptic membrane to release ACh into the synaptic cleft. The docking and fusion process requires SNARE proteins to work.
SNARE Proteins (the Blue Slinkies)
SNARE = Soluble NSF Attachment protein REceptor. Three proteins (synaptobrevin, SNAP-25, syntaxin) form a complex that pulls the vesicle into the membrane so it can fuse and release ACh. Think of them as tiny coiled springs (slinkies) that zip the vesicle down to the membrane. Botulinum toxin is a zinc metalloprotease that cleaves these SNARE proteins. Once broken, the vesicle can never fuse. No fusion = no ACh release = flaccid paralysis.
Botulinum Toxin (BoNT)
The most potent biological toxin known. It is a zinc metalloprotease that specifically cleaves SNARE proteins. Seven serotypes (A through G), with types A, B, and E causing most human disease. Each serotype cleaves a different SNARE protein, but the result is always the same: vesicles cannot fuse, ACh cannot be released, muscles go flaccid.
AChR (Postsynaptic)
The nicotinic acetylcholine receptors on the muscle side are completely normal in botulism. The problem is upstream: no ACh is being released to activate them. This is the key difference from myasthenia gravis, where antibodies attack the receptors themselves (postsynaptic). Botulism = presynaptic. MG = postsynaptic.
The Big Three: Direction of Paralysis
Botulism: Descending flaccid. Toxin blocks ACh at the NMJ (peripheral). Starts at cranial nerves, moves down.
Tetanus: Ascending spastic. Toxin blocks inhibitory neurotransmitters (glycine, GABA) in the spinal cord (central). You inhibit an inhibitor, so you get MORE action. Muscles contract uncontrollably.
GBS: Ascending flaccid. Autoimmune demyelination of peripheral nerves. Starts in the feet, moves up. CSF shows high protein, normal cells (albuminocytologic dissociation).
Forms & DDx
The Three Forms + Board Traps
The toxin, the three clinical presentations, and the comparisons that show up on every clinical practice.
Toxin
Clinical Forms
Board DDx
Floppy Baby
Management
The Organism
Identity:Gram-positiveStains blue/purple with crystal violet. Retains the dye because of its thick peptidoglycan cell wall., obligate anaerobic, spore-forming rod
Spores: Heat-resistant. Survive boiling at 100C. Require 121C (autoclave) to destroy. Found in soil, dust, and honey.
Toxin types: Seven serotypes (A through G). Types A, B, E cause most human disease.
Toxin Mechanism
Target:SNARE proteinsSNARE = Soluble NSF Attachment protein REceptor. Three proteins: synaptobrevin (VAMP), SNAP-25, and syntaxin. They form a coiled complex that pulls the vesicle into the presynaptic membrane for fusion. at the presynaptic terminal of the NMJ
Action: Zinc metalloprotease that cleaves SNARE proteins, preventing ACh vesicle fusion. "It breaks those little blue slinkies. Those are the ones that fuse the vesicle into the membrane. If you break them, you are never going to release that acetylcholine."
Result: No ACh released into the synapse. Flaccid paralysis (lower motor neuron pattern). Mentation always preserved.
Board pearl: Both botulism and tetanus toxins target SNARE proteins. Botulism cleaves SNARE at the NMJ (blocks ACh = flaccid). Tetanus cleaves SNARE in the spinal cord (blocks glycine/GABA = spastic). Same enzyme family, different targets, opposite results.
Infant Botulism (most common in US)
Source: Ingestion of spores (classic: honey). Spores germinate in the immature infant gut and produce toxin in vivo.
Presentation: "Floppy baby" with constipation (earliest sign), weak cry, poor feeding, descending hypotonia. Age typically <1 year.
Treatment: BabyBIG (botulism immune globulin, human-derived). NOT equine antitoxin (risk of serum sickness).
Foodborne Botulism
Source: Ingestion of preformed toxin in improperly preserved food. Classic: home-canned goods, fermented fish, garlic in oil.
Presentation: GI symptoms (nausea, vomiting) followed by descending symmetric paralysis: diplopia, dysphagia, dysarthria, then limb and respiratory weakness.
Treatment: Equine heptavalent antitoxin. Antitoxin FIRST, then intubation if needed. "What is fatiguing him is the toxin. Block more toxin from blocking more release."
Wound Botulism
Source: Spores contaminate a wound, germinate in anaerobic tissue. Classic: black tar heroin injection (skin-popping).
Presentation: Same descending paralysis but NO GI prodrome (toxin enters through the wound, not the gut).
The 4 D's of botulism: Diplopia, Dysphagia, Dysarthria, Dysphonia. All cranial nerve findings. Descending from there. Mentation is always preserved. If the patient is confused, it is NOT botulism.
Botulism vs Tetanus
Botulism:Descending FLACCID paralysis. Blocks ACh release at NMJ (peripheral).
Tetanus:ASCENDING SPASTIC paralysis. Blocks inhibitory neurotransmitters (glycine, GABA) in the spinal cord. "You inhibit an inhibitor. Are you going to get more or less action? Of course, MORE. That is why the muscles contract REAL HARD."
Memory: Botulism = floppy (no signal). Tetanus = rigid (cannot stop the signal).
Botulism vs Myasthenia Gravis
Botulism: Presynaptic (no ACh release). All muscles affected at once. Fixed weakness.
MG: Postsynaptic (anti-AChR antibodies). Fatigable weakness: worse with use, better with rest. Improves with AChE inhibitors.
Key: If edrophonium (Tensilon) test improves symptoms = MG. Botulism will NOT improve (there is no ACh to protect).
Botulism vs GBS
Botulism:Descending paralysis, normal CSF, presynaptic NMJ.
GBS:Ascending paralysis (starts in feet), albuminocytologic dissociation (high protein, normal cells in CSF), demyelination.
Key: Direction is everything. Ascending = GBS. Descending = botulism.
Botulism vs Lambert-Eaton
Botulism: Toxin-mediated. Acute onset. ACh vesicles cannot fuse (SNARE cleaved).
LEMS: Autoimmune (anti-VGCC antibodies). Chronic. Proximal weakness that improves with use. Often paraneoplastic (small cell lung cancer).
Key: Gets WORSE with use = MG. Gets BETTER with use = LEMS. Fixed weakness = botulism.
The floppy baby differential: three causes, ranked. "Hypothyroidism, number one cause of a floppy baby. Number 2 is botulism. Number 3 is Werdnig-Hoffmann."
#1: Hypothyroidism
Clue:Macroglossia (large tongue). "Number one cause of macroglossia."
Other findings: Poor feeding, constipation, prolonged jaundice, large fontanelle, umbilical hernia.
Catch: Newborn screening catches it. If they say "missed on screening" or "born outside US," think congenital hypothyroidism.
#2: Infant Botulism
Clue:Honey + constipation + 6 months old. "As soon as they say 6 months, that is when children get botulism. That is just when people start feeding them canned goods."
Timing: Give BEFORE intubation. "He is fatiguing, but what is fatiguing him is the toxin. Block any more toxin from blocking any more release."
Step 2: Supportive Care
Respiratory: Mechanical ventilation for respiratory failure. Monitor vital capacity.
Nutrition: NG tube or parenteral nutrition if swallowing is impaired.
Recovery: New SNARE proteins must be synthesized. Takes weeks to months.
Wound Botulism Extras
Debridement: Surgical debridement of the infected wound.
Antibiotics: Penicillin or metronidazole (active against anaerobes).
Do NOT give antibiotics for infant botulism: Lysis of bacteria in the gut releases MORE toxin.
Board trap: Why antitoxin before intubation? Because the antitoxin neutralizes circulating toxin and prevents further nerve damage. Intubation is supportive but does not stop the disease from progressing. Stop the toxin FIRST, then manage the airway.
Elimination Game
Eliminate the Imposters
Read the vignette. Reveal clues. Tap the wrong diagnoses to eliminate them.
A 4-month-old infant presents with progressive weakness over 3 days. The parents note the baby has not had a bowel movement in 4 days, has a weak cry, and is unable to latch during breastfeeding. The family recently returned from a rural area where a neighbor gave the baby a taste of honey. On exam, the infant has generalized hypotonia, bilateral ptosis, and absent deep tendon reflexes.
Guillain-Barre
Infant Botulism
Tetanus
Myasthenia Gravis
Werdnig-Hoffmann
Hypothyroidism
Poliomyelitis
Organophosphate
Clue 1: Constipation is the earliest and most consistent sign. GBS starts in the legs and ascends. Tetanus produces rigidity, not flaccidity. Poliomyelitis causes asymmetric paralysis. Organophosphate poisoning causes SLUDGE (salivation, lacrimation, etc.).
Clue 2: Descending pattern (cranial nerves first: ptosis, weak cry, feeding difficulty). MG is fatigable weakness and extremely rare in infants at this age.
Clue 3: Hypothyroidism causes a floppy baby too, but the key finding would be macroglossia. And hypothyroidism does not cause ptosis or acute-onset weakness over days.
Clue 4: Werdnig-Hoffmann has fasciculations and preserves eye movements. No constipation association. This baby has honey exposure + constipation + descending cranial nerve palsies = infant botulism.
Infant Botulism. Spores from honey colonize the immature infant gut. Toxin produced in vivo blocks ACh release. Constipation is the earliest sign, followed by descending cranial nerve palsies and generalized hypotonia. Treatment: BabyBIG, NOT equine antitoxin.
A 32-year-old woman presents with blurred vision, difficulty swallowing, and progressive arm weakness 18 hours after eating home-canned green beans at a potluck dinner. Two other attendees have similar symptoms. On exam, she has bilateral fixed, dilated pupils, symmetric descending weakness, and is alert and oriented.
Organophosphate
Myasthenic crisis
Foodborne botulism
Brainstem stroke
Lambert-Eaton
Tick paralysis
GBS
Diphtheria
Clue 1: Multiple people sick after a shared meal = foodborne illness. Stroke, MG, LEMS, and GBS do not cluster from shared food exposure.
Clue 2: Organophosphate causes SLUDGE and miosis (small pupils). This patient has mydriasis (dilated pupils). Tick paralysis is ascending, not descending.
Clue 3: Diphtheria causes a gray pharyngeal membrane and myocarditis. Does not present as acute descending paralysis from a food source.
Foodborne Botulism. Preformed toxin in improperly canned food. Onset 12 to 36 hours. Fixed dilated pupils from blocked parasympathetic ACh. Treatment: equine heptavalent antitoxin + supportive care. Antitoxin first, then manage the airway.
clinical Walkthrough
25 Clinical Vignettes
Full clinical stems with cause-effect teaching chains. Right-click or long-press to cross out. Double-tap to highlight.
QUESTION 1 OF 25
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 5, 2026 at 8:04 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.