One rule unlocks a whole category of board questions: a muscle that is stuck contracted holds the joint in the direction it acts, so it restricts the opposite motion. Learn it on the psoas, then watch it transfer.
Extension. The psoas is the major hip flexor. A hypertonic psoas is stuck pulling the hip into flexion, so it physically holds the joint flexed. The motion it cannot allow is its own antagonist: hip extension.
Flexion is wrong because that is the direction the tight muscle is already pulling, so it stays free or even feels strong. Abduction and internal rotation are governed by other muscles, not the psoas. The lost motion is always the opposite of what the tight muscle does.
Pick a muscle. Watch which way it drags the hip, and watch the motion it steals. The green arrow is the pull. The red arc is the motion you lose.
Stop memorizing lists of restricted motions. There is one move. A tight muscle is a rope pulled taut on one side of the joint. The joint sits where the rope drags it, and it cannot travel the way the rope refuses to lengthen. Flexor stuck on means flexion is the resting deformity and extension is the casualty. Name the muscle, name its action, flip it. That distinction drives every one of these questions.
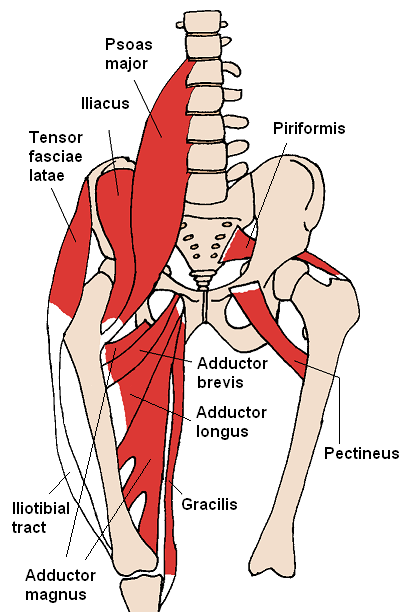
If you know where the psoas starts, where it ends, and what it does, the restricted motion is not a fact to memorize. It is the only answer that fits.
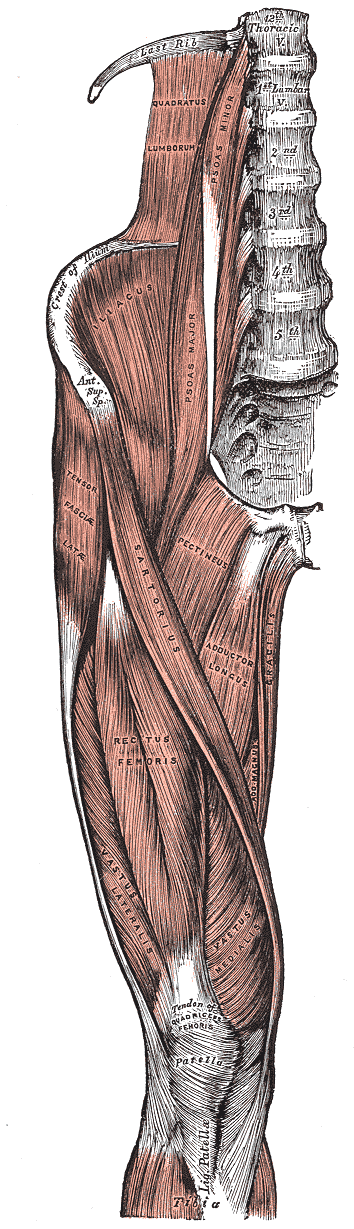

Look at where it inserts. The lesser trochanter sits in front of the hip axis. Anything that crosses in front of a joint and pulls is a flexor. You do not need a chart. Front of the axis means flexor, flexor stuck means extension is gone. Find the insertion, find the answer.
The whole syndrome is the rule playing out in a person. The psoas will not lengthen, so the body folds forward to live inside the deficit.

When the patient flattens the back by pulling one knee up, gravity should let the other leg lie flat. A shortened psoas will not allow its hip to extend onto the table, so that thigh floats. The test is just the opposite-motion rule, measured. The muscle that flexes refuses to extend.
The psoas does not only get stuck. It can get irritated from the outside by an inflamed organ lying against it. The exam looks similar. The disposition could not be more different.
A retrocecal appendix sits directly on the right psoas. When it inflames, every stretch of that muscle hurts. The classic bedside psoas sign is right lower quadrant pain when the clinician passively extends the right hip; resisted right hip flexion can reproduce the same irritation. On the right, that points at the appendix.
Notice the rule still holds: the inflamed psoas hates the motion that lengthens it (extension), just like the tight one. The difference is the source. One is a mechanical muscle problem. The other is a visceral emergency wearing the same coat.

Before the physician reaches for the treatment table, ask one question: is this muscle tight or is it irritated. A fever and a high white count beside a positive psoas sign is not a tender point, it is an appendix. Find the source first. Every time.
Tap each card to flip it. Front is the tight muscle and its action. Back is the motion it steals. Same logic, new joint.

A muscle is hypertonic. Name the motion it can no longer allow. Predict before you tap.