Clue cells or trichomonads? Gray or green? They all blur together until you know the trick.
Section 1
The Lineup
Tap a card to flip it and read the backstory. Know your villains.
NOT an STI
🦠
Bacterial Vaginosis
Gardnerella vaginalis
WeaponThin, gray, fishy discharge
pH
Whiff TestPositive 💨
TreatmentMetronidazole
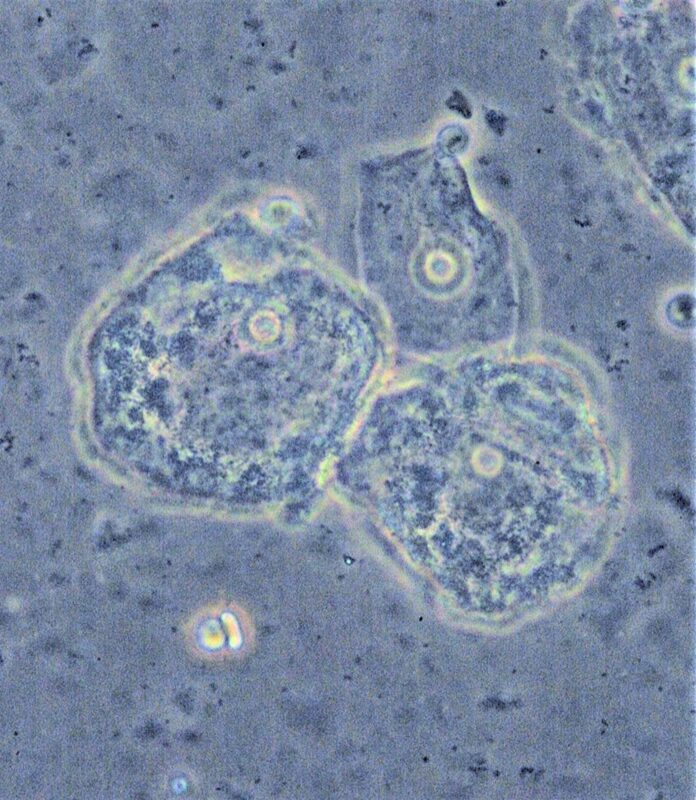
🔎 CLUE CELLS
tap to flip →
Why BV Happens
The Bouncer Analogy
Lactobacillus is the bouncer of the vagina. It makes lactic acid, keeping pH low (~4.0) and bad bacteria out.🔑The bouncer keeps it tight under 4.5. When he leaves, anything gets in.
What Goes Wrong
BV = bouncer left. Gardnerella and anaerobesBacteria that thrive without oxygen. They produce amines (fishy smell) as metabolic byproducts. move in. pH rises above 4.5.
Why Clue Cells?
Gardnerella coats vaginal epithelial cells. Edges look stippled/blurred because they're covered in bacteria. That's the clue.🔑Gardnerella → Gray. Clue cells = coated cells giving a clue.
NOT an STI
BV is a flora shift. No partner treatment needed. Risk factors: douching, antibiotics, new partners.
tap to flip back →
STI ⚠
🦠
Trichomoniasis
Trichomonas vaginalis
WeaponGreen-yellow, frothy
pH
Classic SignStrawberry cervix 🍓
TreatmentMetro + TREAT PARTNER
🔎 MOTILE TRICHOMONADS
tap to flip →
Why Trich Is Different
Not Bacteria
Flagellated protozoan with a tail. Actual parasite, not a flora shift. That's why it's an STI.
Microscopy
Wet mount shows pear-shaped organisms darting around with visible flagella. They MOVE. Clue cells don't move.
Strawberry Cervix
Intense inflammationImmune response creates punctate hemorrhages on the cervix, giving it a strawberry appearance. → punctate hemorrhages. Classic colposcopy finding.
Why TREAT THE PARTNER?
It's sexually transmitted. Men are asymptomatic carriers. Treat only one = immediate reinfection.🔑If you don't treat the partner, he just keeps coming... back.
tap to flip back →
NOT an STI
🍄
Candidiasis
Candida albicans
WeaponThick, white, cottage cheese
pH
Key SymptomINTENSE ITCHING 🔥
TreatmentFluconazole
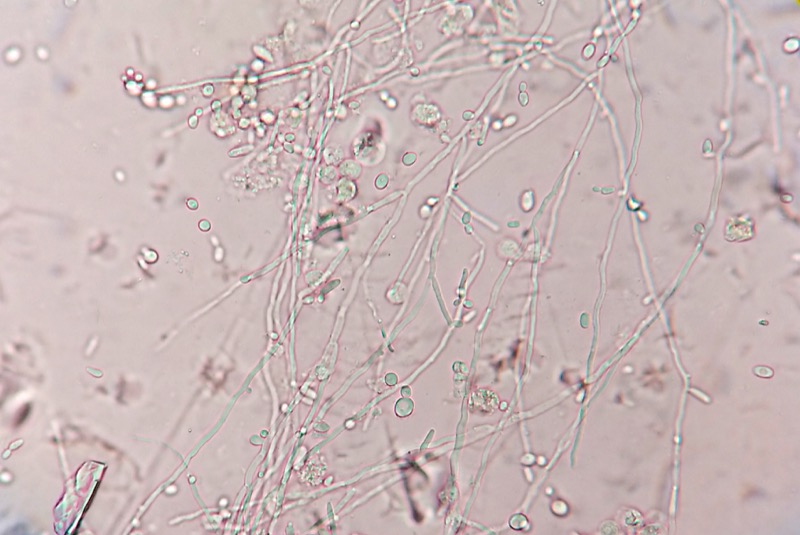
🔎 PSEUDOHYPHAE on KOH
tap to flip →
Why Candida Is the Odd One Out
THE Key Differentiator
pH is NORMAL (<4.5). Single biggest board distinguisher. Normal pH = Candida. Elevated pH = BV or Trich.🔑Under 4.5 = undisturbed flora = only yeast can survive here.
Why KOH Prep?
KOH lysesDissolves human cells and bacteria, leaving only tough fungal cell walls visible on the slide. everything except fungi. Pseudohyphae (branching filaments) stand out clearly.
Why Fluconazole, Not Metro?
Metro kills anaerobes. Candida is a fungus. Need an azole that blocks ergosterolThe lipid in fungal cell membranes. Block it and the membrane falls apart. synthesis.
tap to flip back →
STI ⚠
😵
Pelvic Inflammatory Disease
N. gonorrhoeae + C. trachomatis
TriggerAscending infection from cervix
Classic SignChandelier sign 🕑
ComplicationFitz-Hugh-Curtis perihepatitis
TreatmentCefoxitin + Doxycycline
🔎 CMT on pelvic exam
tap to flip →
PID: When It Goes Upstream
How It Starts
Gonorrhea or Chlamydia in the cervix ascends through the uterus into the fallopian tubes and ovaries. Causes endometritis, salpingitis, oophoritis.
Chandelier Sign
Moving the cervix during pelvic exam causes excruciating pain. Patient grabs the chandelier.🔑CMT = Cervical Motion Tenderness. She hits the chandelier because you touched the inflamed tubes through the cervix.
Fitz-Hugh-Curtis
Chlamydia or Gonorrhea spreads to the liver capsule → perihepatitisInflammation of the liver capsule (not the liver itself). Causes right upper quadrant pain that mimics cholecystitis. → RUQ pain. Classic board curveball: PID presenting as RUQ pain.
Why Dual Coverage?
PID is polymicrobial. Cefoxitin covers GN + anaerobes. Doxycycline covers Chlamydia (Chlamydia won't grow on standard culture).
HSV = PAINFUL. Syphilis = painless. This is the single most-tested distinction. If the stem says "painful ulcer," go HSV.
Lifecycle
Prodrome (tingling/burning) → grouped vesicles → ulcers → crusting. Primary outbreak worst. Virus hides in dorsal root gangliaNerve cell bodies near the spinal cord. HSV hides here indefinitely, reactivating with stress, illness, or UV exposure. forever.
Tzanck Smear
Scrape the base of the ulcer. See multinucleated giant cells with intranuclear inclusions. Not specific to HSV-2 (also HSV-1, VZV).🔑Tzanck = Herpes family. Many nuclei crammed together = the "group" picture that matches the grouped vesicles.
Neonatal Risk
Primary outbreak near delivery = C-section. Neonatal HSV is devastating: encephalitis, disseminated disease.
tap to flip back →
STI ⚠
💀
Syphilis
Treponema pallidum
PrimaryPainless chancre (indurated, clean)
SecondaryDiffuse rash, palms + soles
TreatmentPenicillin G
DiagnosisRPR/VDRL screen, then FTA-ABS confirm
🔎 PAINLESS ulcer + palms/soles rash
tap to flip →
Syphilis: The Great Imitator
Primary vs Secondary
Primary = painless chancre at site of inoculation (heals spontaneously). Secondary = weeks later: diffuse maculopapular rash including palms and soles.🔑Only two things cause palms/soles rash: Syphilis and Rocky Mountain Spotted Fever. Both need treatment.
Why Painless?
Treponema creates a localized immune response that seals the ulcer with firm fibrous tissue. No open nerve endings exposed = no pain. Then immune system "wins" locally but T. pallidum disseminates.
Testing Logic
RPR/VDRL = non-treponemalDetects antibodies against cardiolipin released by damaged cells. False positives: lupus, pregnancy, viral infections. Titers track treatment response. screen (cheap, fast, false-positives exist). Confirm with FTA-ABS (treponemal-specific, stays positive for life).
tap to flip back →
Section 2
Clinical Photos
What they actually look like under the scope and on exam. Tap to expand.
📷 BV: Clue CellsStippled epithelial cells on wet prep. Wikimedia
Caused by N. gonorrhoeae + C. trachomatis (often both)
Can cause Fitz-Hugh-Curtis: RUQ pain (violin-string adhesions on liver capsule)
Treat: Cefoxitin + Doxycycline
Localized vaginitis/cervicitis
Infection hasn't ascended into upper tract
Treat the identified organism (GC, Chlamydia) and re-evaluate
Monitor for ascending signs
BV
Trich
Candida
PID
Organism
Gardnerella
T. vaginalis
C. albicans
GC + Chlamydia
pH
>4.5
>4.5
<4.5
Variable
Microscopy
Clue cells
Motile trichomonads
Pseudohyphae (KOH)
CMT on exam
STI?
No
Yes
No
Yes
Treatment
Metro
Metro + partner
Fluconazole
Cefoxitin + Doxy
Hallmark
Fishy smell
Strawberry cervix
ITCHING
Chandelier sign
Section 4
clinical Quiz
8 questions in the pool. 4 presented per session. Get them all for confetti.
Section 5
Don't Fall For These
⚠️
Trap 1: Same Drug, Different Rules
Both BV and Trich use metronidazole. Only Trich requires partner treatment. "Treated with metro, returns with same symptoms" = untreated partner = Trich.🔑Metro cures it. But if partner wasn't treated, it was Trich. BV doesn't have a partner to infect.
⚠️
Trap 2: Clue Cells vs Trichomonads
Clue cells are epithelial cells coated with bacteria (static). Trichomonads are separate organisms that swim. If it moves = Trich. If it's stuck to a cell = BV.
⚠️
Trap 3: pH Is the Fastest Differentiator
Normal pH (<4.5) = Candida. Period. Eliminates BV and Trich instantly.🔑4.5 is the line. Under = undisturbed. Over = overgrowth (BV or Trich).
Fitz-Hugh-Curtis perihepatitis: Chlamydia or GC spreads to liver capsule → right upper quadrant pain mimicking cholecystitis. Young sexually active female + RUQ pain = rule out PID before gallbladder.🔑Fitz-Hugh-Curtis: violin string adhesions on the liver capsule from ascending infection. Not the liver itself, just the capsule.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 1, 2026 at 10:03 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.
Section 6
Decision Tree: Diagnosing the Vaginal or Pelvic Infection
Work through symptoms, exam findings, and labs. Arrive at the diagnosis.
Before you reveal the branch: is this a pH problem, a moving-organism problem, or an upper-tract pain problem?
Good. Use the first abnormal branch, then confirm with the microscope or pelvic exam.
Chief complaint: vaginal discharge, odor, itching, or pelvic pain?
Check pH. Whiff test (KOH). Wet mount.
Bacterial Vaginosis (BV). Treat: metronidazole (oral or vaginal). No partner treatment needed. STI screen but BV is NOT an STI.
Trichomonas vaginalis. Confirm: motile pear-shaped flagellates on wet prep.
Classic Trich with colpitis macularis. Treat: metronidazole single dose, TREAT PARTNER. STI, notify partners.
Still Trich, just without the classic cervical sign. Same treatment: metro + partner treatment. Cervical sign absent in many cases.
pH < 4.5 (normal or low), NO fishy odor. Add KOH to wet prep.
Candida vulvovaginitis confirmed. First episode or recurrent?
Fluconazole 150mg oral single dose (first-line). Topical azole if oral azole contraindicated (pregnancy). No partner treatment needed for uncomplicated cases.
Recurrent vulvovaginal candidiasis. Obtain culture to confirm species (C. glabrata is fluconazole-resistant). Consider suppressive therapy and screen for diabetes or immunosuppression.
Wet prep and KOH are only 50-70% sensitive. If clinical picture is classic (thick white discharge, low pH, severe pruritus), empiric treatment for candida is reasonable. Alternatively send fungal culture for confirmation.
Check for cervical motion tenderness (CMT), uterine tenderness, adnexal tenderness on bimanual exam.
Pelvic Inflammatory Disease (PID). Caused by GC or Chlamydia ascending from cervix. Check for fever and labs (elevated WBC, ESR, CRP).
PID outpatient: ceftriaxone IM 500mg once PLUS doxycycline 100mg BID x 14 days (add metronidazole if BV co-infection). Treat partner. Follow up in 72 hours.
PID inpatient: cefoxitin IV PLUS doxycycline (or clindamycin + gentamicin if penicillin-allergic). Transition to oral when improving. TOA may need IR drainage or surgery if no improvement in 72 hours.
Fitz-Hugh-Curtis syndrome: PID spreading to liver capsule (perihepatitis). Violin-string adhesions on liver capsule. Treat for PID, same regimen. Rule out cholecystitis (USS), but if young sexually active female: think PID first.