DERM · PRE-MALIGNANT LESIONS
The sun's receipt. Years of UV damage, stored as a rough scaly patch on sun-exposed skin. Ignore it and it might cash in as squamous cell carcinoma.
☀️ ROUND ONE
Don't look at the answer yet. Just read.
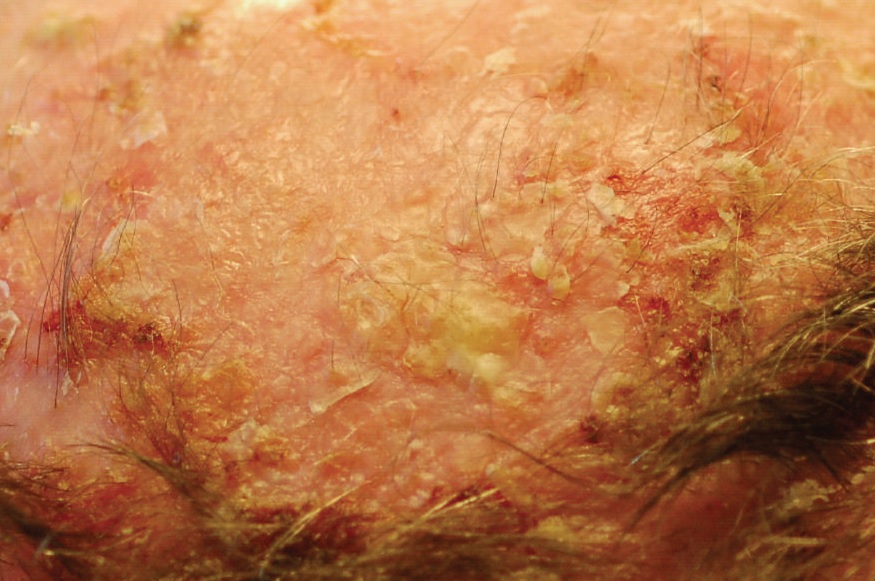
A 66-year-old landscaper comes in with a 4-month history of recurrent crusty patches on the backs of his hands. He describes them as rough, like sandpaper with a peeling, adherent scale that comes back whenever he picks it off. Occasionally they itch and burn. He's worked outdoors without sunscreen for 30 years.
Photograph shows multiple erythematous patches with an adherent yellowish-white scale, concentrated on the dorsal hands. No rolled edges, no pearly border, no dark pigment.
What's the most likely diagnosis, and what's the one thing you don't want to miss about it?
The answers are woven into everything below. Keep going and earn them.
📚 THE BASICS
Start here before anything else
Actinic keratosis (AK) is a pre-malignantNot cancer yet. But it's standing in the cancer waiting room. The cells are abnormal but haven't punched through the basement membrane yet. skin lesion caused by cumulative UVB radiation damage to keratinocytes.
Think of it like this: every unprotected sun exposure is a tiny mutation stored in your DNA. After 30 years of landscaping without sunscreen, those mutations pile up. AK is the skin's way of saying "the bill is coming due."
The key word is cumulative. This isn't about one bad sunburn. This is decades of UV exposure quietly damaging the same keratinocytes on the same sun-exposed areas, over and over, until the DNA can't keep up.
⚙️ THE MECHANISM
p53 is what catches and fixes DNA errors. UV breaks it.
UVB radiation causes a very specific type of DNA damage: it fuses adjacent thymine bases together (called pyrimidine dimersTwo adjacent thymines (T-T) stuck together by UV energy. The DNA proofreader can't read it correctly. If p53 is also broken, the cell divides with this error baked in.). Normally your cells catch these errors using p53Tumor suppressor gene. When DNA is damaged, p53 STOPS the cell from dividing until repairs are made. Or, if damage is too severe, p53 tells the cell to self-destruct (apoptosis). Break p53 and you remove the brake pad entirely..
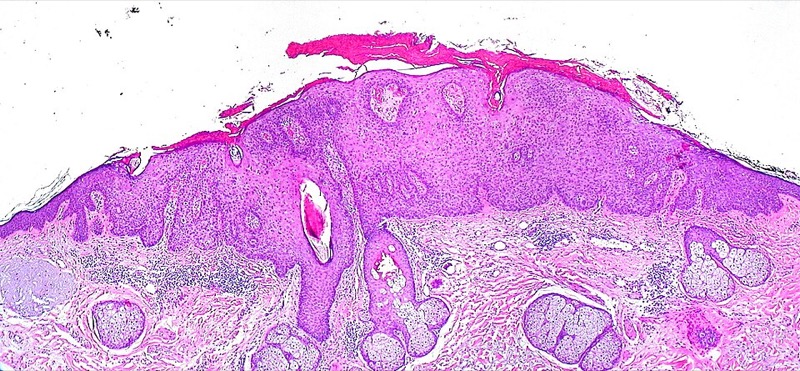
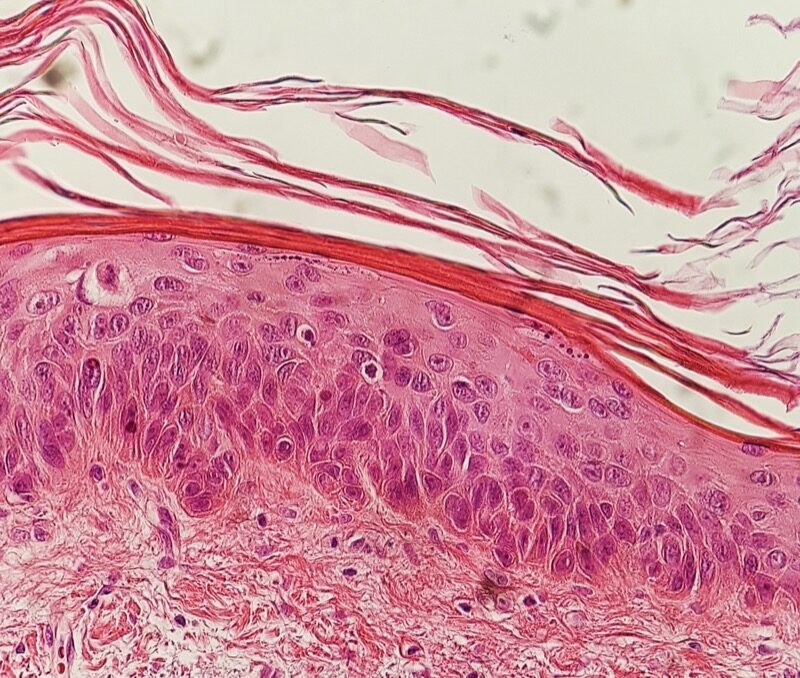
Here's the problem: UVB also mutates p53 itself. So you get damaged DNA AND no editor to catch it. The cell divides. The daughter cells have the same mutation. This keeps happening for years until you get a clonal population of dysplastic keratinocytes sitting in the epidermis.
That clonal dysplastic population is the actinic keratosis.
🧬 The AK-to-SCC Story in One Chain
👨🏭 WHO GETS IT
The profile is very specific
| Risk Factor | Why It Matters | Board Clue |
|---|---|---|
| Chronic sun exposure | Cumulative UVB damage over years (not single burn) | Outdoor worker, farmer, landscaper, sailor |
| Fair skin (Fitzpatrick I-II) | Less melanin = less UV protection | Blue/green eyes, light hair, burns easily |
| Immunosuppression | Immune surveillance fails, dysplastic cells aren't cleared | Transplant patient on tacrolimus, HIV |
| Age >60 | Decades of accumulated UV damage | Combined with outdoor work = highest risk |
| Prior AK or skin cancer | Same UV-damaged field produces more lesions | Field cancerization (covered below) |
👀 HOW IT LOOKS
clinical practice test recognition. Know the feel.


AK has a signature feel that earns it the nickname "sandpaper skin." The findings are:
| Feature | Description | The Clue |
|---|---|---|
| Texture | Rough, gritty, sandpaper-like | You can FEEL it before you see it in clinical practice |
| Scale | Adherent yellowish-white scale that recurs when removed | "Comes back every time I pick it off" |
| Base | Erythematous (red) base underneath the scale | Remove scale → bleeding/red base = positive "flag sign" |
| Size | Usually <1 cm | Multiple lesions common, not just one |
| Location | Sun-exposed areas: dorsal hands, face, scalp, ears, forearms, lips | NEVER on covered skin |
| Symptoms | Pruritus (itching), occasional burning/stinging | Usually mild; painless unless irritated |
🖼️ THE BIG PICTURE
Why treating one lesion isn't enough
Field cancerizationSlaughter's concept (1953): chronic carcinogen exposure (like UV) doesn't damage just one cell. It damages an entire field of cells in the exposed area. Multiple independent pre-malignant lesions develop across the field simultaneously. is the concept that explains why patients with one AK almost always have many. The entire sun-exposed area has been damaged by UV, not just the spot where the AK appeared.
Think of it like this: if you spill bleach on a carpet, the whole area is damaged, not just the visible stain. Treating only the visible AK without addressing the surrounding field leaves dozens of future lesions ready to emerge.
This is why dermatologists often use field therapy (5-FU cream, imiquimod) that treats the entire visible area, not just spot-treating each AK one by one. You have to treat the whole carpet, not just the stain you can see.
🌈 THE SPECTRUM
Tap each event to see what's happening at the cellular level
🔍 TRAIN YOUR EYE
4 suspects walked into the clinic. Use the clues to eliminate the imposters.
A patient has a rough, sandpaper lesion on sun-exposed skin. These 4 diagnoses are on your differential. Use each clue to eliminate one at a time. Last one standing is the answer.
🤖 KNOW YOUR LOOKALIKES
These get confused in clinical practice. Know the key pattern for each.
| Condition | Key Differentiator | key pattern |
|---|---|---|
| AK | Rough sandpaper texture, erythematous base, sun-exposed, adherent scale | The feel is the clue. If it's rough and scaly on a sun-damaged area, it's AK until proven otherwise. |
| SCC | Ulcerates, indurated, bleeds without provocation, bigger, faster growing | AK doesn't bleed on its own. Bleeding = biopsy = SCC until proven otherwise. |
| BCC | Pearly translucent nodule with rolled ("rodent") border and telangiectasias. Doesn't feel rough. | BCC is smooth and shiny. AK is rough and scaly. If you feel glass vs sandpaper, you know which is which. |
| Bowen's Disease | Well-defined, erythematous plaque. Full-thickness dysplasia (in situ SCC). On trunk, not just sun-exposed. | Bowen's is SCC in situ (full-thickness). AK is partial thickness dysplasia. Bowen's also hits non-sun-exposed sites like trunk and genitals. |
| Seborrheic Keratosis | "Stuck-on" waxy, verrucous appearance. Not always sun-exposed. Benign. Well-defined. | Seb K is stuck ON the skin like someone applied it with glue. AK is IN the skin. Also: seb K is not pre-malignant, AK is. |
| Psoriasis | Silver/white THICK scale. Symmetric. Extensor surfaces (elbows, knees). Auspitz sign positive. Systemic associations. | Psoriasis is symmetric on elbows and knees. AK is asymmetric on sun-exposed areas. Nobody gets psoriasis "only on the dorsal hands" from being a landscaper. |
VILLAIN CARDS
Tap a card to flip it.
🎯 PROVE IT
5 patients. All solar-damaged. Read the stem, commit, then check the explanation.
📋 THE PLAN
Answer before you see the branch. It's the only way to learn it.
AK treatment depends on whether you're treating one visible lesion or the whole field. These require different approaches.
Decision branch: For isolated discrete AK → Cryotherapy. For widespread field with multiple AKs → 5-FU cream or Imiquimod (field treatment). For recurrent or complex cases → PDT. Bottom line: spot = cryo; field = topical therapy.
💉 TREATMENTS AT A GLANCE
Know what each one does and when to reach for it
| Treatment | Trace It | Best For | Board Clue |
|---|---|---|---|
| Cryotherapy (liquid N2) | Freezes and destroys dysplastic cells | 1-3 discrete, clearly visible lesions | Most common first-line for isolated AK |
| 5-Fluorouracil (5-FU) cream | Antimetabolite; kills rapidly dividing dysplastic cells | Field treatment, multiple lesions over broad area | Causes inflammation/crusting as it works (that's a good sign) |
| Imiquimod cream | TLR-7 agonist; activates local immune response to destroy dysplastic cells | Field treatment, immunocompetent patients | Works via immune system; takes weeks; less useful in immunosuppressed |
| Photodynamic therapy (PDT) | Topical photosensitizer (ALA) + light activation destroys abnormal cells | Recurrent, extensive, cosmetically sensitive areas (face) | Good cosmetic outcome; second-line for refractory cases |
| Diclofenac gel | NSAID; anti-inflammatory + mild anti-proliferative | Mild, limited AK in patients who can't tolerate other treatments | Slowest-acting; least aggressive; for mild cases |
| Surgical excision | Physical removal with margins | Lesion suspicious for SCC; biopsy-confirmed malignancy | If AK is changing, biopsy first, then excise if SCC confirmed |
🧠 Memory Hook for Treatments
Cryotherapy = Choose this for isolated spots
F-U cream = Field treatment
Imiquimod = Immune-boosting field therapy
PDT = Premium option for face & recurrent
Diclofenac = Downscaled, for mild cases
Original clinical vignettes. Shuffled, never-repeat, full explanations for every choice.