Where the lesion lives determines what's lost. Map the tracts and the deficit becomes a diagnosis.
Opening Challenge
A 28-year-old man is involved in a motor vehicle accident. He presents with
right-sided hemiparesis and loss of right-sided proprioception and vibration
below the level of injury, AND loss of pain and temperature sensation on the LEFT side below
the injury. Upper motor neuron signs on the right. He can walk haltingly.
Correct: Brown-Sequard syndrome.
Brown-Sequard is the key mismatch syndrome. The deficits are ipsilateral motor + proprioception loss
combined with contralateral pain and temperature loss. Why the split?
Corticospinal and dorsal columns travel ipsilaterally in the cord and only cross at the medulla. A cord hemisection hits them on the same side as the lesion.
Spinothalamic tract decussates in the cord within 1 to 2 spinal segments. So a cord lesion knocks out the contralateral ascending signal slightly below the lesion.
Anterior cord would lose bilateral motor and pain/temp but preserve proprioception. Complete transection loses everything bilaterally. Neither fits.
Section 1 of 8
Tract Map
Three major tracts, three rules. Master these and every syndrome falls out logically.
Clinical Images
Tract geography · dorsal, lateral, anterior · tap to expand
Cord cross-section · lesion geography · tap to expand
Decussation map · why side flips matter · tap to expand
Corticospinal Tract (Motor)
MotorUMN / LMN
Path: Descends ipsilaterally through the cortex and brainstem until the
pyramidal decussation at the medulla, then crosses to the contralateral lateral corticospinal tract.
Key rule: A spinal cord lesion is BELOW the decussation. So the cord carries the
ipsilateral motor signal. Cord lesion = ipsilateral weakness.
UMN signs (cord lesion): spasticity, hyperreflexia, Babinski sign, loss of fine motor control.
No atrophy.
LMN signs (anterior horn cell):ipsilateral flaccid weakness, atrophy,
fasciculations, hyporeflexia. Same side as the damaged cell body.
Somatotopic layout: Cervical fibers run centrally, lumbar fibers run laterally. Central cord injury
hits arms > legs.
Dorsal Columns (Proprioception, Vibration)
Sensory
Modalities carried: vibration, proprioception (joint position), fine touch, two-point discrimination.
Path: Ascends ipsilaterally in the posterior cord until the
nucleus gracilis and cuneatus at the medulla, where it decussates as the medial lemniscus.
Cord lesion rule: Because crossing happens at the medulla, a cord injury gives
ipsilateral proprioception and vibration loss below the lesion.
Tests to know: Romberg test (swaying with eyes closed), finger-nose ataxia, heel-shin test, inability to detect tuning fork vibration.
Path: Sensory neuron enters the dorsal horn, synapses, and
decussates in the cord within 1 to 2 spinal segments in the anterior commissure.
Then ascends contralaterally to the thalamus.
Cord lesion rule: Because crossing happens immediately in the cord, a cord injury gives
contralateral pain and temperature loss
1 to 2 levels below the lesion (the signal already crossed before ascending).
The mismatch: Dorsal columns and spinothalamic cross at different levels. This is
the entire reason Brown-Sequard syndrome produces a level-split sensory picture.
Dorsal columns stay same side until the brainstem. Spinothalamic crosses immediately in the cord.
This mismatch creates every classic spinal cord syndrome.
Vibration with a tuning fork and great-toe up/down testing are dorsal column checks. Pinprick and hot/cold are spinothalamic checks. A distal stocking-glove gradient points away from a single cord level and toward peripheral neuropathy.
The spinal cord ends around L1-L2 as the conus medullaris. Below that, the canal contains cauda equina nerve roots, so lumbar puncture is aimed lower and new saddle anesthesia plus bladder trouble gets sorted into conus versus cauda.
1 / 8
Section 2 of 8
Most Common Causes
Tap a syndrome. The cross-section lights up exactly which tracts go down and tells you the single cause boards love to test.
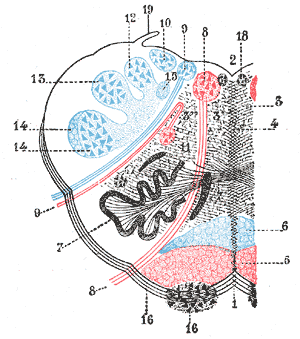
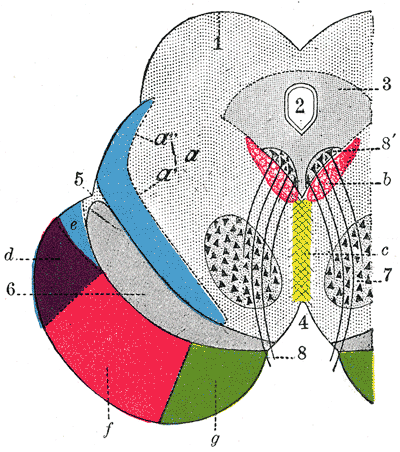
Axial Cross-Section · Cervical
Cord Cross-Section · Live Map
PictureNormal cord cross-section. All three tracts intact. Tap a syndrome to watch which tracts go down and which stay live.
CauseSelect a syndrome to load the single most-tested cause.
See ItPatterns below.
Cervical axial view · anterior at top
Anterior cord = anterior spinal artery emboli or injury (often aortic surgery). Central cord = trauma + hyperextension in the elderly, or syringomyelia in the young. Brown-Sequard = penetrating trauma (stab or bullet).
2 / 8
Section 3 of 8
The Syndromes
Tap each card to reveal the full clinical picture. Know what's lost, what's spared, and why.
Brown-Sequard
Hemisection · Best prognosis
Select to reveal
Ipsilateral:UMN weakness (corticospinal) + vibration/proprioception loss (dorsal columns)
Contralateral:pain and temperature loss (spinothalamic crosses in the cord within 1 to 2 segments)
Prognosis:best of all incomplete SCI syndromes
Patient can often still walk (contralateral motor partially intact)
Most common cause:PENETRATING TRAUMA (stab wound, gunshot) producing hemisection. Also: MS demyelinating plaque, tumor, disc herniation. What will you do next time? Stab to neck or back → think Brown-Sequard first.
Central Cord
Arms > Legs · Most common incomplete SCI
Select to reveal
Motor:bilateral arm weakness > leg weakness (CAPE distribution: cervical fibers most central)
Bladder: dysfunction (urinary retention common)
Sensory: variable loss; hands most affected
Leg strength often preserved enough to walk
Two most common causes:TRAUMA (whiplash / hyperextension: elderly fall, MVC rear-end) AND SYRINGOMYELIA (cystic cavity in cord, often with Chiari). Mechanism: central damage hits crossing spinothalamic fibers at the anterior commissure first → bilateral cape pain/temp loss. Cervical fibers run most central in CST → hand-first weakness.
Anterior Cord
Worst prognosis · Proprioception SPARED
Select to reveal
Bilateral loss:motor (corticospinal) + pain and temperature (spinothalamic)
Preserved:vibration and proprioception (dorsal columns, posterior cord, not supplied by anterior spinal artery)
Prognosis:worst of incomplete syndromes
Most common cause:EMBOLI OR INJURY TO THE ANTERIOR SPINAL ARTERY (ASA supplies the anterior two-thirds). Classic: aortic aneurysm surgery (cross-clamping), aortic dissection, atherosclerosis, hypotension. Watershed at T4 to T8. Burst fracture impinging the anterior cord also fits.
Pathology: TDP-43 aggregates, SOD1 mutation (familial). Both UMN (lateral corticospinal) and LMN (anterior horn cells) degenerate simultaneously.
Polio
Anterior horn cells · LMN only
Select to reveal
Target: anterior horn motor neurons
Motor:asymmetric flaccid weakness, legs often worse than arms
Reflexes:hyporeflexia with atrophy and fasciculations
Sensory:intact, because posterior horn and sensory tracts are spared
Cause: poliovirus. Classic stem: unvaccinated child, febrile prodrome, then flaccid paralysis a few days later. Anterior horn = LMN weakness with no sensory level.
Spinal Muscular Atrophy
Floppy baby · Tongue fasciculations
Select to reveal
Target: anterior horn cells, like polio, but inherited
Cause: autoimmune CNS demyelination. If the cord pattern is weirdly focal but the history has optic neuritis or separate neurologic attacks, load MS as the mechanism.
Cauda vs Conus
Roots below L1-L2 · Saddle and bladder
Select to reveal
Cauda equina: nerve-root problem below the cord. Gradual, asymmetric radicular leg pain, LMN signs, urinary retention, saddle anesthesia.
Conus medullaris: cord-end problem at L1-L2. More sudden, bilateral/symmetric, early bladder and bowel dysfunction, perianal anesthesia.
Decision rule: roots scream pain and asymmetry; conus declares bladder and bilateral saddle findings early.
Cause: disk herniation, tumor, trauma, or compression at the cord ending. The dedicated cauda/conus localizer lives in Neuro for deeper sorting.
3 / 8
Section 4 of 8
B12 and the Posterior Columns
Two classic cord diseases that live in the dorsal cord. High-yield for clinical practice. Know both.
Classic board clue: Absent ankle jerks (LMN peripheral neuropathy) + hyperreflexia at the knee
(UMN lateral column) in the SAME exam. This paradox is B12.
Lab clue:macrocytic anemia (megaloblastic) + neurologic deficits = think B12 first.
MMA (methylmalonic acid) is the most sensitive test.
Schilling test (historical): distinguishes intrinsic factor deficiency from dietary deficiency.
Tabes Dorsalis (Tertiary Syphilis)
Posterior Columns Only
Cause:Treponema pallidum, tertiary (late) neurosyphilis.
Demyelinates the dorsal root ganglia and posterior columns. No lateral column involvement
(unlike SCD, no UMN signs).
Classic findings:
Lancinating "lightning" pains: sudden shooting pains in legs, often nocturnal
Argyll Robertson pupil: "accommodates but doesn't react." Brisk near reflex (pupil constricts when focusing near) but NO light reflex (pupil doesn't constrict to direct light). Lesion: dorsal midbrain
Positive Romberg: falls with eyes closed (proprioception lost)
Charcot joints: painless joint destruction from repeated unrecognized trauma (proprioception gone, so patient doesn't know to protect the joint). Knee most common.
Key distinction from SCD: Tabes = posterior columns ONLY. No hyperreflexia, no Babinski, no UMN. SCD = posterior + lateral (both).
SCD = "Subacute COMBINED" because it hits TWO column systems (posterior + lateral). Tabes hits ONE (posterior). B12 causes combined. Syphilis causes isolated posterior.
4 / 8
Section 5 of 8
Elimination Game
Use the clues to knock out wrong answers one by one. Find the lesion.
Clinical Vignette
A 35-year-old woman wakes up with weakness in her right hand and arm with right-sided
hyperreflexia, difficulty writing, and poor vibration sense in the right thumb and index finger. She also reports she cannot feel hot and cold on her
LEFT arm and upper trunk, beginning below the right-sided lesion level, for the past week.
She has a history of optic neuritis 2 years ago.
ABrown-Sequard (C5-C6 right)
BCentral cord syndrome
CAnterior cord syndrome
DComplete cord transection
The loss is side-split, not bilateral: right motor plus right dorsal column signs, with left pain and temperature loss. This eliminates:
Anterior cord syndrome (would produce bilateral motor plus bilateral pain/temp loss with dorsal columns spared).
Complete transection (all modalities would be gone bilaterally). Both eliminated.
Weakness and hyperreflexia are IPSILATERAL (right). Pain and temperature loss is
CONTRALATERAL (left). The pattern is hemicord: one side carries ipsilateral CST and dorsal
columns; contralateral spinothalamic is affected. This is the textbook Brown-Sequard picture.
Eliminates Central cord (bilateral arm > leg, not a side-split pattern).
History of optic neuritis 2 years ago. MRI shows a
demyelinating plaque at C5 on the right side. No trauma. The cause is
Multiple Sclerosis, producing a Brown-Sequard pattern from a right-sided
demyelinating lesion at C5. MS is the second most common cause of Brown-Sequard (after penetrating trauma).
Diagnosis Confirmed
Brown-Sequard syndrome from MS at C5 right. Right CST gives ipsilateral weakness. Right dorsal columns give ipsilateral proprioception and vibration loss. Left pain and temperature are lost because those spinothalamic fibers crossed in the cord and ascended on the right. Optic neuritis plus a focal cord plaque = MS producing a Brown-Sequard pattern.
5 / 8
Section 6 of 8
Cheat Sheet
Every syndrome, every tract, side by side. Use this to drill the pattern until it's automatic.
Syndrome
Motor
Pain / Temp
Proprioception
Cause
Brown-Sequard
Ipsilateral loss
Contralateral loss
Ipsilateral loss
Penetrating trauma, MS
Central Cord
Bilateral (arms > legs)
Bilateral cape loss
Variable
Elderly hyperextension injury
Anterior Cord
Bilateral loss
Bilateral loss
PRESERVED
Anterior spinal artery infarct
Posterior Cord
Normal
Normal
Bilateral loss
B12 deficiency, syphilis
Syringomyelia
Arms at level (LMN)
Bilateral cape loss
Preserved early
Chiari malformation, trauma
ALS
UMN + LMN combined
NONE
NONE
TDP-43, SOD1 mutation
Polio
LMN flaccid weakness
None
None
Anterior horn infection
Infantile SMA
LMN floppy baby
None
None
SMN1 deletion, tongue fasciculations
MS Cord Plaque
Variable, asymmetric
Variable
Variable
Relapsing CNS demyelination
Cauda Equina
Asymmetric LMN root signs
Saddle, radicular pain
Root pattern
Disk, tumor, compression below conus
Conus Medullaris
Bilateral, symmetric
Perianal anesthesia
Variable
Sudden cord-end lesion at L1-L2
Complete SCI
Bilateral loss
Bilateral loss
Bilateral loss
Major trauma
UMN + LMN + NO SENSORY. This combination is pathognomonic for ALS. No other condition causes UMN hyperreflexia in the same limb as LMN atrophy and fasciculations without any sensory deficits.
The anterior spinal artery originates from the aorta. Cross-clamping the aorta during aneurysm repair can infarct the anterior cord. Patient wakes up paraplegic but can feel vibration and joint position. Preserved proprioception with lost motor and pain/temp = anterior cord, every time.
Polio, SMA, and ALS can all hit anterior horn cells. The deciding move is the company they keep: polio and SMA are LMN with sensory spared; ALS combines UMN plus LMN with sensory spared; B12 adds sensory loss, so it is not ALS.
6 / 8
Section 7 of 8
Quiz
Eleven original clinical questions. No shortcuts.
Question 1 / 11
A 42-year-old construction worker falls from scaffolding and sustains a stab wound to the
left side of his cervical spine at C6. In the ER: left-sided weakness (3/5), left-sided loss of vibration and
proprioception below C6, right-sided loss of pain and temperature below C7. DTRs are 3+ on the left,
normal on the right.
Which spinal cord syndrome does this represent?
Question 2 / 11
A 72-year-old woman is brought to the ED after a rear-end collision. Both arms have 2/5 grip
strength bilaterally, but she can walk with minimal assistance (4/5 leg strength). She has urinary retention.
Cervical spine X-ray shows diffuse degenerative changes, no fracture. MRI shows central cord signal change
at C4-C5.
What is the mechanism of her deficits?
Question 3 / 11
A 58-year-old man with hypertension undergoes repair of a descending thoracic aortic aneurysm.
Six hours postoperatively he cannot move his legs and has no pinprick or temperature sensation in his lower
extremities. However, he correctly identifies vibration and position changes when tested with a tuning fork.
Which spinal artery territory explains this presentation?
Question 4 / 11
A 45-year-old vegan man presents with 4 months of progressive difficulty walking, stumbling in
the dark, and positive Romberg. Exam: 3/5 leg strength, 4+ DTRs at patella and Achilles, bilateral Babinski,
AND absent ankle jerks. Vibration is absent to mid-shin bilaterally. Pinprick is intact.
Which best describes the coexisting neurological findings in this condition?
Question 5 / 11
A 55-year-old man presents to the ER with sudden-onset paralysis of both legs immediately after a motor vehicle collision. He cannot move or feel anything below the umbilicus. His blood pressure is 80/50 mmHg and heart rate is 52 bpm. A Foley catheter drains 800 mL of urine. Rectal tone is absent. He has no spasticity; his legs are completely flaccid with no reflexes.
Which phase of spinal cord injury does this presentation represent, and what neurological pattern is expected weeks later?
Question 6 / 11
A 48-year-old man presents with 8 months of progressive bilateral numbness in both hands in a cape-like distribution across his shoulders and upper arms, along with weakness of the intrinsic hand muscles. He reports burning pain in this same distribution. Leg strength and bladder function are intact. Vibration sense is preserved at the wrists. MRI shows a fluid-filled cystic cavity within the spinal cord at C4-C7.
Which feature of this presentation most reliably distinguishes syringomyelia from anterior cord syndrome?
Question 7 / 11
A 63-year-old woman with a history of pernicious anemia presents with progressive difficulty walking for 6 months. She sways when standing with her eyes closed and has fallen twice. Neurological exam: vibration absent at the ankles bilaterally; proprioception absent at the great toes; 4+ knee jerks bilaterally with bilateral Babinski signs; absent ankle jerks bilaterally. Pinprick sensation is intact in the feet.
The coexistence of absent ankle jerks alongside brisk knee jerks and Babinski signs in this patient is best explained by which combination of pathology?
Question 8 / 11
A 73-year-old man with a 30-year history of neck pain undergoes elective cervical decompression surgery. The morning after surgery he complains that he cannot feel heat or cold on either side of his chest and upper abdomen. His grip strength is 2/5 bilaterally but he can flex and extend his toes. DTRs are absent in both arms but 3+ at the knees. He has urinary retention.
Which spinal cord syndrome is most consistent with this post-operative presentation?
Question 9 / 11
A 67-year-old woman with a known thoracoabdominal aortic aneurysm undergoes endovascular repair. Several hours later in recovery she cannot move either leg and reports she cannot feel pinprick or temperature anywhere below the umbilicus. She CAN, however, accurately identify when her great toes are passively flexed or extended and feels a tuning fork on her shins. Her blood pressure is 92/58 mmHg.
Which vascular event best explains this constellation of deficits?
Question 10 / 11
An 82-year-old man with longstanding cervical spondylosis trips on a rug and lands face-first on the bathroom floor, momentarily hyperextending his neck. He is brought to the ED with 2/5 grip strength bilaterally, sensory loss in a shawl-like pattern over both shoulders and upper arms, but 4+/5 leg strength and a normal gait when assisted. He has urinary retention. Cervical CT shows no fracture; MRI shows central T2 hyperintensity at C4-C5 with no anterior or posterior column edema.
Which mechanism most directly accounts for the hand and arm weakness being more severe than the leg weakness?
Question 11 / 11
A 26-year-old man is brought to the ED after being stabbed in the right side of the lower neck during an altercation. He has 2/5 strength in the right leg with hyperreflexic right knee and ankle jerks, absent vibration and joint position sense in the right leg, and complete loss of pinprick and temperature sensation on the left side of his trunk and left leg starting two dermatomes below the wound. Right leg pinprick and temperature are intact. Left leg vibration and proprioception are intact.
Which spinal cord syndrome and most common cause does this presentation match?
7 / 8
BONE WIZARDRY · NEUROLOGY · SPINAL CORD SYNDROMES
clinical Walkthrough
clinical Walkthrough
Original clinical vignettes. Shuffled, never-repeat, full explanations for every choice.
8 / 8
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 12, 2026 at 11:55 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.