SLE, RA, Scleroderma, Dermatomyositis, Sjogren's. They all have joint pain. They all have fatigue. They all have autoantibodies. Here's how to never mix them up again.
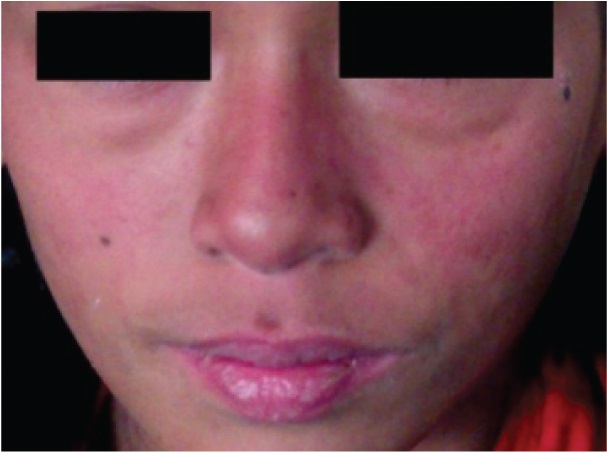
A 32-year-old woman presents with fatigue, joint pain, and a facial rash that spares the nasolabial folds. Labs show ANA positive and low complement levels (C3, C4). She also reports pain in her fingers when exposed to cold.
RA has symmetric joint involvement but no malar rash and doesn't consume complement. Scleroderma has skin tightening, not butterfly rash. Dermatomyositis has a heliotrope rash (on eyelids, not cheeks). Sjogren's has dry eyes and dry mouth as the hallmark.
The low complements are the real clincher · SLE consumes complement via immune complex deposition. None of the others do this.
Know Your Enemies
Each disease has a unique fingerprint. Tap through them. Notice what makes each one DIFFERENT.
SLE
RA
Scleroderma
Dermatomyositis
Sjogren's
Systemic Lupus Erythematosus
The Great Imitator
📷 Malar (butterfly) rash · tap to expand
Who Gets It
Young women (15-45), 9:1 F:M. More severe in Black and Hispanic patients.
EROSIVE arthritis (see bony erosions on X-ray). SLE is non-erosive. This is the #1 differentiator.
Board Trap
Swan neck + boutonniere + ulnar deviation = RA. If they describe a deforming arthritis with bony erosions on imaging, it's RA, not SLE. Also: Caplan syndrome = RA + coal worker's pneumoconiosis.
Scleroderma (Systemic Sclerosis)
The Skin Tightener
📷 CREST: telangiectasias and sclerodactyly · tap to expand
Who Gets It
Women 30-50, 4:1 F:M. Two subtypes matter: limited (CREST) vs diffuse.
Signature Finding
Skin thickening/tightening. Mask-like facies. Sclerodactyly (tight skin on fingers). Raynaud's is often the FIRST symptom.
Elevated CK (creatine kinase) · most important lab. Aldolase also elevated. Confirms muscle damage.
What It Attacks
Proximal muscles (can't climb stairs, can't brush hair). Skin. Lungs (ILD with anti-Jo-1). NOT distal muscles.
Cancer Link
Adult dermatomyositis = screen for occult malignancy. Ovarian, lung, GI cancers. This is the #1 board association.
Board Trap
Heliotrope rash (eyelids) vs Malar rash (cheeks) · both are facial rashes in autoimmune disease but they are NOT the same. Also: polymyositis = same muscle weakness, NO rash, NO cancer association.
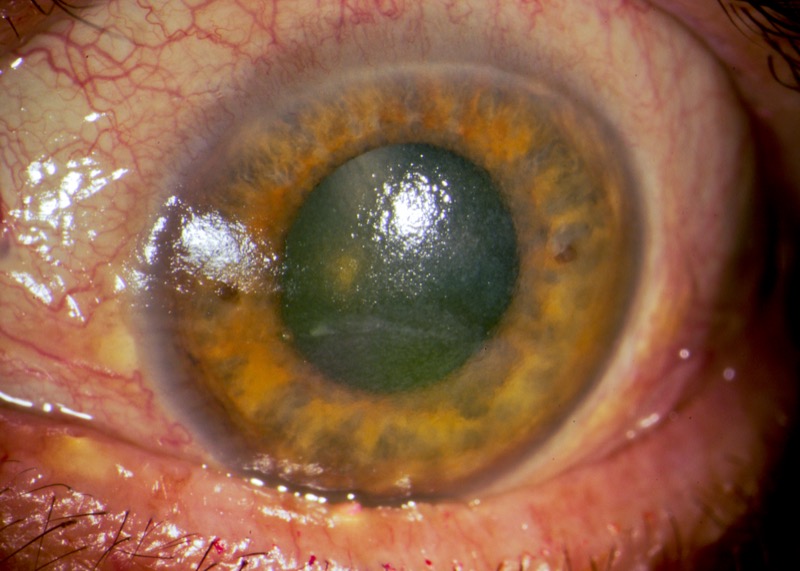
Sjogren's Syndrome
The Dry One
📷 Keratoconjunctivitis sicca · tap to expand
Who Gets It
Women 40-60, 9:1 F:M. Often coexists with RA or SLE (secondary Sjogren's).
Anti-SSA (Ro) and Anti-SSB (La). RF also elevated. Anti-SSA crosses the placenta!
Unique Labs
Positive Schirmer test (reduced tear production). Lip biopsy shows lymphocytic infiltration of minor salivary glands.
What It Attacks
Exocrine glands (lacrimal, salivary). Can also cause renal tubular acidosis (Type 1), peripheral neuropathy, and interstitial nephritis.
Cancer Link
44x increased risk of MALT lymphoma (mucosa-associated lymphoid tissue). Parotid gland swelling that becomes hard/fixed = biopsy immediately.
Board Trap
Anti-SSA (Ro) in a pregnant woman = risk of neonatal lupus and congenital heart block. The antibody crosses the placenta. They WILL test this. Also: dental caries from chronic dry mouth is a classic Sjogren's complication.
Antibody Match
Match each antibody to its disease. Wrong guesses shake. Right ones lock in.
Anti-dsDNA
→
SLE
RA
Scleroderma
Dermatomyositis
Sjogren's
Anti-CCP
→
SLE
RA
Scleroderma
Dermatomyositis
Sjogren's
Anti-Scl-70
→
SLE
RA
Scleroderma
Dermatomyositis
Sjogren's
Anti-Jo-1
→
SLE
RA
Scleroderma
Dermatomyositis
Sjogren's
Anti-SSA (Ro)
→
SLE
RA
Scleroderma
Dermatomyositis
Sjogren's
Anti-centromere
→
SLE
RA
Scleroderma
Dermatomyositis
Sjogren's
Anti-Smith
→
SLE
RA
Scleroderma
Dermatomyositis
Sjogren's
All matched. The antibody fingerprint is the fastest way to a diagnosis in clinical practice. Anti-dsDNA tracks SLE activity, Anti-CCP is the most specific for RA, Anti-Scl-70 means diffuse scleroderma, Anti-centromere means CREST, Anti-Jo-1 is antisynthetase syndrome, and Anti-SSA crosses the placenta.
The Diagnostic Algorithm
A patient has fatigue, joint pain, and a positive ANA. Walk through the decision tree.
1
Does the patient have SKIN findings?
Yes: facial rash (butterfly pattern on cheeks)
Yes: skin tightening / sclerodactyly
Yes: purple eyelid rash / knuckle papules
No significant skin findings
2
The malar rash spares nasolabial folds. Are complements (C3/C4) low?
Yes - low complements
No - normal complements, patient on hydralazine/procainamide/etanercept
2
Skin tightening detected. Is Raynaud's present? Where is the skin involvement?
Raynaud's + skin limited to distal extremities/face + dysphagia
Tap each card to reveal the hook. These are meant to stick.
🦋
SLE
The butterfly rash is the logo. Lupus = wolf, but think butterfly on the face. She eats her own complement (low C3/C4) because she attacks everything, including herself. Double-stranded DNA for double the trouble.
tap to reveal
🔨
RA
RA destroys joints. SLE doesn't. That's the whole thing. Swan necks and hammer toes. If X-ray shows erosions, it's RA. Anti-CCP = Can Confirm Precisely (97% specific).
tap to reveal
🧊
Scleroderma
CREST = the mild version (think: a nice crest on a wave). Anti-centromere for the center of the cell = the milder, more contained form. Scl-70 for the one that goes everywhere (diffuse = worse).
tap to reveal
💪
Dermatomyositis
Heliotrope = eyelids turn purple like the heliotrope flower. Gottron's on the knuckles (imagine punching something and your knuckles go purple). In adults: the muscles are weak AND there might be a tumor hiding. Always screen.
tap to reveal
💧
Sjogren's
SSA and SSB = Sjogren's Syndrome Antibody (and B). Dry eyes, dry mouth, dry everything. The A antibody is the dangerous one in pregnancy · it crosses the placenta and blocks the baby's heart. MALT lymphoma = the glands went bad.
tap to reveal
The Lineup
Eight joint diseases. Tap to flip each one.
🦵
Rheumatoid Arthritis
Symmetric small joints, morning stiffness
Pattern: symmetric polyarthritis, small joints (MCP, PIP)
Stiffness: morning stiffness >1 hr
Labs: RF, anti-CCP (most specific)
Path: pannus formation erodes cartilage
Extra-articular: nodules, ILD, vasculitis
Treat: MTX first-line, then biologics (anti-TNF)
🦡
SLE
Butterfly rash, multi-organ, low complement
Rash: malar butterfly, spares nasolabial folds
Mnemonic: SOAP BRAIN MD
Specific Ab: anti-dsDNA, anti-Smith
Labs: low C3/C4, false+ VDRL
Renal: class III/IV lupus nephritis = severe
Treat: hydroxychloroquine for all patients
🧑
Ankylosing Spondylitis
Young male, bamboo spine, HLA-B27
Who: young male, sacroiliac joint pain
Imaging: bamboo spine (X-ray)
Genetics: HLA-B27
Extra-articular: uveitis, aortic regurgitation
Treat: NSAIDs first-line, then anti-TNF
🧬
Psoriatic Arthritis
Asymmetric, DIP joints, sausage digits
Pattern: asymmetric, DIP joints specifically
Hallmark: sausage digit dactylitis
Skin: nail pitting, psoriatic plaques
Pearl: skin plaques can precede or follow joint disease
Ankylosing spondylitis: NSAIDs first, then anti-TNF.
Aspirate the joint. Any crystals?
Gout: monosodium urate. Colchicine or NSAIDs for flare. Allopurinol for prevention.
Pseudogout: CPP crystals. Elderly patient, wrists or knees. Chondrocalcinosis on X-ray.
Fibromyalgia or OA: widespread tender points with no lab findings = fibromyalgia. Treat with duloxetine, pregabalin, aerobic exercise.
Test Yourself
clinical vignettes. No time pressure. Take your time.
clinical Walkthrough
clinical Walkthrough
Original clinical vignettes. Shuffled, never-repeat, full explanations for every choice.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 1, 2026 at 10:03 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.