Same chains-in-pairs bug. Two patients at opposite ends of life. Everyone learns the newborn. Almost nobody learns the diabetic adult.
Day 1 to 3 months
Newborn sepsis & meningitis
same bug
The diabetic / elderly adult
Invasive disease
Start here
Start where the trap is
A 71-Year-Old Walks In. Not a Newborn.
A board stem about invasive Group B Strep in an older adult feels like it came from nowhere, because review banks only ever taught you the newborn. Let's fix that in one move.
Mr. Alvarez, 71, with poorly controlled type 2 diabetes, comes to the emergency department with a swollen, hot, red right knee for 2 days and a fever of 38.7°C. He cannot bear weight. Knee arthrocentesis returns cloudy fluid. The Gram stain shows gram-positive cocci in chains, and the lab calls the next morning: the organism is beta-hemolytic, CAMP test positive, hippurate positive, bacitracin resistant, PYR negative.
The reasonable mistake
"Group B Strep? That's a newborn bug. He's 71, so it can't be that." That instinct is exactly what the question is testing. The lab profile above is screaming one organism, and his age is the distractor, not the answer.
Which organism is growing in this man's knee?
Staphylococcus aureus · the usual septic-arthritis suspect
Streptococcus pyogenes (group A) · bacitracin sensitive, PYR positive
Streptococcus agalactiae (group B) · the "newborn" bug
Enterococcus faecalis · PYR positive, grows in bile + salt
It's group B Strep, Streptococcus agalactiae. Walk the lab profile and only one organism fits every line: chains of gram-positive cocci, beta-hemolytic, CAMP positive, hippurate positive, bacitracin resistant, PYR negative. Staph aureus is clusters, not chains, and is catalase positive. Group A Strep is bacitracin SENSITIVE and PYR POSITIVE, the exact opposite of group B on both. Enterococcus is PYR positive too. The age was bait. The real signal is the diabetes: diabetes is the number-one host factor for invasive group B Strep in adults. Lock this in now and the rest of the page is just filling in the picture.
Bottom line: GBS is a newborn bug AND a diabetic-adult bug. When the lab says CAMP positive in a diabetic, his age does not save the wrong answer.
Tell the lookalikes apart
The Lab Lineup: GBS vs Group A vs Enterococcus
All three are gram-positive cocci that can grow in chains. Four tests pull them apart. Tap each suspect to run its panel.
Gram +Cocci · chainsCatalase −Group B (Lancefield)
📷 Chains of gram-positive cocci. This chaining morphology is what puts GBS in the strep family. Tap to enlarge.
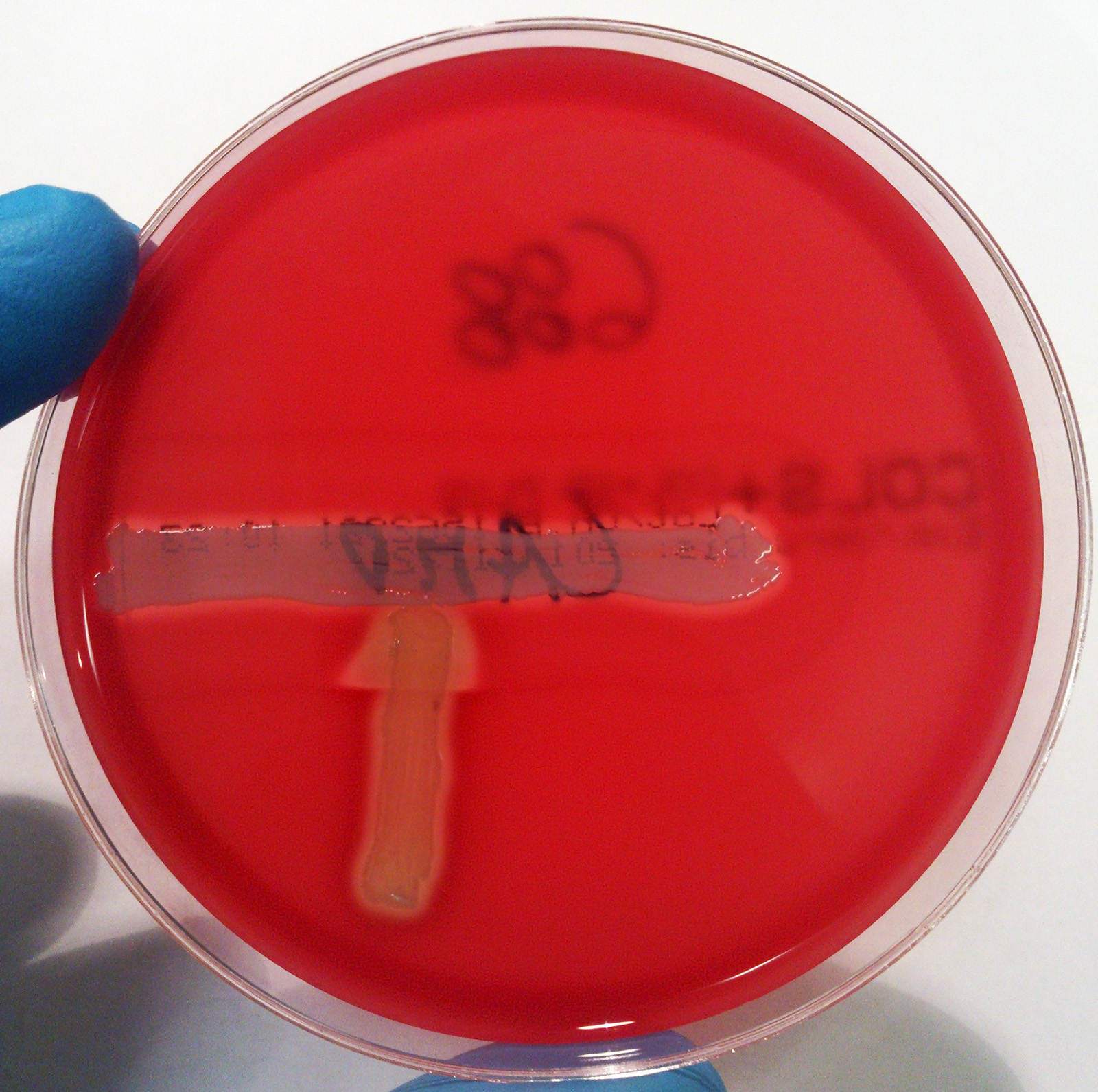
🎯CAMP testPOSITIVE. Makes an arrowhead of enhanced hemolysis pointing at a streak of Staph aureus. The arrow points to GBS.🔑The CAMP arrow points to GBS. If you see the arrowhead, the answer is group B.
✅HippuratePOSITIVE. Hydrolyzes hippurate. Classic GBS confirmatory test alongside CAMP.
🚫BacitracinRESISTANT. Grows right up to the bacitracin disc. (Group A is killed by it.)
❌PYRNEGATIVE. No color change. (Group A and Enterococcus are positive.)
💧HemolysisBeta-hemolytic with a narrow zoneThe clear hemolytic ring is small. Group A makes a wider, more dramatic beta zone. The narrow zone is a quiet GBS clue. on blood agar.
GBS fingerprint: CAMP +, hippurate +, bacitracin resistant, PYR negative. It is the one beta-hemolytic strep that is bacitracin resistant and PYR negative.
📷 Beta-hemolysis on blood agar: complete clearing of red cells, classically a narrower zone than group A. Tap to enlarge.📷 The positive CAMP test: an arrowhead of enhanced hemolysis where GBS meets the Staph aureus streak. The arrow points to GBS. Tap to enlarge.
❌CAMP testNegative. No arrowhead.
❌HippurateNegative.
✅BacitracinSENSITIVE. A zone of no growth around the bacitracin (A) disc. This is the classic group A test.
✅PYRPOSITIVE. Turns bright red. Group A is PYR positive.
💧HemolysisBeta-hemolytic with a wide, clean zone.
Group A is the mirror image of GBS: bacitracin SENSITIVE, PYR POSITIVE. Group B is resistant and negative. Opposite on both.
❌CAMP testNegative.
✅PYRPOSITIVE. Like group A, Enterococcus is PYR positive.
🧤Bile esculinGrows in bile. Blackens bile-esculin agar.
🌊6.5% NaClGrows in 6.5% salt. The salt-and-bile combo is the Enterococcus signature.
💧HemolysisUsually gamma (non-hemolytic) or alpha. Not classically beta.
Enterococcus signature: PYR positive, grows in bile + 6.5% NaCl. It survives the gut and the salt. GBS does neither of those tricks.
Run the CAMP image in the photo strip later and you will see the literal arrowhead. The whole lineup collapses to one habit: CAMP arrow = GBS, and remember it is the opposite of group A on bacitracin and PYR.
Own the half everyone teaches
Neonatal GBS: Early vs Late Onset
The newborn catches it from the mother's genital and GI tract during delivery. Timing splits the picture into two syndromes. Tap to compare.
Early-onset
First week of life
Late-onset
1 week to 3 months
Early-onset hits in the first week of life, often within the first 24 hours.
Picture: sepsis and pneumonia. The baby is sick fast, sometimes in the delivery room, with respiratory distress and shock.
Source: vertical transmissionThe baby passes through a colonized birth canal. Mom's rectovaginal GBS gets aspirated or seeds the infant during delivery. This is why intrapartum antibiotics work: they cut the dose the baby meets. during delivery from a colonized mother.
Late-onset shows up from 1 week to 3 months of age.
Picture: meningitis and bacteremia. Think the febrile, irritable, poorly feeding infant with a bulging fontanelle.
Source can be the delivery or later environmental exposure, so intrapartum prophylaxis does NOT fully prevent late-onset disease.
📷 The neonatal host. Babies acquire GBS from a colonized birth canal; prematurity raises the risk. Tap to enlarge.
Prevention: the maternal screen
Pregnant patients get a rectovaginal screening culture at 36 to 37 weeks. A positive screen, or any risk factor, triggers intrapartum penicillin (or ampicillin) during labor.🔑Screen at 35 to 37 weeks, treat during labor, not before. The antibiotic is for the baby's passage, so it has to be on board when the baby comes through.
PrematurityPreterm delivery raises risk.
Membranes > 18 hrProlonged rupture of membranes.
Intrapartum feverMaternal fever in labor.
GBS bacteriuriaGBS in urine this pregnancy.
Prior GBS infantA previous baby with invasive GBS.
Any one of these, even with an unknown or pending screen, is enough to give prophylaxis. A prior infant with invasive GBS means treat, no screen needed.
The under-taught half
The Diabetic Adult: Invasive GBS
This is the part the banks skip. In an adult, GBS is a real cause of invasive disease, and diabetes is the headline.
The number-one host factor for invasive GBS in adults is diabetes mellitus. The high-sugar, poorly-perfused host is the open door.
📷 An infected diabetic foot ulcer: a classic adult GBS soft-tissue site, since diabetes is the #1 host factor. Tap to enlarge.
Treatment: penicillin or ampicillin is first line. Add gentamicinThe aminoglycoside gives synergy for serious infection, classically endocarditis. GBS stays reliably penicillin-susceptible, so the penicillin backbone almost never changes. for serious disease such as endocarditis. For a penicillin allergy: a cephalosporin or vancomycin depending on severity.
The teaching point in one line: GBS is not just a newborn bug. In a diabetic or elderly adult, it is a legitimate cause of cellulitis, a hot joint, bacteremia, and more.
Play it both directions
Two Patients, One Bug
A newborn and an elderly diabetic both grow the same chains-in-pairs organism. Work each one from opposite ends of life to the same diagnosis.
The same plate, two lives
One Organism
Two patients are admitted the same night. A newborn and a 71-year-old with diabetes. Both blood cultures grow the identical bug: gram-positive cocci in chains, beta-hemolytic, CAMP positive. Work both to the diagnosis.
Chapter I · First 24 hours
Baby Rosa
Born at 35 weeks. Mother's membranes were ruptured 22 hours. At 18 hours of life Rosa is grunting, tachypneic, and mottled. The blood culture is growing the bug.
Which neonatal syndrome is this?
Chapter II · Opposite end of life
Mr. Alvarez
71, type 2 diabetes, HbA1c 10.4%. Hot swollen knee, cannot bear weight, fever. Joint fluid grows the same bug. What single host factor most explains why GBS landed in him?
The number-one adult host factor here is:
Chapter III · Same lab, both ends
The Shared ID
Both plates ran identical. One result nails it down and tells group B apart from group A. Pick the lab line that confirms Streptococcus agalactiae.
PearlB is for Baby and Blood sugar. The age never rules GBS out
Both ends of life, one organism. You worked it both directions.
Decide on test day
The GBS Decision Tool
Guess each branch before it opens. The goal is a reflex you can run under pressure.
A beta-hemolytic, gram-positive coccus in chains grows from a sterile site. You need to name it.
Step 1: It is bacitracin RESISTANT and PYR NEGATIVE. Group A or group B?
Group B (S. agalactiae)
Group A (S. pyogenes)
Yes. Group B is bacitracin resistant and PYR negative. Group A is the opposite on both: sensitive and positive.
Flip it. Group A is bacitracin SENSITIVE and PYR POSITIVE. Resistant + negative is the group B signature. Group A is positive on both, group B is negative on both.
→ Bacitracin resistant + PYR negative = group B
→ CAMP positive and hippurate positive confirm it
You have group B Strep. Now: who is the patient?
Step 2: It is a 70-year-old diabetic with a hot knee. Does the age rule GBS out?
No. Diabetes is the #1 adult host factor
Yes. GBS only affects newborns
Right. GBS is a genuine adult invasive pathogen, and diabetes is the leading host factor. Septic arthritis, cellulitis, and bacteremia all fit.
That's the trap. "Newborn only" is the misconception the exam baits with. In a diabetic adult, GBS causes invasive disease. Age never rules GBS out.
→ Newborn: early-onset sepsis or late-onset meningitis
→ Diabetic / elderly adult: cellulitis, hot joint, bacteremia
You confirmed invasive group B Strep. Treatment time.
Step 3: First-line drug?
Penicillin or ampicillin
Vancomycin for everyone
Yes. GBS stays reliably penicillin-susceptible. Add gentamicin for serious disease like endocarditis. Vancomycin or a cephalosporin is the penicillin-allergy backup.
Save the vanc. Vancomycin is the backup for penicillin allergy. GBS is reliably penicillin-susceptible, so penicillin or ampicillin is first line. Penicillin first, vancomycin only if allergic.
→ Penicillin / ampicillin first line
→ Add gentamicin for endocarditis / serious disease
→ Cephalosporin or vancomycin if penicillin-allergic
Stick the landing
Memory Hooks
Tap to reveal. Pick whichever one sticks.
Who gets itWhat two groups does group B Strep hit?
"B is for Baby and for Blood sugar." Group B Strep hits newborns and diabetic adults.
tap to reveal
Lab signatureWhat is the four-test GBS fingerprint?
The nameWhy does agalactiae help you remember the hosts?
"Agalactiae = no milk." Think the pregnant and postpartum and newborn axis first, then remember the diabetic adult too.
tap to reveal
A vs BHow do you keep group A and group B from blurring?
"Group A is PYR positive and bacitracin sensitive. Group B is the opposite on both." A is positive, B is negative.
tap to reveal
Board-style walkthrough
Clinical Walkthrough
Original vignettes, one at a time, shuffled, never repeating until the bank is exhausted. Right-click or long-press a choice to cross it out. Double-click or double-tap to highlight. Every option gets explained.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last reviewed June 2026
References: Murray Medical Microbiology, Levinson Review of Medical Microbiology and Immunology, Mandell Principles and Practice of Infectious Diseases.