Sympathetic spinal levels. Parasympathetic cranial and sacral. Splanchnic pathways. The map under every viscerosomatic finding and every ANS-targeted technique.
Match The Organ To Its SNS Level
Click an organ on the body. Pick its sympathetic cord level. Eight organs, one shot each, score climbs.
CORRECT 0
OF 0 / 8
Click any organ on the body to start.
From the Attending
SNS levels track the gut tube. Foregut T5−T9, midgut T10−T11, hindgut T12−L2. Heart is its own beast at T1−T5. The bladder splits: SNS T11−L2 stores, PSNS S2−S4 voids. Click all eight to drill it in.
The Core Clue
Every organ has TWO drivers. Sympathetic wires in from the thoracolumbar spine (T1 to L2). Parasympathetic wires in from cranial nerves and S2 to S4. Both lines meet at the organ. OMT taps the WIRE, not the organ.
Two systems, two highways
Pull the right lever and the organ's tone changes. The lever is the spinal segment or the cranial nerve, NOT the organ itself. Once you have the highways memorized, every viscerosomatic finding and every autonomic OMT becomes obvious.
Vagus does most viscera; pelvic splanchnics finish the colon
The four-question algorithm for every ANS stem
What organ is mentioned?
Sympathetic level for that organ?
Parasympathetic source for that organ (vagus or pelvic)?
Which OMT calms or fires the matching wire?
📷 Anatomy schematic: SNS + PSNS outflow · tap to expand
Board Pearl
The spinal sympathetic outflow stops at L2. Anything below L2 that "looks" sympathetic is actually fibers from the lumbar chain riding caudally. The cord itself never sends a sympathetic fiber out below L2.
Memory hooks
🔥
SNS = Thoracolumbar
"Stress lives in the thorax." T1 starts the gas pedal at the heart. L2 is the last fiber out the door. Above T1 and below L2: zero sympathetic outflow from the cord.
tap to reveal
🌚
PSNS = Craniosacral sandwich
Brainstem at the top, sacrum at the bottom, sympathetic in the middle. The vagus is the long arm of the sandwich, reaching all the way down to the splenic flexure of the colon.
tap to reveal
💰
"Pay 1974" rule
CN 3, 7, 9, 10: the only cranial nerves with parasympathetic fibers. Three, seven, nine, ten. The other CNs do not carry PSNS.
tap to reveal
From the Attending
Stop memorizing every level. Sympathetic outflow lives in the thoracolumbar (T1·L2) IML · nothing below L2 ever leaves the cord as a sympathetic fiber. Parasympathetic outflow is craniosacral · CN III, VII, IX, X cranially, and S2·S4 caudally. If the stem says "pre-ganglionic sympathetic from L4" it's wrong · the cord can't do that. The lumbar chain just hands fibers down. Anchor the levels first, the organs second.
Sympathetic spinal level map
The IML (intermediolateral cell column) of the spinal cord between T1 and L2 is the entire factory floor for sympathetic outflow. Tap any segment on the spine. The right panel shows which organs that segment fires, which ganglion the fibers synapse in, and the clinical medicine-style buzzword.
Tap a segment. Organs and pathway will light up.
Tap T1-T4 / T5-T9 / T10-11 / T12-L2 / S2-S4
Tap a segment on the spine to see the organs it innervates, the splanchnic pathway, and the clinical medicine-style memory cue.
Splanchnic nerves (the SNS pre-ganglionic shipping lanes)
Pre-ganglionic sympathetic fibers exit the cord, pass STRAIGHT THROUGH the chain ganglia without synapsing, and form named splanchnic nerves that travel forward to abdominal ganglia. Tap a splanchnic to see its lane.
Greater splanchnic (T5-T9): exits the cord at T5 to T9, travels DOWN past the sympathetic chain WITHOUT synapsing, pierces the diaphragm, and synapses in the celiac ganglion. Post-ganglionic fibers then innervate the foregut (esophagus, stomach, liver, gallbladder, spleen, duodenum, pancreas, proximal to the ligament of Treitz).
Sacral Splanchnic Trap
Sacral splanchnics are SYMPATHETIC fibers from the lumbar chain riding down. Pelvic splanchnics are PARASYMPATHETIC fibers from S2 to S4. The names are nearly identical and the clinical medicine love this trap. Pelvic = parasym. Sacral = sym.
From the Attending
The splanchnic naming is the test favorite. Greater (T5·T9) → celiac → foregut.Lesser (T10·T11) → superior mesenteric → midgut.Least (T12) and lumbar → aorticorenal/inferior mesenteric → hindgut/kidneys. They all skip the chain · pre-ganglionic fibers pass through and synapse on the organ side. If a stem describes early periumbilical appendicitis pain, that's referred sympathetic from T10·T11 midgut. The cord, not the appendix, decides where it hurts.
Parasympathetic: cranial + sacral only
Four cranial nerves carry parasympathetics: CN III, VII, IX, X. Then S2 to S4 finish the bottom of the GI and pelvis. Tap a node on the diagram below to see the nucleus, the ganglion, and the target.
Tap a cranial nerve node or the sacral block to load nucleus · ganglion · target.
The vagus / pelvic handoff
The single most testable PSNS fact: vagus drives EVERYTHING above the splenic flexure. Pelvic splanchnics (S2 to S4) take over from the splenic flexure DOWN.
Quick check: which PSNS source innervates the descending colon?
Vagus (CN X)
Pelvic splanchnics (S2 to S4)
Sacral splanchnics
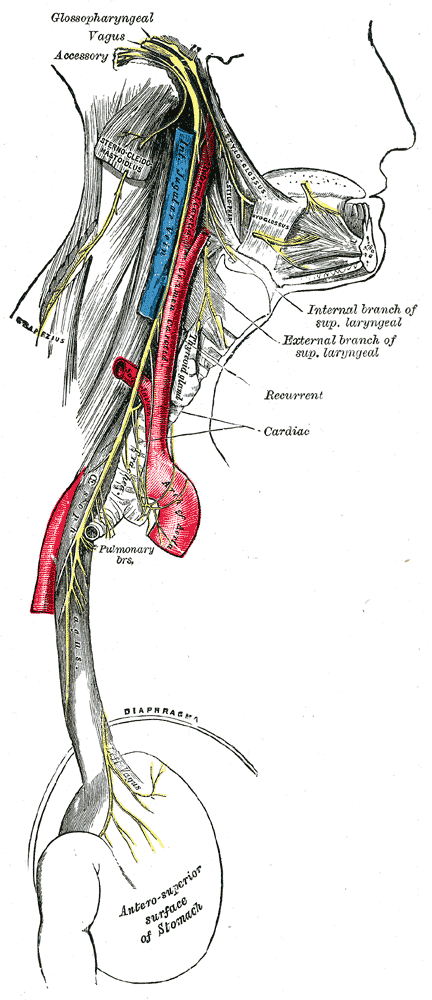
📷 Vagus nerve: thoracic and abdominal branches · tap to expand
Asthma + Vagus
Vagus drives bronchoconstriction + mucus secretion. Asthma is functionally a parasympathetic-skewed bronchospasm. Sympathetic fibers (T2-T7) bronchodilate via beta-2 receptors. That is why every asthma OMT picks rib raising (calm SNS chain, balance the autonomic teeter-totter) plus suboccipital release (modulate vagus).
From the Attending
Parasympathetic doesn't reach the lower colon. CN X (vagus) runs out at the splenic flexure · everything distal (descending colon, sigmoid, rectum, bladder, lower GU) is on pelvic splanchnics (S2·S4). Cauda equina injury → lose pelvic splanchnics → neurogenic bladder/bowel below that line. Stem says "trouble emptying the bladder after a sacral fracture"? That's S2·S4, not vagus. The vagus never had that turf.
Memory hooks
👨
Vagus = "from the brain to the bowel"
Then it stops. Splenic flexure of the colon is the brick wall. Below that, the body builds a different parasympathetic line out of the sacrum.
tap to reveal
👀
CN III makes the pupil small
Edinger-Westphal sends fibers via CN III to the ciliary ganglion to the iris constrictor. Lose CN III parasympathetics: pupil blows wide open. Classic uncal herniation sign.
tap to reveal
😯
"Spit, weep, dribble"
CN VII = lacrimal (weep) + submandibular/sublingual (dribble). CN IX = parotid (spit). All cholinergic muscarinic. Block them and your patient gets dry eyes and dry mouth.
tap to reveal
Viscerosomatic reflex: the wire becomes the symptom
Visceral afferent fires up the SAME spinal segment as the sympathetic outflow. The cord then sensitizes the somatic side at that segment. Result: palpable tissue texture change, hypertonicity, skin temperature shift in the paraspinal region one segment off-center from the affected organ's SNS level.
Chronic: ropy, fibrotic, cool, dry, pale paraspinal tissue.
Always palpate one to two finger-widths off midline at the segment level.
Findings persist after the visceral problem resolves (chronic cases) - so you can read it like a fingerprint.
The decision
Stem describes an organ symptom: ask "what SNS spinal level?" then check that paraspinal segment. The answer is the level from the spinal map, not the organ itself.
Five short stems. Pick the SNS level where you'd expect paraspinal tenderness. Same logic the clinical medicine use.
Stem 1 of 6
All six locked in. The level IS the answer.
OMT targets: turn the dial up or down
Decrease sympathetic tone
Rib raising (T1-T12): paraspinal/costovertebral mobilization. Direct contact on the chain ganglia along the rib heads. Workhorse for hospitalized patients with autonomic overdrive.
Paraspinal inhibition: sustained pressure (~90 sec) on hypertonic paraspinal soft tissue at the involved segment. Drains the sensitization.
Thoracic soft tissue / lift: lengthens the paraspinal mass, decongests the chain.
clinical medicine
Rib raising for the post-op ileus, asthma exacerbation, hospitalized pneumonia, and the patient with hypertensive urgency from autonomic dysregulation. If the stem hands you a cardiopulmonary or upper-GI complaint with no contraindication, rib raising is on the answer list.
Increase parasympathetic tone
OA / AA / C2 release (suboccipital release): opens the jugular foramen region and modulates vagal tone. Used for visceral PSNS upregulation above the splenic flexure.
Cranial: CV4, vault hold, V-spread: classic cranial techniques, all designed to restore the inherent rhythm and tip the autonomic balance toward PSNS.
Sacral rocking (S2-S4): gentle rhythmic motion of the sacrum to address pelvic splanchnic tone. The OMT pick for descending colon constipation, urinary retention, and pelvic-floor dysfunction.
clinical medicine
OA release for upper-GI/post-vagotomy reflux. Sacral rocking for the elderly post-op constipation case where the descending colon will not move.
Abdominal ganglion inhibition
Sustained anterior abdominal pressure over the named ganglion. Calms post-ganglionic SNS firing into that organ field. Match the ganglion to the organ.
Ganglion
Spinal source
Target field
Celiac
T5-T9
Foregut: stomach to mid-duodenum, liver, gallbladder, pancreas, spleen
Six clinical scenarios. Pick the right OMT for the autonomic goal. One try per stem; explanations show after you commit.
From the Attending
OMT picks track autonomics, not muscles. Hypersympathetic organ → rib raising (T1·T12 to calm SNS chain) or ganglion inhibition over the matching collateral (celiac for foregut, SMG for midgut, IMG for hindgut). Hypoparasympathetic organ above splenic flexure → suboccipital release / OA decompression (vagus). Below splenic flexure → sacral rocking (S2·S4 pelvic splanchnics). Match the lever to the level. The board never asks you to "guess the gentle technique" · it asks which autonomic line you're trying to move.
clinical quiz
Eight questions. Original stems. Same energy as the levels you'll see in clinical practice. Tap your pick, see the chain.
From the Attending
Quiz strategy: read the last sentence first. "Which paraspinal level?" → map organ to SNS segment (foregut T5·T9, midgut T10·T11, hindgut T12·L2, head/neck T1·T4, heart T1·T5, lungs T2·T7, kidneys T10·T11, ureters T10·L1, uterus T10·L2). "Which OMT?" → match the autonomic line. Cross out anything that gives a sympathetic answer below L2 or a parasympathetic answer between splenic flexure and S2. The cord can't break its own rules.
Medically reviewed by Fatima Ali, DO and Kaitlyn Cocuzzo, MD · Last updated July 5, 2026 at 8:04 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.