Six drugs. Each one hijacks a different step of DNA synthesis. Know the enzyme, know the rescue, know the trap.
A 10-year-old boy with acute lymphocytic leukemia is on maintenance chemotherapy including 6-mercaptopurine. He develops hyperuricemia from tumor lysis and is started on allopurinol. Three weeks later he presents with severe pancytopenia. What should have been done when allopurinol was added?
Which adjustment prevents this complication?
Add leucovorin rescue
Reduce 6-MP dose by 75%
Switch to rasburicase
Monitor serum methotrexate levels
Allopurinol inhibits xanthine oxidase. 6-MP is metabolized by xanthine oxidase. Block the enzyme, the drug accumulates, the patient becomes myelosuppressed. Reduce 6-MP dose by 75% when co-administering allopurinol. This is the single most tested drug interaction in antimetabolite pharmacology.
Explore
The Pathway
Tap a drug to see where it strikes in DNA synthesis.
Methotrexate structure (DHFR inhibitor)
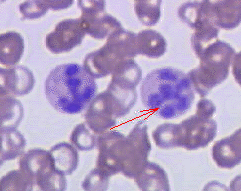
Megaloblastic anemia: hypersegmented neutrophils
Bone marrow aspiration: sampling for chemo-induced suppression
Methotrexate inhibits dihydrofolate reductase (DHFR). Without DHFR, DHF cannot be converted to THF. Without THF, there is no one-carbon donor for thymidine or purine synthesis. Result: no DNA. Rescue: leucovorin (folinic acid) bypasses the block by providing reduced folate directly.
5-Fluorouracil inhibits thymidylate synthase. This enzyme converts dUMP to dTMP (thymidine monophosphate). Without dTMP, no thymidine gets incorporated into DNA. Board trap: leucovorin enhances 5-FU (stabilizes the drug-enzyme complex). Opposite of methotrexate where leucovorin rescues.
6-Mercaptopurine is a purine analog that blocks de novo purine synthesis at the PRPP to IMP step. It is the active metabolite of azathioprine. Metabolized by xanthine oxidase and TPMT. CRITICAL: allopurinol blocks xanthine oxidase, so 6-MP accumulates. Reduce dose by 75%.
Hydroxyurea inhibits ribonucleotide reductase (RNR), which converts ribonucleotides (NDP) to deoxyribonucleotides (dNDP). Without dNDPs, no DNA precursors. Used in sickle cell disease (increases HbF), CML, and polycythemia vera.
Cytarabine (Ara-C) inhibits DNA polymerase. It is a cytidine analog that gets incorporated into DNA and terminates chain elongation. Used in acute myeloid leukemia (AML). S-phase specific.
The Drug Lineup
Tap each card to reveal the full breakdown. Every card, every mechanism, every trap.
Methotrexate▾
DHFR Inhibitor
Trace It
Inhibits dihydrofolate reductase (DHFR). No THF means no purinesTHF donates one-carbon units needed for purine ring assembly. Without it, neither AMP nor GMP can be synthesized de novo. and no thymidine.
Rescue
Leucovorin (folinic acid) bypasses the DHFR block. It IS reduced folate, so cells get THF without needing DHFR.
MTX is NOT metabolized by xanthine oxidase. Allopurinol does NOT affect MTX levels. Completely different pathway from 6-MP.
Methotrexate structure
Mucositis (MTX toxicity)
6-Mercaptopurine▾
Purine Analog
Trace It
Purine (thiol) analog. Blocks de novo purine synthesis. Active metabolite of azathioprineAzathioprine is a prodrug that is converted to 6-MP in the body. It is used as an immunosuppressant in organ transplant and autoimmune diseases.. S-phase specific.
Metabolism
Two pathways: xanthine oxidase and TPMT. Both produce inactive metabolites.
The Interaction
Allopurinol blocks XO. Now only TPMT can clear 6-MP. Drug accumulates to toxic levels. Reduce dose by 75%.
TPMT polymorphisms: some patients have low TPMT activity at baseline. These patients are already at risk for 6-MP toxicity even WITHOUT allopurinol. Genotyping before starting therapy.
5-Fluorouracil▾
Pyrimidine Analog
Trace It
Pyrimidine analog. Converted to 5-FdUMP, which covalently inhibits thymidylate synthase. Blocks dUMP to dTMP conversion.
The Leucovorin Trap
Leucovorin + 5-FU = ENHANCED toxicity. Leucovorin provides the reduced folate cofactor that stabilizes the 5-FdUMP/thymidylate synthase complex. This is the OPPOSITE of MTX, where leucovorin rescues.
Same drug (leucovorin), opposite effect. MTX = rescue. 5-FU = enhance. clinical medicine love this one.
Hydroxyurea▾
RNR Inhibitor
Trace It
Inhibits ribonucleotide reductase (RNR). This enzyme converts ribonucleotides to deoxyribonucleotides. Without deoxyribonucleotides, no DNA precursors.
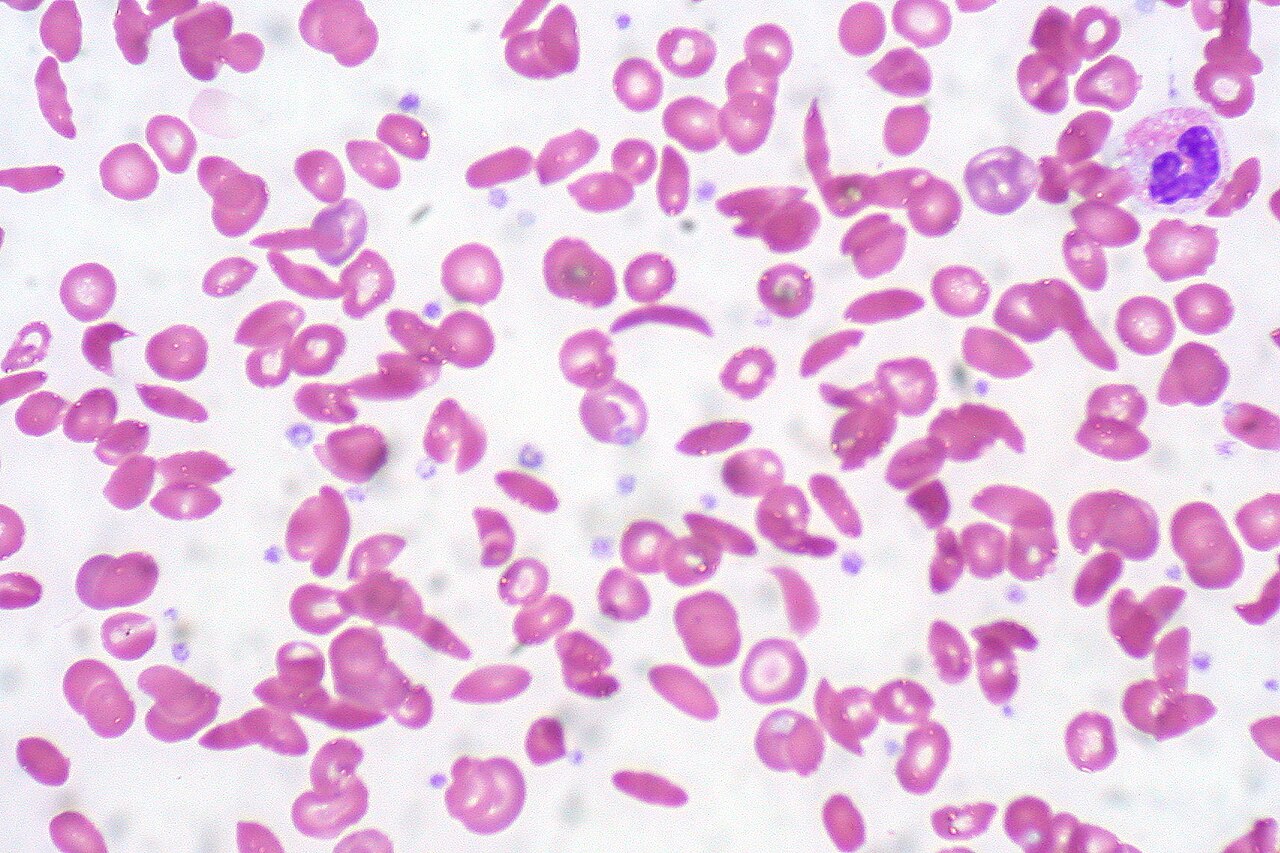
Sickle Cell Use
Increases fetal hemoglobin (HbF). HbF does not polymerize with HbS, reducing sickling frequency and vaso-occlusive crises. Also used in CML and polycythemia vera.
Only chemo drug given CHRONICALLY for sickle cell. The HbF mechanism is why it works for a non-cancer condition.
Cytarabine (Ara-C)▾
DNA Polymerase Inhibitor
Trace It
Cytidine analog. Inhibits DNA polymerase. Gets incorporated into DNA and terminates chain elongation. S-phase specific.
Clinical Use
Acute myeloid leukemia (AML). Part of the "7+3" regimen7 days of cytarabine continuous infusion plus 3 days of an anthracycline (daunorubicin or idarubicin). Standard induction for AML..
Toxicity
Myelosuppression, cerebellar toxicity at high doses (ataxia, dysarthria)
The cerebellar toxicity at high doses is a board pearl. Patient on Ara-C who develops ataxia = high-dose cytarabine neurotoxicity.
Cyclophosphamide▾
Alkylating Agent
Trace It
Alkylating agent. Cross-links DNA (not an antimetabolite, but tested alongside them). Requires hepatic activation via CYP450 to produce phosphoramide mustardThe active DNA-damaging species. It alkylates guanine bases at the N7 position, creating interstrand crosslinks that prevent DNA unwinding and replication..
Unique Toxicity
Hemorrhagic cystitis from acrolein (a toxic byproduct). Prevention: MESNA (binds acrolein in the bladder) + aggressive hydration.
MESNA for cyclophosphamide is the same logic as leucovorin for MTX: a rescue agent for a specific toxicity. Know the pairs.
Elimination Game
Read the vignette. Reveal clues one at a time. Eliminate drugs that don't fit.
A 10-year-old boy with acute lymphocytic leukemia is on maintenance chemotherapy. After tumor lysis prophylaxis with allopurinol, he develops severe pancytopenia. Which chemotherapy agent's dose should have been reduced?
6-Mercaptopurine
Methotrexate
Cyclophosphamide
Cisplatin
Vincristine
Clue 1: Allopurinol inhibits xanthine oxidase. Which drug on this list is metabolized by xanthine oxidase?
Clue 2: Cyclophosphamide is an alkylating agent. Cisplatin is a platinum agent. Vincristine is a vinca alkaloid. None of these use XO for metabolism. All eliminated.
Clue 3: Methotrexate inhibits DHFR. It is NOT metabolized by xanthine oxidase. Leucovorin rescues MTX toxicity. Allopurinol has no effect on MTX.
Clue 4: 6-MP is metabolized by XO and TPMT. Block XO with allopurinol, and 6-MP accumulates to toxic levels. Must reduce dose by 75%.
6-Mercaptopurine. 6-MP is metabolized by xanthine oxidase. Allopurinol blocks XO, so 6-MP accumulates. The dose must be reduced by 75% to prevent fatal myelosuppression. This is the #1 tested drug interaction on the clinical medicine.
A patient on methotrexate for rheumatoid arthritis develops severe pancytopenia and oral ulcers. What is the rescue agent?
Leucovorin
MESNA
Allopurinol
N-Acetylcysteine
Dexrazoxane
Clue 1: MTX blocks DHFR, preventing THF synthesis. The rescue must bypass this block by providing reduced folate directly.
Clue 3: Allopurinol blocks xanthine oxidase. MTX is NOT metabolized by XO. Allopurinol has absolutely no role in MTX toxicity.
Clue 4: Leucovorin IS folinic acid (5-formyl THF). It skips the DHFR step entirely, feeding reduced folate directly into the pathway.
Leucovorin (folinic acid). It bypasses the DHFR block by providing reduced folate directly to the cell, rescuing normal cells from methotrexate toxicity while cancer cells (which have higher MTX uptake) remain suppressed.
A patient with sickle cell disease has recurrent vaso-occlusive crises. The hematologist prescribes a medication to increase fetal hemoglobin (HbF) levels. Which drug?
Methotrexate
Hydroxyurea
5-Fluorouracil
Cytarabine
6-Mercaptopurine
Clue 1: Only one of these drugs is used chronically in a non-cancer condition. The others are strictly oncology drugs.
Clue 2: HbF does not polymerize with HbS. More HbF means fewer sickle cells. The drug must upregulate fetal hemoglobin production.
Clue 3: The drug inhibits ribonucleotide reductase but also has a separate mechanism of increasing HbF through stress erythropoiesis and epigenetic modification.
Clue 4: Also used in CML and polycythemia vera (cytoreduction to lower cell counts).
Hydroxyurea. It inhibits ribonucleotide reductase AND increases HbF. More HbF means less HbS polymerization, fewer sickle cells, fewer vaso-occlusive crises, and reduced acute chest syndrome episodes. The only chemo drug given long-term for sickle cell.
clinical Walkthrough
Full vignettes with clue highlights. Pick your answer, then walk through every option.
QUESTION 1 OF 25
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated June 30, 2026 at 10:26 AM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.