Two 46XY patients raised as girls. Same chromosomes, different broken switch. One grows breasts. One grows a beard.
Reproductive · Sexual Differentiation
AIS vs 5-ARD
Two 46XY teens, both raised as girls. One walks into puberty and grows breasts. The other grows a beard. Same chromosomes. Different broken switch.
The Setup
Same blueprint, two outcomes
Before we walk the timeline, take the bait. Get this wrong on purpose so the rest of the page nails it down.
Alex, 16, was raised as a girl. Pediatrician noted "ambiguous genitalia" at birth, parents picked female. Now Alex is in your clinic because puberty started six months ago and Alex's voice is dropping, jaw is squaring, body hair is spreading. No breasts. Karyotype: 46XY. Testes are palpable in the inguinal canals. There is no uterus on ultrasound.
What is the most likely diagnosis?
The Signature Move
Drag puberty across two Alexs
Same karyotype. Same testes. Same testosterone in the blood. Drag the slider and watch what happens at puberty · the divergence is the whole point.
Alex A
AIS · receptors broken
Karyotype46XY
TestesYes (inguinal)
AMHYes
Uterus / tubesNone
External genitaliaFemale
BreastsNo (yet)
Body hairSparse / absent
Alex B
5-ARD · can't make DHT
Karyotype46XY
TestesYes (inguinal)
AMHYes
Uterus / tubesNone
External genitaliaAmbiguous
BreastsNo
Body hairSparse / absent
In Utero · Week 8
Both Alexs have testes. Both are pumping AMH (which deletes the female internal plumbing) and testosterone. So far they look identical.
In utero
Birth
Childhood
Puberty
Notice: right now the two Alexs look identical. Drag the slider to puberty and watch them split.
⚠
The one-sentence rule that owns this whole topic
AIS = breasts at puberty (testosterone is unused, so it gets aromatized to estrogen and the body grows breasts). 5-ARD = beard at puberty (testosterone is used directly, no aromatization needed). Same Y chromosome, opposite outcomes, decided by whether the receptor works.
Core Profiles
Match each disorder to the broken step
Six high-yield disorders. Each profile keeps the karyotype, puberty pattern, lab signature, and board rule visible at once.
⚌
Turner Syndrome
45,X
Core cue
Turner 45,X
GonadalStreak ovaries
PubertyPrimary amenorrhea, no spontaneous puberty
PhenotypeShort, webbed neck, shield chest
LabsHigh FSH/LH, low estrogen
Key ruleNo Y = no testes = streak ovaries
♾
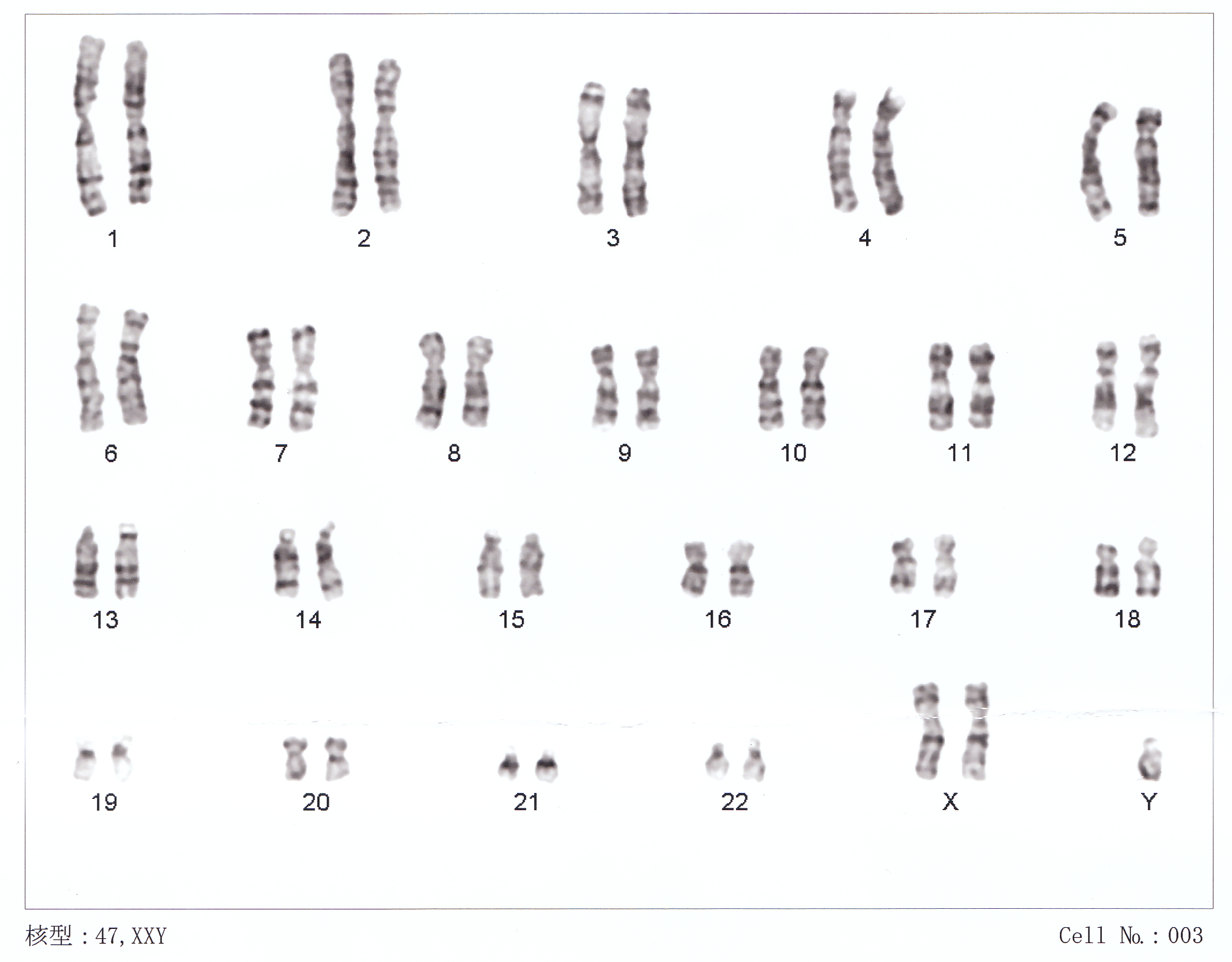
Klinefelter
47,XXY
Core cue
Klinefelter 47,XXY
TestesSmall and firm
PubertyGynecomastia, tall, infertile
LabsHigh FSH/LH, low testosterone
PhenotypeAzoospermia, eunuchoid habitus
Key ruleExtra X = seminiferous failure
🔒
AIS
46,XY · dead receptor
Core cue
AIS 46,XY
BreakAndrogen receptor non-functional
PubertyBreasts (estrogen), no beard, no period
GenitaliaFemale at birth, no uterus
HairScant pubic/axillary
Key ruleBreasts at puberty = AIS
🔤
5-ARD
46,XY · no DHT
Core cue
5-ARD 46,XY
Break5-alpha reductase enzyme missing
BirthAmbiguous external genitalia
PubertyBeard, voice drops, masculinizes
LabsLow DHT, normal testosterone
Key ruleBeard at puberty = 5-ARD
⚡
CAH (21-OH)
46,XX · adrenal
Core cue
CAH 46,XX
Break21-hydroxylase deficiency
EffectAdrenal androgens virilize a 46XX female
BirthAmbiguous genitalia in 46XX baby
LabsHyponatremia, hyperkalemia (salt-wasting)
Key ruleIf 46XX + ambiguous = CAH first
🔴
Mullerian Agenesis
46,XX · no uterus
Core cue
MRKH 46,XX
Karyotype46,XX (female)
BreakMullerian ducts fail to develop
HormonesNormal FSH, LH, estradiol
PubertyNormal breast development, no period
HairNormal pubic and axillary hair
Key rule46,XX + absent uterus + normal hormones = MRKH
Clinical Photos
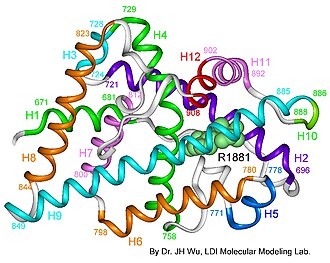
Androgen receptor: the broken lock in AIS
Individuals of Latin American descent with Turner syndrome
Human chromosomes XXY: Klinefelter karyotype
Steroidogenesis: where each disorder breaks
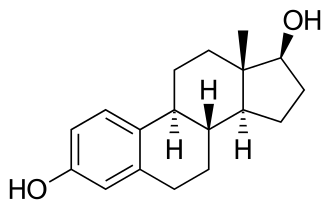
Estradiol: the aromatization endpoint in AIS
The Algorithm
Karyotype to phenotype in 3 questions
Every sex differentiation board case starts the same way. Follow these three questions and you will never mislabel a patient again.
Question 1: What is the karyotype?
This splits every case into two parallel roads. Everything downstream depends on whether there is a Y chromosome.
46,XX or 45,XNo Y: no testes will form. Go to ovarian pathway. Turner (45,X) or CAH (46,XX virilized by adrenal androgens).
46,XY or 47,XXYY present: testes will form. Go to androgen pathway. AIS, 5-ARD, or Klinefelter.
Question 2 (Y present): Did the testes make androgens AND can the body read them?
Testes always make AMH (so no uterus) and testosterone. The question is what happened next to that testosterone.
Receptor dead (AIS)Testosterone cannot bind anything. Aromatizes to estrogen. Breasts at puberty, female external genitalia at birth, no uterus.
Enzyme missing (5-ARD)Testosterone cannot become DHT in utero. Ambiguous external genitalia at birth. At puberty, testosterone itself virilizes: beard, deep voice.
Question 3: What happened at puberty?
Breasts in a 46,XY = AIS. Beard in a 46,XY raised female = 5-ARD. Gynecomastia in a 46,XY male = Klinefelter. This is the disambiguation endpoint. Every board question resolves here.
🔐
Three memory hooks for three disorders
AIS = ICE. Receptor is frozenInsensitive, Converts to estrogen, Estrogen builds breasts. Dead receptor = testosterone unused = aromatizes = breast tissue. The lock is broken, so the key (testosterone) never opens anything, and gets melted down into estrogen. so testosterone aromatizes to estrogen. Breasts at puberty.
5-ARD = "Late beard." The enzyme
can't finish5-alpha reductase converts testosterone to DHT. In utero, no DHT = ambiguous genitalia. But the receptor still works. At puberty, the LH surge produces SO much testosterone that even without DHT conversion, the receptor gets overwhelmed and virilizes. The beard arrives late but it arrives.
making DHT in utero, so genitalia are ambiguous at birth. Beard comes in at puberty when testosterone floods the functional receptor.
Klinefelter = "Extra X, less T."Extra XEach extra X chromosome damages the seminiferous tubules (the testosterone-making part of the testis). More X chromosomes = more testicular failure = less testosterone and less sperm. FSH and LH spike trying to compensate, but the testis can't respond.
disrupts seminiferous tubules, drops testosterone, spikes FSH/LH. Gynecomastia, azoospermia, tall stature.
Lock It In
Drop each feature on the right Alex
Tap a card, then tap the column it belongs to. Wrong drops bounce back. The point is the disambiguation rule, not the speed.
Which Alex does each clue belong to? Both have 46XY and testes. Sort by the puberty outcome.
Alex A · AIS
Alex B · 5-ARD
🧠
Memory hook to never miss this
AIS = ICE. Receptors are frozen, so testosterone slides past unused and gets converted to Estrogen. Insensitive, Converts, Estrogen-dominant → eyes go to the breasts. 5-ARD = "Five for the beard." Five-alpha can't finish DHT in utero (ambiguous at birth), but at puberty pure testosterone is enough · five years late, but the beard arrives.
🔐If the patient is a 46XY teen and has BREASTS → AIS. If they have a BEARD → 5-ARD. That one swap is 90% of clinical questions.
Feature
AIS
5-ARD
Broken switch
Androgen receptor
5-alpha reductase enzyme
Testosterone in blood
Normal / high
Normal / high
Estrogen in blood
High (aromatized)
Normal
External genitals at birth
Female
Ambiguous
At puberty
Breasts, no beard
Beard, no breasts
Internal female plumbing
None (AMH worked)
None (AMH worked)
New Mechanic
Trace the Switch
Pick a karyotype. Toggle each molecular signal on or off. Watch the internal organs and external genitalia resolve in real time.
Step 1 · Choose karyotype
Step 2 · Toggle signals
Internal anatomy
Wolffian ducts: no signal
Mullerian ducts: default persist
External genitalia & puberty
At birth: female (default)
Puberty: no androgens
Select a karyotype to begin.
You have set: 46,XY + SRY on + AMH on + Testosterone on + 5α-reductase OFF + AR on. Before you toggle, predict: what does this patient look like at birth?
Which phenotype does the configuration above produce?
The Board Trap
Blind vaginal pouch: three answers, one algorithm
The board gives you a teenage girl with primary amenorrhea and a blind-ending vaginal pouch. Three diagnoses share that surface feature. One question separates all three.
Feature
AIS (46,XY)
MRKH (46,XX)
5-ARD (46,XY)
Karyotype
46,XY
46,XX
46,XY
Pubic / axillary hair
Scant or absent
Normal
Absent before puberty
Breast development
Present (small nipples)
Normal
None
Uterus
Absent (AMH worked)
Absent (Mullerian failed)
Absent (AMH worked)
Testosterone
High (male range)
Normal female range
High, DHT low
Puberty outcome
Breasts, no period
Normal breasts, no period
Virilizes (beard, voice)
One-line rule
Scant hair + 46,XY
Normal hair + 46,XX
Virilizes at puberty
🔐
Three hooks for three blind pouches
AIS: Blind pouch + scant pubic hairThe board key for AIS. DHT normally drives pubic and axillary hair growth. Dead androgen receptor means no DHT signal lands anywhere. Normal breasts (estrogen from aromatized testosterone) but almost no body hair. That contrast is the tell. + 46,XY + male-range testosterone = dead receptor. Testosterone aromatizes to estrogen → small breasts but NO full breast development (DHT is also present, suppressing full development). The separator: scant or absent pubic/axillary hair in a teenager with a blind pouch.MRKH: Blind pouch + normal everythingMullerian agenesis (MRKH) looks like a missing building in an otherwise perfect neighborhood. The ovaries work perfectly, estrogen flows, puberty goes normally, normal breasts, normal hair growth, normal hormones. The only missing piece is the uterus. So the patient comes in with no period but totally normal development in every other way. + 46,XX + normal FSH/LH/estradiol = Mullerian ducts just never formed. The factory works perfectly, the packaging machine is missing.
5-ARD: Blind pouch + virilizes at pubertyThe "phallus at 12" presentation. The patient is raised female, ambiguous genitalia at birth, then at age 12-13 the testosterone surge at puberty overcomes the enzyme deficiency and the receptor (which works fine) finally gets enough signal. Jaw sharpens, voice drops, body hair spreads. No breast tissue because testosterone is being actively used, not aromatized. + low DHT + normal testosterone = 5-alpha reductase missing. No breast tissue because testosterone is USED, not converted.
Apply the Algorithm
Identify the diagnosis from clues
Tap each clue in order. Watch the field narrow to one answer. This is the exact logic path the board question expects you to run.
Start here: a teenage girl has primary amenorrhea and a blind-ending vaginal pouch. No uterus on ultrasound. What is the karyotype?
46,XXNo Y chromosome. No testes. No AMH from fetal testes. The uterus failed to form from a different reason: the Mullerian ducts never developed. Ovaries are present and working. Diagnosis: MRKH (Mullerian agenesis). Confirm: normal FSH, LH, estradiol.
46,XYY chromosome present. Testes formed. AMH was secreted and demolished the Mullerian ducts. That is why there is no uterus. Now the question is: why did the external genitalia not masculinize normally? Go to the next branch.
The patient is 46,XY with no uterus and a blind pouch. Check pubic and axillary hair. What does the exam show?
Scant or absent pubic / axillary hairDHT (dihydrotestosterone, the active form of testosterone responsible for body hair growth) requires a working androgen receptor to signal hair follicles. Dead receptor means no DHT signal reaches the follicle. Normal breasts are present because testosterone aromatizes to estrogen. Diagnosis: AIS. Testosterone will be in the male range or above.
Present pubic hair (before puberty) OR no puberty yet; check DHTIf the androgen receptor works, pubic hair grows normally when testosterone/DHT are present. The question is whether DHT was ever made. If testosterone is normal but DHT is low: the 5-alpha reductase enzyme is missing. External genitalia were ambiguous at birth (no DHT in utero), but the receptor is intact. At puberty: virilization. Diagnosis: 5-ARD.
Board rule: the fastest three-way separator
Blind pouch + normal pubic hair + 46,XX + normal hormones = MRKH.
Blind pouch + scant pubic hair + 46,XY + male-range testosterone = AIS. Receptor dead.
Blind pouch + 46,XY + virilizes at puberty + low DHT with normal testosterone = 5-ARD. Enzyme missing.
From the board: "Whenever you see blind vaginal pouch and a teenager, AIS vs 5-ARD are your top two. Add pubic hair to separate them."
Board Walkthrough
15 original vignettes
One at a time. Shuffled every round. Clue highlights glow after you answer. Never see the same case twice until you exhaust the bank.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 13, 2026 at 12:48 AM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.