Vault hold, V-spread, CV4, sphenopalatine release, and the suboccipital decompression that calms the vagus. Pick the right hand for the right autonomic problem.
Quick Challenge
A 28 year old with chronic congestion, post-nasal drip, and refractory sinusitis comes in for adjunctive OMT after maximal medical therapy. Which cranial technique most directly drains the sinuses by releasing the ganglion in the pterygopalatine fossa?
Scroll to learn the patterns ↓
Why these techniques exist
Four cranial nerves carry parasympathetic fibers out of the brainstem. They squeeze through tiny bony exits. Compress the exit, you choke the nerve. Open the exit, the nerve glides. That is the entire premise of cranial PSNS work.
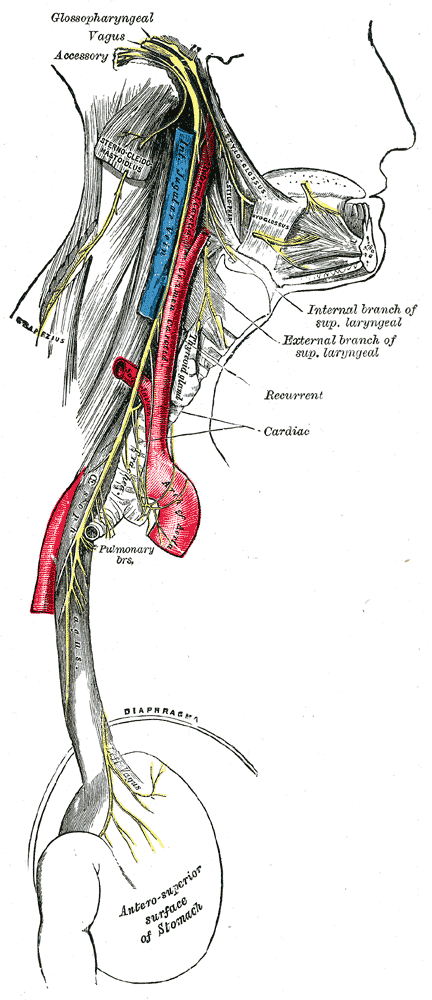
🧠CN III, VII, IX, X carry the cranial parasympathetics. Their nuclei live in the brainstem, their fibers exit through the skull, and their endings drive pupil, glands, heart, lung, and gut down to the splenic flexure.
Click a bone to see what nerve it gates and which technique opens it
Tap a bone above to see which cranial nerve passes through and which OMT addresses it.
The pathway in one diagram
Brainstem nucleus → cranial nerve → ganglion → target organ. Same template for all four PSNS cranial nerves.
III
ciliary ganglion
cil
→
Pupil · lens
VII
pterygopalatine ganglion
PPG
→
Tears · nose
submandibular ganglion
SMG
→
Submand · subling
IX
otic ganglion
otic
→
Parotid (spit)
X
terminal ganglia in organ wall
→
Heart · lung · gut
down to splenic flexure
For the full PSNS spinal map (with sacral S2 to S4 and sympathetic levels), see the autonomic levels page. This page is about HOW you treat through these channels.
The five techniques
Pick a tab. Each technique gets indication, hand placement, what you do, the endpoint, and the contraindications.
Vault Hold
The diagnostic listening hand. Treatment is by intent, not push.
Indication
Diagnose strain patterns, palpate the cranial rhythmic impulse CRI~10 to 14 cycles per minute. Slow, gentle, biphasic. Felt as a flexion-extension whisper through the bone. (about 10 to 14 cycles per minute), assess flexion vs extension dysfunction.
Hand placement (5-finger)
Index on greater wings of sphenoid. Middle on temporals. Ring on parietals. Fifth on occipital squama. Thumbs crossed overhead, not on the head.
What you do
Listen. Do not push. Note the rate, amplitude, and symmetry of the CRI. Indirectly treat by intent: hold the cranium toward its still point until tissue releases.
Endpoint
A still point arrives, then the rhythm restarts broader and more symmetric.
Contraindications
Skull fracture, recent intracranial hemorrhage, increased ICP, acute severe TBI.
V-Spread (Sutural Spread)
Aim a fluid wave at the stuck suture from across the skull.
Indication
Focal sutural restriction, cranial nerve foramen compression, sinus drainage assist (V-spread the maxillary or sphenoid sutures), post-traumatic suture binding.
Hand placement
V (index + middle) on the side OPPOSITE the restricted suture, fingertips pointing AT the suture. Other hand sits on the directly opposite side of the skull as the fluid driver.
What you do
Drive hand pumps a gentle fluid wave across the cranium toward the V. The V "catches" the wave and the suture spreads under your fingertips.
Endpoint
Tissue release felt at the suture. Patient often reports immediate symptom shift (sinus pop, drainage, pressure relief).
Contraindications
Skull fracture, recent ICH, increased ICP, infection at contact site.
CV4 · Compression of the 4th Ventricle
The classic parasympathetic-boosting still point. Cradle the occiput, ride to silence.
View from above → patient supine
☑
Hypothenar eminences on occipital squama
☑
Medial to occipitomastoid sutures
☑
Thumbs touch or interlace overhead
✗
Do not contact suboccipital muscles
Indication
Fever, congestion, sinusitis adjuvant, autonomic dysregulation, sleep disturbance, tension headache. Considered the strongest cranial parasympathetic boost.
Hand placement
Bilateral hypothenar eminences cradle the occipital squama, MEDIAL to the occipitomastoid sutures. Thumbs touch or interlace overhead. Stay off the suboccipital muscles.
What you do
During cranial flexion, gently follow. During extension, RESIST. Encourage compression, discourage extension, until a still point arrives. Hold quietly. Release.
Endpoint
Still point felt. Patient often sighs, body warms, breathing deepens. Then CRI restarts broader and symmetric. Increased amplitude of CRI is the textbook outcome.
Contraindications
Absolute: skull fracture, recent intracranial hemorrhage, acute stroke, increased ICP, severe TBI. Relative: pregnancy uncertainty, active seizure disorder.
Sphenopalatine Ganglion Release
Reach the ganglion that runs the lacrimal, nasal, and palatine glands. Open the sinus.
Modern preference is extra-oral: gloved fingertip pressure on the lateral face just inferior to the zygomatic arch, aiming toward the pterygopalatine fossa. Intranasal cotton applicator and intra-oral contact (finger to pterygoid plate) are also taught and require explicit consent.
What you do
Gentle, sustained pressure for 30 seconds to 2 minutes. Wait for tissue softening. Patient may report drainage relief, nasal pop, or eye watering as the ganglion fires.
Patient supine. Physician seated at head of table. Finger pads slip just under the inferior nuchal line bilaterally. Skull rests on your fingertips. For OA: add gentle sidebending and rotation to engage barriers. For AA: pure rotation.
What you do
Sustained, slow pressure for 1 to 3 minutes. The skull settles into your hands as the suboccipital muscles release. Theoretical effect: reduce tension on the dura and the jugular foramen exit, freeing vagal nerve glide.
C1-C2 instability (Down syndrome, severe RA, Klippel-Feil), vertebral artery dissection history or vertebrobasilar insufficiency symptoms (dizziness or syncope on cervical motion), acute cervical fracture.
🤩Supporting roles: Frontal lift opens the superior orbital fissure (CN III, IV, V1, VI exits). Parietal lift addresses parietal restrictions. Temporal rocking influences CN VII through the internal acoustic meatus and CN IX, X, XI through the jugular foramen.
Pick the technique
Six clinical scenarios. Pick the cranial OMT that fits best. The board loves these matchups.
Case 1 of 6
Loading scenario...
Symptom → technique cheat grid
Sinusitis adjunct
SPG release + V-spread
Open the maxillary sutures, fire the ganglion that drives lacrimal and nasal glands. Add lymphatic pump.
Acute severe traumatic brain injury or active coup-contrecoup
Uncontrolled hydrocephalus
CSF leak or recent neurosurgery
Decision tree: should you treat this skull?
A 48 year old comes in 4 days after an MVA. CT was negative for fracture and bleed. She wants OMT for her headache. Safe for cranial work?
Yes, go ahead
Yes, with caution and a recheck
')">No, never within a month
A 6 year old with Down syndrome has constipation. Mom asks for cranial OMT. You consider OA / suboccipital decompression to boost vagal tone. Best move?
Proceed with bilateral OA decompression
CV4 instead, plus abdominal techniques
Skip OMT entirely
A 32 year old reports a severe headache yesterday described as "the worst of my life," now resolved. She wants CV4 for sleep. What do you do?
Proceed with gentle CV4
Vault hold only, no compression
Refer for urgent workup, no cranial OMT today
Memory hooks
🧠
Cranial PSNS = "3, 7, 9, 10"
Four nuclei. Edinger-Westphal (III) for the pupil, superior salivatory (VII) for tears and submandibular spit, inferior salivatory (IX) for parotid spit, dorsal motor (X) for everything from heart to splenic flexure. Memorize the four numbers and you own the cranial PSNS.
tap to reveal
🍻
CV4 = "cradle, compress, count to silence"
Hands cradle the occiput. Resist extension during cranial cycle. Wait for the still point (the silence). When the rhythm restarts broader, you are done. Three Cs ride the technique from start to finish.
tap to reveal
👀
SPG = "the sinus thermostat"
The sphenopalatine ganglion runs the lacrimal, nasal, and palatine glands. Squeeze the right zone and you can shift sinus secretion the way a thermostat shifts a room. That is why one technique helps allergic rhinitis, sinusitis, and even cluster headache adjunctively.
tap to reveal
☠
"Bleeders, breakers, balloons"
Three buckets of absolute no: bleeders (recent ICH or stroke), breakers (skull fracture or severe TBI), balloons (raised ICP or hydrocephalus). Touch nothing on the vault until each bucket is ruled out.
tap to reveal
📷 Vagus nerve: thoracic and abdominal branches · tap to expand
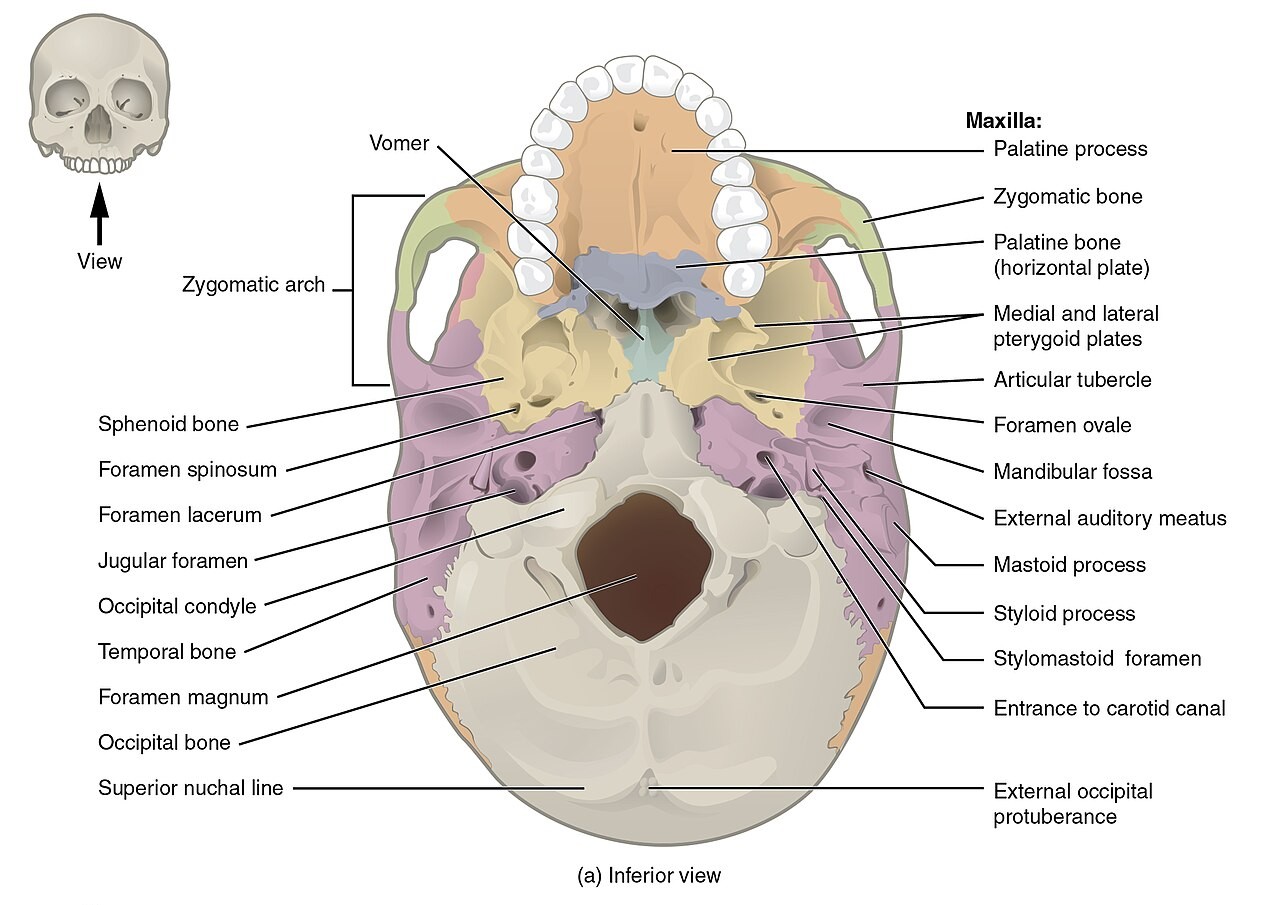
📷 Skull base: foramina that gate the cranial nerves · tap to expand
📷 CN VII: facial nerve and its parasympathetic branches · tap to expand
Quiz
Five rotating questions per load. Pulled from a pool of eight. Refresh to see different ones.
Loading...
Medically reviewed by Fatima Ali, DO and Kaitlyn Cocuzzo, MD · Last updated July 1, 2026 at 10:03 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.