Every one of these has appeared in clinical practice.
Butterfly (Malar) Rash → SLE
BUZZWORD Erythematous rash across both cheeks, sparing the nasolabial folds
- Spares nasolabial folds · this is the key differentiator from rosacea (which doesn't spare them)
- Photosensitive · worsens with sun exposure
- Part of the SLE diagnostic criteria (need 4 of 11)
- Other SLE skin: discoid lupus (scarring), oral ulcers (painless)
Board trap: Rosacea also causes facial erythema but does NOT spare nasolabial folds and has papules/pustules without the systemic features. Don't confuse them.
🔑The butterfly lands on the cheeks but its body doesn't touch the nose creases · SLE spares the nasolabial folds
Target Lesions → Erythema Multiforme
BUZZWORD Three concentric color zones: dark center, pale ring, red outer ring
- #1 cause: HSV (herpes simplex) · NOT drugs
- Acral distribution (hands, feet, palms, soles)
- EM minor = just skin. EM major = skin + mucous membranes
- Self-limited · treat the HSV, not the EM
Board trap: SJS/TEN are NOT just "severe EM." They're separate diseases, usually drug-induced. EM = HSV. SJS = drugs (sulfonamides, phenytoin, allopurinol, carbamazepine, lamotrigine). Don't merge them.
🔑Herpes hits the bullseye · HSV causes target lesions (EM), NOT drugs
Herald Patch → Pityriasis Rosea
BUZZWORD Single large oval scaly patch followed days later by smaller lesions in a "Christmas tree" pattern on the back
- Herald patch comes first (the "herald" announces the army)
- Smaller lesions follow the skin cleavage lines → Christmas tree on back
- Associated with HHV-6 and HHV-7
- Self-limited over 6-8 weeks, no treatment needed
- Young adults, common in spring/fall
Board trap: Secondary syphilis can mimic this pattern. Always get an RPR/VDRL if the "Christmas tree" rash involves the palms and soles · pityriasis rosea does NOT.
Dew Drops on Rose Petals → Varicella
BUZZWORD Clear vesicles on an erythematous base, lesions in different stages simultaneously
- Different stages at once = pathognomonic (macules, papules, vesicles, crusts all present)
- Starts on trunk, spreads centrifugally
- Vs smallpox: all lesions in the SAME stage, starts on face/extremities and spreads centrifugally (periphery outward)
- Complication in adults: varicella pneumonia
- Complication in kids on aspirin: Reye syndrome
🔑A garden has flowers in every stage · buds, blooms, and wilting all at once. That's varicella's "different stages."
Nikolsky Sign (+) → Pemphigus Vulgaris
BUZZWORD Gentle lateral pressure on normal-appearing skin causes the epidermis to separate and slough off
- Pemphigus vulgaris: Nikolsky (+), flaccid blisters, intraepidermal (superficial split)
- Antibodies against desmoglein 3 (desmosome component)
- Oral mucosa involved FIRST in most patients
- Vs bullous pemphigoid: Nikolsky (−), tense blisters, subepidermal (deeper split)
- Pemphigoid: antibodies against hemidesmosome proteins BP180 and BP230, elderly patients, pruritic
Pemphigus = superficial = flaccid = falls apart easily (Nikolsky +)
Pemphigoid = deep = tense = holds together (Nikolsky −)
🔑PemphiGUS is flacc-GUS (flaccid). PemphiGOID is ten-GOID (tense). The superficial one falls apart.
Silvery Scales + Auspitz Sign → Psoriasis
BUZZWORD Well-demarcated erythematous plaques with silvery-white scales; scraping reveals pinpoint bleeding (Auspitz sign)
- Extensor surfaces: elbows, knees, scalp, sacrum
- Nail pitting is classic (also: oil spots, onycholysis)
- Koebner phenomenon: lesions appear at sites of trauma/injury
- Histology: Munro microabscesses, parakeratosis, epidermal hyperplasia
- Associated with psoriatic arthritis (DIP joints, dactylitis, pencil-in-cup deformity)
Board trap: Guttate psoriasis in a young patient after strep pharyngitis · small "drop-like" lesions. Treat the strep, the psoriasis often resolves.
🔑Silver scales reveal a bloody surprise underneath · that's Auspitz. Like scraping frost off a red car.
Gottron Papules + Heliotrope Rash → Dermatomyositis
BUZZWORD Purple papules over MCP/PIP joints (Gottron) + purple-lilac eyelid discoloration (heliotrope)
- Proximal muscle weakness + elevated CK
- Anti-Jo-1 antibodies (antisynthetase syndrome)
- Anti-Mi-2 (classic DM), anti-MDA5 (amyopathic DM)
- Shawl sign: V-shaped photodistributed rash on upper back/chest
- Screen for malignancy · ovarian, lung, GI cancers in adults with new-onset DM
Board trap: clinical medicine loves asking: "What screening test should you order in a 55-year-old with new dermatomyositis?" → Age-appropriate cancer screening. The DM is paraneoplastic (meaning a hidden tumor elsewhere is triggering the immune attack -- the cancer is the real culprit) until proven otherwise.
Cafe-au-Lait Spots → Neurofibromatosis Type 1
BUZZWORD ≥6 cafe-au-lait spots >5mm (prepubertal) or >15mm (postpubertal)
- NF1 diagnostic criteria (need 2+): cafe-au-lait spots, neurofibromas (≥2), axillary/inguinal freckling, optic glioma, Lisch nodules (iris hamartomas), osseous lesion, first-degree relative
- Chromosome 17, neurofibromin gene (tumor suppressor)
- Autosomal dominant
- Risk of malignant peripheral nerve sheath tumors
NF1 = Von Recklinghausen = chromosome 17 (17 letters in "von Recklinghausen")
NF2 = bilateral acoustic neuromas = chromosome 22 (22 = 2 tumors, 2 ears)
Ash-Leaf Spots → Tuberous Sclerosis
BUZZWORD Hypopigmented macules best seen under Wood lamp (UV light)
- Classic triad: seizures, intellectual disability, angiofibromas (adenoma sebaceum)
- Other skin: shagreen patches (leathery plaques on lower back), periungual fibromas
- Cardiac rhabdomyomas (in neonates · most common cardiac tumor in infants)
- Renal angiomyolipomas, cortical tubers (brain)
- TSC1 (hamartin) or TSC2 (tuberin) · tumor suppressors
🔑Ash leaves fall on a shagreen couch near an angel (angiofibroma) while the baby's heart grows muscle (rhabdomyoma)
Koebner Phenomenon → Psoriasis / Lichen Planus / Vitiligo
BUZZWORD New lesions appearing at sites of skin trauma (scratches, surgical scars, tattoos)
- The Big 3 that Koebner: Psoriasis, Lichen planus, Vitiligo
- Also seen in: molluscum contagiosum, warts, lichen nitidus
- Isomorphic response = same as Koebner (different name, same concept)
- clinical medicine tests this as: "patient develops new psoriatic plaques along a recent surgical scar"
Darier Sign → Mastocytosis
BUZZWORD Rubbing a skin lesion causes urtication (wheal and flare) due to mast cell degranulation
- Urticaria pigmentosa = most common form in kids (brown-red macules/papules)
- Systemic mastocytosis: flushing, diarrhea, hypotension, hepatosplenomegaly
- Elevated serum tryptase
- Histology: increased mast cells (toluidine blue or Giemsa stain, metachromatic granules)
Dermatitis Herpetiformis → Celiac Disease
BUZZWORD Intensely pruritic grouped vesicles on extensor surfaces (elbows, knees, buttocks)
- "Herpetiformis" = looks like herpes (grouped vesicles) but is NOT herpes
- IgA deposits at dermal papillae on immunofluorescence
- Anti-tissue transglutaminase (anti-tTG) antibodies = same as celiac
- Treatment: dapsone (rapid relief) + gluten-free diet
- Most patients have celiac disease, even if asymptomatic GI
Board trap: clinical medicine shows you "grouped vesicles" and wants you to say herpes. But if it's on elbows/knees/buttocks bilaterally and the patient has diarrhea/malabsorption → dermatitis herpetiformis, NOT HSV.
🔑Herpes-looking bumps on gluten-sensitive skin · the gut is leaking and the skin is screaming about it. IgA at the scene of the crime.
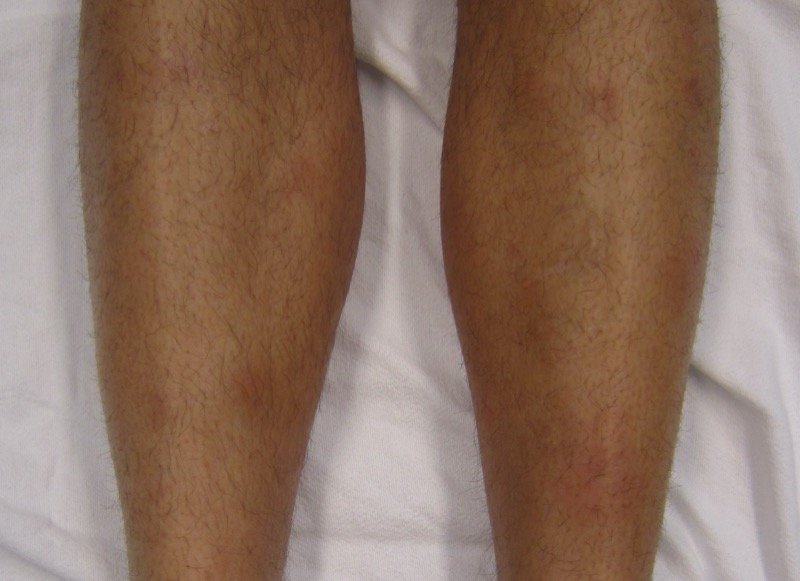
Erythema Nodosum → Sarcoidosis / IBD / Infection
BUZZWORD Tender, red nodules on the anterior shins (panniculitis of the subcutaneous fat)
- Most common causes: sarcoidosis, IBD (especially Crohn's), strep pharyngitis, OCPs, sulfonamides
- Septal panniculitis · inflammation of fat septae, NO vasculitis
- Self-limited · treat the underlying cause
- Biopsy: Miescher radial granulomas in the septae
Erythema nodosum = septal panniculitis = shins
Erythema induratum = lobular panniculitis = calves (posterior) = think TB
Palpable Purpura → Leukocytoclastic Vasculitis / IgA Vasculitis
BUZZWORD Non-blanching, raised, purplish lesions on lower extremities
- "Palpable" = raised = vasculitis until proven otherwise
- In a child: IgA vasculitis (HSP) · palpable purpura + abdominal pain + arthralgia + hematuria
- IgA deposits in skin and kidney (IgA nephropathy component)
- In adults: drug reaction, infection, or autoimmune vasculitis
- Non-palpable purpura = thrombocytopenia, not vasculitis
Board trap: clinical medicine shows a child with purpura on the legs/buttocks after a URI. If they say low platelets → ITP. If platelets are normal → IgA vasculitis (HSP). The platelet count is the branch point.
Iris Lesion + Oral Ulcers → Stevens-Johnson / Behcet's
SIGN OVERLAP These two get confused because both involve mucous membranes
- SJS: Drug-induced (sulfa, phenytoin, allopurinol, carbamazepine, lamotrigine). Epidermal detachment <10% BSA. Atypical target lesions. Nikolsky (+).
- TEN: Same as SJS but >30% BSA detachment. Medical emergency. Mortality 25-35%.
- Behcet's: Recurrent oral + genital ulcers + uveitis. HLA-B51. Silk Road countries. Pathergy test (+).
- SJS/TEN is acute and drug-related. Behcet's is chronic and autoimmune.
SJS/TEN = drugs = acute = skin falls off
Behcet's = autoimmune = chronic = ulcers recur + eye inflammation
Shawl Sign + Mechanic's Hands → Dermatomyositis
BUZZWORD V-shaped photodistributed rash + hyperkeratotic, cracked skin on fingertips
- Shawl sign = rash draped across upper back/shoulders like a shawl
- Mechanic's hands = rough, cracked, hyperkeratotic lateral fingers (antisynthetase syndrome)
- Anti-Jo-1 is the antibody for antisynthetase syndrome
- Antisynthetase syndrome: mechanic's hands + ILD + myositis + arthritis + Raynaud's + fever
Honey-Crusted Lesions → Impetigo
BUZZWORD Golden/honey-colored crusts on an erythematous base, usually perioral in children
- Non-bullous impetigo (70%): S. aureus or GAS → honey crusts
- Bullous impetigo: S. aureus exfoliative toxin → flaccid bullae
- Complication of GAS impetigo: post-strep glomerulonephritis (NOT rheumatic fever · skin strep doesn't cause RF)
- Treatment: topical mupirocin (mild), oral cephalexin (extensive)
Board trap: Impetigo caused by GAS can cause PSGN but NOT rheumatic fever. Only pharyngeal GAS causes RF. Skin GAS = nephritis risk only.
🔑The skin strep can hit the kidney (PSGN) but NOT the heart (RF). Only the throat strep breaks hearts.
Scarlatiniform Rash + Strawberry Tongue → Scarlet Fever
BUZZWORD Sandpaper-textured diffuse erythematous rash, red tongue with prominent papillae, pastia lines
- Caused by GAS erythrogenic toxin (superantigen)
- Follows GAS pharyngitis (NOT skin infection)
- Pastia lines: linear petechiae in skin folds (axillae, antecubital)
- Circumoral pallor (pale around the mouth)
- Desquamation during recovery (starts at fingertips)
Slapped Cheek → Erythema Infectiosum (Fifth Disease)
BUZZWORD Bright red facial erythema ("slapped cheeks") followed by lacy/reticular rash on trunk and extremities
- Parvovirus B19 (ssDNA virus, smallest DNA virus)
- Infects erythroid precursors → temporary halt in RBC production
- Dangerous in sickle cell: aplastic crisis (reticulocyte count drops to zero)
- Dangerous in pregnancy: hydrops fetalis
- Dangerous in immunocompromised: pure red cell aplasia
Board trap: Sickle cell patient with sudden Hb drop + low reticulocytes → parvovirus B19 aplastic crisis. NOT vaso-occlusive crisis (that doesn't drop reticulocytes).
Skin Cancer Triad: BCC vs SCC vs Melanoma
HIGH-YIELD COMPARISON
- BCC: Most common skin cancer. Pearly, translucent papule with telangiectasias and rolled borders. Sun-exposed areas. Almost NEVER metastasizes. Upper lip.
- SCC: Second most common. Scaly, ulcerated nodule. Can metastasize. Arises from actinic keratoses. Lower lip. Associated with immunosuppression.
- Melanoma: Most deadly. ABCDE criteria (Asymmetry, Border irregularity, Color variation, Diameter >6mm, Evolving). Breslow depth = most important prognostic factor.
BCC = upper lip (the "better" location · locally invasive but almost never metastasizes)
SCC = lower lip (the "worse" location · it can spread)
Melanoma = Breslow depth determines prognosis and management
🔑BCC is on top (upper lip) and stays put. SCC is on the bottom (lower lip) and can drop down to lymph nodes. Melanoma goes deep.