Benign lumps, scary mimics, and the red flags that separate them. From fibroadenoma to inflammatory carcinoma.🔑Two pivots on every stem: Is it MOBILE or FIXED? Does she have DISCHARGE? Those two cut the differential in half.
A 42-year-old premenopausal woman presents with spontaneous unilateral bloody discharge from the left nipple. She has no palpable mass. Mammogram shows a single dilated duct without calcifications. Which of the following is the most likely diagnosis?
Invasive ductal carcinoma
Intraductal papilloma
Fibrocystic changes
Phyllodes tumor
Think of it like a tiny polyp growing inside a milk duct. Intraductal papilloma is the #1 cause of bloody/serosanguinous nipple discharge in premenopausal women. It sits inside a single duct, too small to feel, but it bleeds because its stalk has fragile blood vessels. IDC can also cause bloody discharge, but you would expect a hard mass or microcalcifications. Fibrocystic changes give you bilateral cyclic pain, not unilateral discharge. Phyllodes tumors are big, round, and do not discharge. Bloody nipple discharge + single dilated duct + no mass = intraductal papilloma until proven otherwise.
Clinical Images
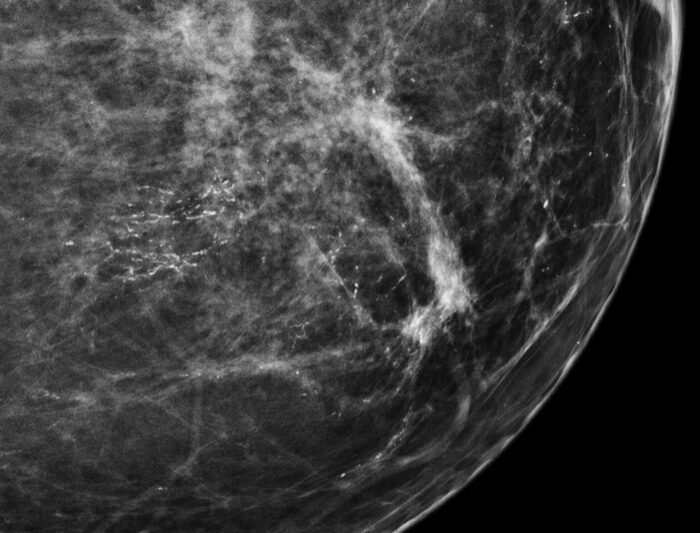
📷 Mammogram: clustered microcalcifications in DCIS · tap to expand
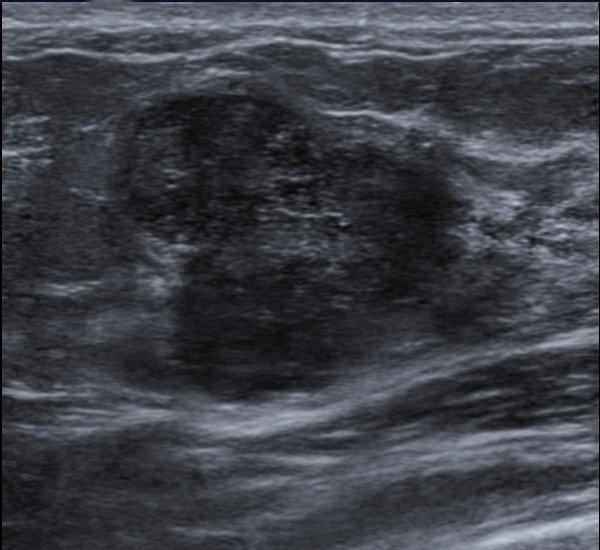
📷 US: well-circumscribed, mobile breast mass (fibroadenoma) · tap to expand
📷 Peau d'orange: inflammatory breast cancer skin change · tap to expand
The Lineup
Tap a card to reveal the full profile. Lock in the key clue first🔑Every card front has ONE diagnostic hook. That is the board question clue. Commit before you flip., details second.
🪨
Invasive Ductal Carcinoma
Most common (~75%). Irregular hard mass. Spiculated on mammogram.🔑IDC = "It's Definitely Cancer." Rock-hard + fixed + spiculated = IDC until proven otherwise.
tap to flip
Invasive Ductal Carcinoma (IDC)
Freq~70-80% of all breast cancers; most common type
MammoSpiculated mass + clustered microcalcifications
SkinDimpling (tethered to Cooper ligaments)
ReceptorsTest ER, PR, HER2 on every biopsy specimen
ManageLumpectomy + radiation or mastectomy; SNB; systemic therapy per receptor
📊
DCIS
Microcalcifications only. No palpable mass. Non-invasive.🔑DCIS = "Danger Contained In Situ." Basement membrane still intact. The wall has not broken yet.
MammoClustered microcalcifications ONLY; no palpable mass
SubtypeComedocarcinoma = central necrosis; worst DCIS prognosis
RiskCan progress to IDC if untreated (pre-invasive)
ManageLumpectomy + radiation; tamoxifen if ER+
🧻
Invasive Lobular Carcinoma
Indian file pattern. Bilateral. No calcifications🔑ILC is the stealth cancer. Cells sneak single-file through stroma. Mammogram misses it because no calcifications. MRI is the better tool.. Easy to miss.
tap to flip
Invasive Lobular Carcinoma (ILC)
Freq2nd most common (~10-15%)
PathSingle-file "Indian file" pattern; loss of E-cadherin
CalcificationsNONE (reason mammography misses it)
BilateralHigher bilateral risk than IDC
ReceptUsually ER+/PR+; rarely HER2+
ManageSame as IDC; MRI preferred over mammo for surveillance
🔥
Inflammatory Breast Cancer
Peau d'orange. Lymphatic invasion. Worst prognosis.🔑Not a mass. Looks like mastitis. Non-lactating + antibiotics fail = biopsy immediately. Every time. NOT a mass!
tap to flip
Inflammatory Breast Cancer
KeyPeau d'orange (orange-peel skin), warmth, erythema; NO discrete mass
ManageNeoadjuvant chemo FIRST, then mastectomy + radiation (never surgery first)
🏳
Fibroadenoma
Young women. Mobile, smooth, rubbery.🔑"Breast mouse" = it runs away from your fingers. If you can chase it around, it's a fibroadenoma. No malignant potential.
HormonesEstrogen-responsive: grows in pregnancy, shrinks in menopause
Cancer riskNo malignant potential (unless complex variant)
ManageObserve if <3 cm and typical; excise if growing or atypical
🌿
Phyllodes Tumor
Large stromal + epithelial. Rapidly growing.🔑Phyllodes = fibroadenoma that went to the gym too much. Same fibroepithelial mix, but rapid growth + cystic areas on US = clue. Low-grade malignant potential.
tap to flip
Phyllodes Tumor
Age5th decade (40s-50s)
MassLarge, rapidly growing, well-defined; leaf-like stroma on histology
USWell-circumscribed, hypoechoic with cystic regions
Malignant10-25% malignant potential (most are benign)
ManageWide local excision with margins; no axillary dissection needed
🤝
Intraductal Papilloma
Bloody nipple discharge. Single duct. No mass.🔑Like a nosebleed from a nasal polyp. One duct, one fragile stalk, one bleed. Unilateral bloody discharge + clean mammogram = papilloma.
tap to flip
Intraductal Papilloma
AgePremenopausal (30s-50s)
Key ClueUnilateral serosanguinous/bloody nipple discharge; no mass
ImagingSingle dilated duct; usually invisible on mammogram
PalpableUsually NOT palpable
RiskSlight cancer risk; core needle biopsy needed
ManageDuct excision (microdochectomy)
📷
LCIS
Incidental finding. Bilateral risk marker.🔑LCIS is the weather advisory: conditions are risky. Not the storm itself. Bilateral risk, not a direct precursor. Invisible on imaging.
tap to flip
Lobular Carcinoma In Situ
KeyIncidental on biopsy; no mass, no calcifications on imaging
TypeRisk marker, NOT direct precursor; bilateral cancer risk
GeneticsLoss of E-cadherin (lobular lesions lose E-cadherin; ductal retain it)
RiskIncreases risk in EITHER breast bilaterally
ManageSurveillance + tamoxifen chemoprevention; no surgery
🔴
Paget Disease of Breast
Eczematous nipple. Steroids fail.🔑Termites disguised as wood grain. Looks like eczema on the surface. Cancer underneath. Unilateral + steroid failure = biopsy, not more cream. Underlying DCIS or IDC.
tap to flip
Paget Disease of Breast
KeyUnilateral eczema/crusting/erosion of nipple that does not respond to steroids
PathLarge Paget cells (clear halos) in nipple epidermis; PAS+
UnderlyingAlmost always associated with underlying DCIS or IDC
ManageFull workup for underlying malignancy; mastectomy or lumpectomy
🚕
Fat Necrosis
Post-trauma. Painless mass. Oil cyst with rim calcification.🔑Like a bruised avocado: damaged fat walls off into an oil cyst. Seatbelt injury + breast mass = fat necrosis first, cancer second.
tap to flip
Fat Necrosis
AgeAny age; history of trauma (MVC, fall, surgery)
KeyPainless mass after breast trauma; CAN mimic cancer on exam
ImagingOil cyst (fat-density center); RIM calcification (not clustered)
Walk the breast mass algorithm.🔑Two pivots: AGE determines first imaging (US vs mammogram). BI-RADS score determines biopsy vs follow-up. Learn those two forks and the tree writes itself. Make a call at each fork before the next step reveals.
Side-by-Side
Quick-reference comparison.🔑The three columns that matter most in clinical practice: Age, Discharge type, Imaging pattern. Those three cut it to one diagnosis. Scroll horizontally on mobile.
Lesion
Age
Presentation
Discharge
Imaging
Management
Fibroadenoma
15-35
Rubbery, mobile, painless
None
Solid, well-defined on US
Observe or excise
Fibrocystic
25-50
Bilateral, cyclic pain
Clear/straw
Multiple cysts
Reassurance, OCP
Papilloma
30-50
No mass, single duct
Bloody
Dilated duct on ductogram
Duct excision
Phyllodes
40-50
Large, rapidly growing
None
Hypoechoic, cystic on US
Wide excision
Fat Necrosis
Any
Post-trauma mass
None
Oil cyst, rim calcification
Observation
DCIS
50-60
No mass (screening only)
Rare
Microcalcifications
Lumpectomy + XRT
LCIS
40-50
Incidental on biopsy
None
Nothing (invisible)
Surveillance + tamoxifen
IDC
55-65
Rock-hard, fixed mass
Possible bloody
Spiculated + microcalcifications
Surgery + systemic
ILC
55-65
Subtle thickening, no mass
None
No calcifications; MRI preferred
Surgery + systemic
Paget
50+
Eczematous nipple
Possible
Variable (underlying tumor)
Mastectomy/lumpectomy
Inflammatory
Any
Peau d'orange, no mass
None
Skin thickening, diffuse
Neoadjuvant chemo first
Elimination Round
Read the scenario. Eliminate wrong diagnoses one by one.🔑The elimination game builds the same reasoning the clinical medicine test: process of elimination, one clue at a time. Last one standing wins.
The Villains
Seven breast neoplasms. Each card front: the entity name and the single clue that makes it a board target. Flip for histology, clinical features, and the pearl that closes the question.
Pearl: biopsy the nipple, not the rash periphery. PAS-positive Paget cells confirm
Test Yourself
5 randomized questions from a bank of 10.🔑Read the last sentence of every stem first. That is where the question lives. Then hunt the stem for the one clue that answers it. All original.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 1, 2026 at 10:03 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.