The muscle that sits on your sciatic nerve and squeezes when you sit. Deep buttock pain, fake sciatica, and the figure-4 stretch that fixes it.
🪑
The setup: Patient says their butt hurts. Worse when sitting. Pain shoots down the leg. You think disc herniation → but neuro exam is clean. Look at the hip: is it externally rotated? Press between the sacrum and greater trochanter → tender? That's not the disc. That's a piriformis sitting on the sciatic nerve like a bully on a park bench.
THE PATTERN
One Muscle, One Nerve, One Story
Everything about piriformis syndrome follows from anatomy.
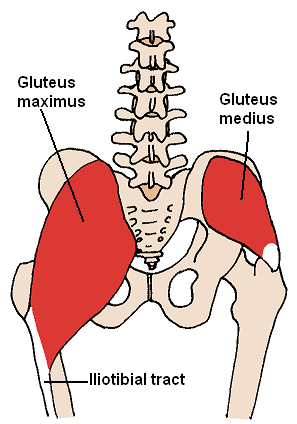
Sacrum → The piriformis originates from the anterior surface of the sacrum (S2-S4). That's why the tender point is between the lateral edge of the sacrum and the greater trochanter → you're pressing directly on the muscle belly.
Greater Trochanter → The piriformis inserts here, on the superior border. When it contracts, it pulls the trochanter posteriorly → external rotation of the hip. A tight piriformis holds the leg in external rotation at rest → that's a board clue.
Piriformis → Runs from sacrum (S2-S4) to greater trochanter. Actions: external rotation (hip extended), abduction (hip flexed). When it spasms, it compresses the sciatic nerve that runs just beneath it (or through it in ~17% of people). The spasm also holds the hip in external rotation.
Sciatic Nerve → Exits the pelvis through the greater sciatic foramenThe piriformis muscle also exits through this foramen, dividing it into a suprapiriformis and infrapiriformis space. The sciatic nerve passes through the infrapiriformis space → directly under the piriformis muscle., usually INFERIOR to the piriformis. In 17% of people, the nerve passes through or above the muscle → making them especially vulnerable to piriformis syndrome.
The link
Why Everything Happens
Follow the chain from spasm to symptoms.
Piriformis spasms→Compresses sciatic nerve→Buttock pain + leg radiation
Piriformis spasms→Pulls trochanter posteriorly→Hip externally rotated at rest
Sitting compresses piriformis→Muscle presses nerve harder→Pain WORSE with prolonged sitting
🎯
The triad: deep buttock pain + worse sitting + externally rotated hip. Add "tender between sacrum and greater trochanter" and there's only one answer.
THE FIX
The Figure-4 Stretch
The piriformis externally rotates. To stretch it, you internally rotate. Simple.
The piriformis externally rotates the hip. To stretch any muscle, you do the opposite of its action. So to stretch the piriformis, you need internal rotation + flexion + adduction. The figure-4 position achieves all three:
The Piriformis Stretch (Figure-4):
Lie supine (face up)
Cross affected ankle over the opposite knee (this creates the "4" shape)
Pull the opposite knee toward your chest
You'll feel the stretch deep in the affected buttock
Why it works: crossing the ankle over the knee puts the affected hip into flexion + external rotation. Pulling the bottom knee toward the chest then forces the affected hip into further flexion + adduction, which stretches the piriformis against its own action.
🔑Figure-4 for the floor of the pelvis. The "4" shape is the piriformis stretch → just like the number 4 when you cross your legs.
THE LINEUP
Don't Pick the Wrong Stretch
clinical medicine love asking you to identify which stretch targets which muscle. Here's the whole set.
4️⃣
Figure-4
Piriformis
🦵
Straight Leg Raise
Hamstrings
🏃
Lunge
Hip Flexors (Psoas)
🤸
Cross-Behind Lean
IT Band / TFL
🦋
Butterfly / Ext Rotation
Hip Adductors
Figure-4 (Piriformis Stretch) Position: Supine → cross affected ankle over opposite knee → pull opposite knee to chest. What it stretches: Piriformis and deep external rotators. Board clue: "Cross ankle over knee, pull knee toward chest" = piriformis. This is the ONLY stretch answer that describes the figure-4. Every other stretch position targets something else.
Straight Leg Raise / Hamstring Stretch Position: Supine → flex hip → extend knee (straighten the leg while hip is flexed). What it stretches: Hamstrings (biceps femoris, semimembranosus, semitendinosus). Board trap: "Flex hip, bring knee into extension" sounds like it could be for anything, but hip flexion + knee extension = maximal hamstring length. Hamstring injury → posterior thigh pain + can lead to posterior innominate rotation dysfunction.
Lunge (Hip Flexor Stretch) Position: Stand with one leg forward, knee bent → lean forward, extending the back hip. What it stretches: Iliopsoas and rectus femoris of the back leg. Board clue: "Stand with opposite leg forward, lean forward" = hip flexor stretch. The psoas crosses the hip joint anteriorly → extending the hip stretches it.
Cross-Behind Lean (IT Band / TFL Stretch) Position: Stand → cross affected leg BEHIND the other → lean away from affected side. What it stretches: Iliotibial band and tensor fasciae latae. Board clue: "Cross leg behind, lean to opposite side" = IT band. The IT band runs along the lateral thigh → adducting and leaning away from it puts maximal stretch on the lateral structures.
Butterfly / External Rotation (Adductor Stretch) Position: Supine → flex knee and hip → bring hip into external rotation. Or seated butterfly: soles of feet together, press knees down. What it stretches: Hip adductors (adductor longus, brevis, magnus, gracilis). Board trap: "Flex hip, external rotation" sounds similar to the piriformis stretch but it's missing the key move → pulling the opposite knee to chest. Without that pull, you're just opening the hip into external rotation, which stretches adductors, not the piriformis.
🚨
Board Trap: Adductor Stretch vs Piriformis Stretch
Both involve supine position with hip flexion. The difference: adductor stretch = external rotation of the affected hip (opening the hip outward). Piriformis stretch = cross ankle over knee + pull opposite knee to chest (creating the figure-4). The "pull toward chest" part is what makes it a piriformis stretch → it forces adduction + internal rotation against the piriformis. Without it, you're stretching adductors.
THE OMT
Osteopathic Treatment
Counterstrain and muscle energy → the two techniques they love to test.
Technique
Type
Position
Trace It
Counterstrain
Passive, indirect
Flex hip + abduct + externally rotate → hold 90 sec
Shortens the piriformis (indirect = move AWAY from barrier) → resets muscle spindle → relieves spasm
Muscle Energy
Active, direct
Patient contracts piriformis (external rotation) against resistance → then stretch into internal rotation
Post-isometric relaxation → engages barrier directly → increases ROM
💡
Counterstrain = shorten the muscle (indirect, passive). Muscle energy = contract then stretch (direct, active). Both reduce spasm → different paths, same destination.
ELIMINATION ROUND
Match the Stretch
A patient has each condition. Eliminate stretches until you find the right one for piriformis syndrome.
Loading...
Supine hip flex + knee extend
Straight leg raise
Lunge forward lean
Standing lunge
Cross behind + lean away
IT band stretch
Figure-4 pull to chest
Ankle over knee
THE ALGORITHM
Exam Day: Piriformis Rapid ID
When you see deep buttock pain, run this checklist.
Clue 1: Deep buttock pain (not posterior thigh = hamstring, not lateral hip = trochanteric bursitis)
Clue 2: Worse with sitting (sitting compresses piriformis against sciatic nerve)
Clue 3:Radiates down the leg (sciatic nerve distribution → mimics disc herniation)
Clue 4:Externally rotated hip at rest (spasmed piriformis pulling trochanter)
Clue 5: Tender between lateral sacrum and greater trochanter (you're pressing on the muscle)
Clue 6:Normal neuro exam (this is NOT a disc → no true nerve root compression)
All 6 → piriformis syndrome → figure-4 stretch + counterstrain/muscle energy
THE REVEAL
Same Pattern: Entrapment Syndromes
Piriformis isn't alone. The body loves trapping nerves.
The piriformis-sciatic relationship follows the exact same pattern as every entrapment syndrome: a nerve runs through or under a muscle, the muscle spasms or hypertrophies, the nerve gets squeezed, and you get pain + neurological symptoms in that nerve's distribution.
Syndrome
Muscle
Nerve Trapped
Symptoms
Piriformis
Piriformis
Sciatic
Buttock pain → leg
Thoracic Outlet
Scalenes / Pec Minor
Brachial Plexus
Arm pain + numbness
Carpal Tunnel
Flexor retinaculum
Median nerve
Hand tingling (1-3.5)
Cubital Tunnel
FCU aponeurosis
Ulnar nerve
Ring/pinky numbness
Same mechanism every time: structure compresses nerve → symptoms in nerve distribution → treatment = decompress. For piriformis, decompression = stretch + OMT.
THE LINEUP: IMPOSTOR CHECK
Know Your Look-Alikes
Piriformis syndrome borrows symptoms from its neighbors. Flip each card to see what makes them different.
💿
Disc Herniation
L4-L5 / L5-S1
tap to compare
Disc Herniation vs Piriformis
SLR positive→Disc
SLR negative→Piriformis
Disc: pain worsens with flexion (sitting, bending forward). Neuro deficit possible (reflexes, strength).
Piriformis: tender between sacrum and GT. Hip externally rotated. Normal neuro.
🦴
Trochanteric Bursitis
Lateral hip pain
tap to compare
Trochanteric Bursitis vs Piriformis
Bursitis: pain over the greater trochanter (lateral hip, pinpointable). No sciatic radiation.
Piriformis: pain deep in the buttock + radiates down the leg. Tender between sacrum and GT, not on top of GT.
Key: bursitis = no leg radiation. Piriformis = leg radiation from sciatic compression.
🔴
SI Joint Dysfunction
Sacroiliac pathology
tap to compare
SI Joint vs Piriformis
SI joint: tender at the PSIS / sacral sulcus (medial, over the joint). FABER test can be positive for both.
Piriformis: tender lateral to the sacral sulcus, in the muscle belly between sacrum and GT. Positive FAIR test (Flexion, Adduction, Internal Rotation provokes pain).
💪
Hip External Rotators
The 6 deep rotators
tap to learn
The Deep 6 External Rotators
All 6 exit through the greater sciatic foramen and insert near the GT. Piriformis is the LARGEST and the only one that can compress the sciatic nerve.
Piriformis (S2-S4)
Superior gemellus
Inferior gemellus
Obturator internus
Obturator externus
Quadratus femoris
🔧
Counterstrain vs MET
Two treatments, one muscle
tap to distinguish
Counterstrain vs Muscle Energy
Counterstrain: INDIRECT + PASSIVE. Move AWAY from barrier. Flex + abduct + externally rotate. Hold 90 sec. Resets muscle spindle.
Muscle Energy: DIRECT + ACTIVE. Contract against resistance (push into external rotation). Then stretch into internal rotation. Post-isometric relaxation.
Memory: Counterstrain = Comfort. Muscle Energy = Move it.
PHOTOS
Anatomy in the Wild
Real anatomy to lock in the spatial relationships. Scroll right to see all.
Piriformis muscle
Deep rotators of the hip
Sciatic nerve pathway
Greater sciatic foramen
Posterior hip muscles
×
📍
The piriformis occupies the infrapiriformis space of the greater sciatic foramen. The sciatic nerve exits BELOW it in most people. In 17%, the nerve runs through or above the muscle, making them significantly more susceptible.
🔑17% rule: roughly 1 in 6 people have a variant nerve path through or above the piriformis. These patients get piriformis syndrome more easily and more severely.
DIAGNOSIS ALGORITHM
Piriformis Syndrome: Step-by-Step
Follow the tree. Each node is clickable to reveal the reasoning.
Deep buttock pain radiating to the leg?
The first gate. Hip pain that radiates = nerve involved. If the pain stays local (lateral hip only) → bursitis. If it goes down the leg, you're in sciatic territory. Piriformis compresses the sciatic nerve → referral follows sciatic distribution (posterior thigh, calf, sometimes foot).
NO
Consider trochanteric bursitis, SI joint, local strain
No radiation = nerve not compressed. Think local structures: bursa, SI joint, hamstring origin, hip flexor. Piriformis is off the table if the pain stays put.
YES
Straight Leg Raise (SLR) positive?
SLR stretches the nerve root at the SPINE. Positive = pain reproduces = disc herniation compressing at the vertebral level. Negative SLR = the nerve root at the spine is fine. Compression is happening DOWNSTREAM → think piriformis. This single test separates disc from piriformis.
POSITIVE
Lumbar disc herniation likely → MRI lumbar spine
Positive SLR at 30-70 degrees = nerve root tension sign. Pain reproducing with passive hip flexion + knee extension = the nerve root is tethered at the spine by the disc. Get the MRI.
NEGATIVE
Hip externally rotated at rest? Tender between sacrum and GT?
Two physical exam findings that together nail piriformis syndrome. External rotation = the spasmed piriformis pulling the greater trochanter posteriorly. Tender between sacrum and GT = you're pressing on the piriformis muscle belly. Both present together = almost certainly piriformis.
NO
Revisit: consider proximal hamstring, deep gluteal syndrome
If SLR is negative but the external rotation and tender point aren't present, broaden the search. Proximal hamstring tendinopathy causes deep buttock pain. "Deep gluteal syndrome" is an umbrella term for any non-discogenic sciatic entrapment.
YES
Piriformis Syndrome → Figure-4 stretch + Counterstrain / MET
Confirmed. Treatment: Figure-4 stretch (lengthen the piriformis), counterstrain (shorten then relax), or muscle energy technique (contract then stretch). NSAIDS for inflammation. If refractory: trigger point injection or ultrasound-guided corticosteroid into the piriformis.
🎯
The FAIR test (Flexion + Adduction + Internal Rotation) is the most specific provocative test. It stretches the piriformis against the nerve → reproduces the pain. Positive FAIR + negative SLR = piriformis.
🔑FAIR test: Flex, Adduct, Internally Rotate. You're doing the OPPOSITE of what the piriformis does. If it hurts, the piriformis is the culprit.
THE ALGORITHM
Decision Tree: Piriformis Syndrome Workup and Treatment
Tap through the steps to arrive at the right diagnosis and treatment approach.
Deep buttock pain with pain on internal hip rotation and non-dermatomal leg radiation?
Differentiate piriformis from disc herniation
Lumbar disc herniation: the nerve is compressed at the vertebral level. SLR reproduces pain at 30 to 70 degrees. Get lumbar MRI. Piriformis is not the culprit here.
OMT approach: is the piriformis hypertonic or inhibited?
MET with passive internal rotation: patient resists as you move into internal rotation, then relax and stretch the hip into full IR. Repeats 3 to 5 cycles. Goal is to lengthen the spasmed piriformis.
Counterstrain: position the hip to shorten the piriformis (external rotation and slight flexion). Find and monitor the tender point at the piriformis belly. Hold 90 seconds, then slowly return to neutral. Tender point should resolve by 70 percent or more.
HVLA side-lying: hip flexed to engage the piriformis. Short, quick thrust directed toward internal rotation. Used when MET and counterstrain fail to normalize range of motion.
Local piriformis strain without sciatic involvement. Diagnose clinically: tender point between sacrum and greater trochanter, pain with hip IR, FAIR test may be mildly positive. Treat with MET or counterstrain as above. No nerve workup needed.
💪Clinical anchor: FAIR test positive plus SLR negative equals piriformis until proven otherwise. Disc herniation needs a positive SLR at 30 to 70 degrees and a dermatomal pattern.
PROVE IT
Clinical Vignettes
4 patients with various hip and buttock complaints. Match the right stretch to the right problem.
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.