Plasma cell dyscrasia from benign paraprotein to end-organ disaster
A 68-year-old man presents with back pain for 3 months, fatigue, and new confusion. Labs: Ca 12.4, Creatinine 2.8, Hgb 9.2, total protein elevated with M-spike on SPEP. X-ray shows multiple lytic "punched-out" lesions in the skull and vertebrae. Bone marrow biopsy shows 35% plasma cells.
End-organ damage from malignant plasma cells. One letter at a time.
Same biology, different threshold. Diagnosis lives in the numbers and organ damage.
| Condition | Plasma Cells | M-Protein | End-Organ Damage | Progression Risk |
|---|---|---|---|---|
| MGUS | <10% | <3 g/dL, no Bence-Jones | None | ~1%/year to myeloma |
| Smoldering Myeloma | 10-60% | ≥3 g/dL | None (by definition) | ~10%/year (initial years) |
| Multiple Myeloma | >10% plus CRAB | Any | Yes (CRAB criteria) | Active disease |
| Plasma Cell Leukemia | >20% in blood | Variable | Severe, multi-organ | Very poor prognosis |

Three classic complications that extend beyond the four CRAB letters.
Four diagnoses. Two clues. One survives.
Four clinical questions. Original vignettes. Pick your answer before reading the explanation.
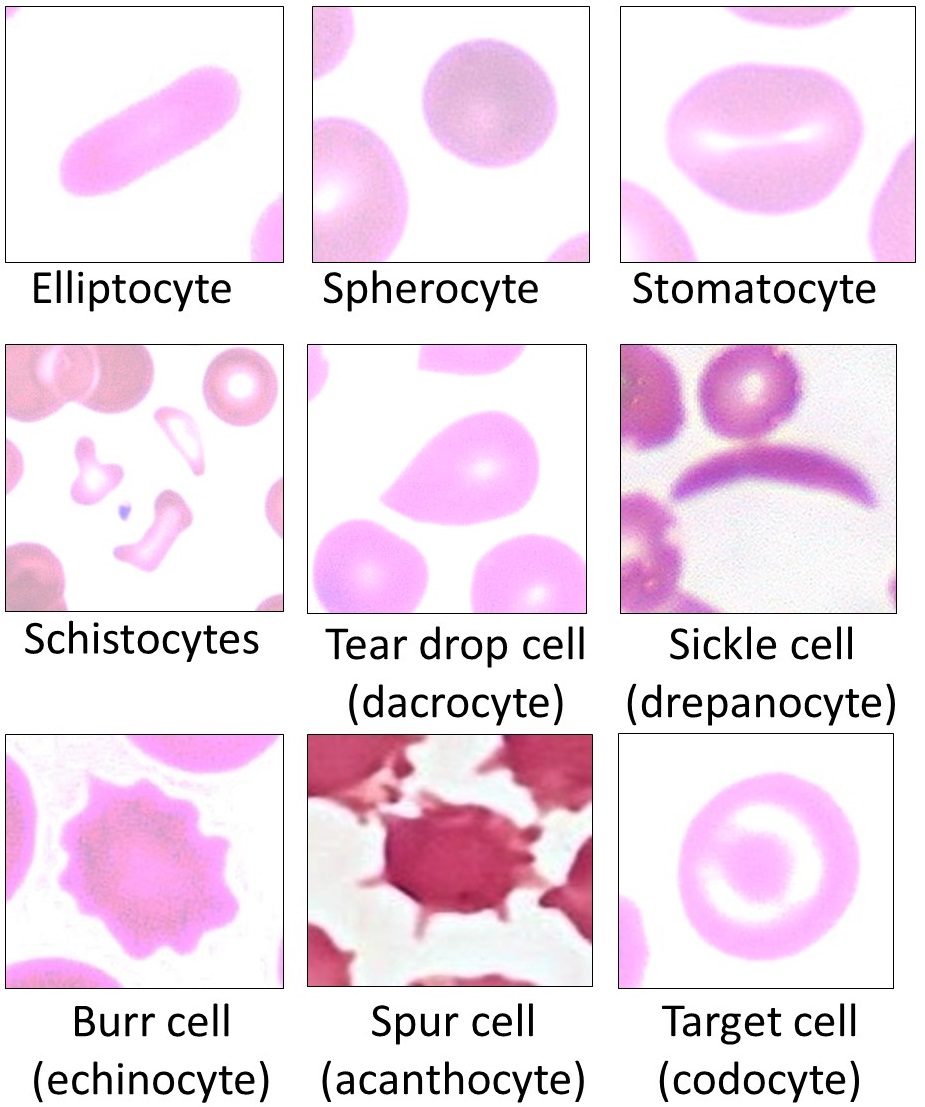
A 72-year-old woman with recently diagnosed multiple myeloma has a peripheral blood smear reviewed. The red blood cells appear stacked in linear arrangements, resembling coins in a stack.
What protein abnormality in her serum is directly responsible for this morphologic finding?A 66-year-old man with multiple myeloma and a creatinine of 3.1 mg/dL is scheduled for CT imaging of the chest, abdomen, and pelvis for staging purposes.
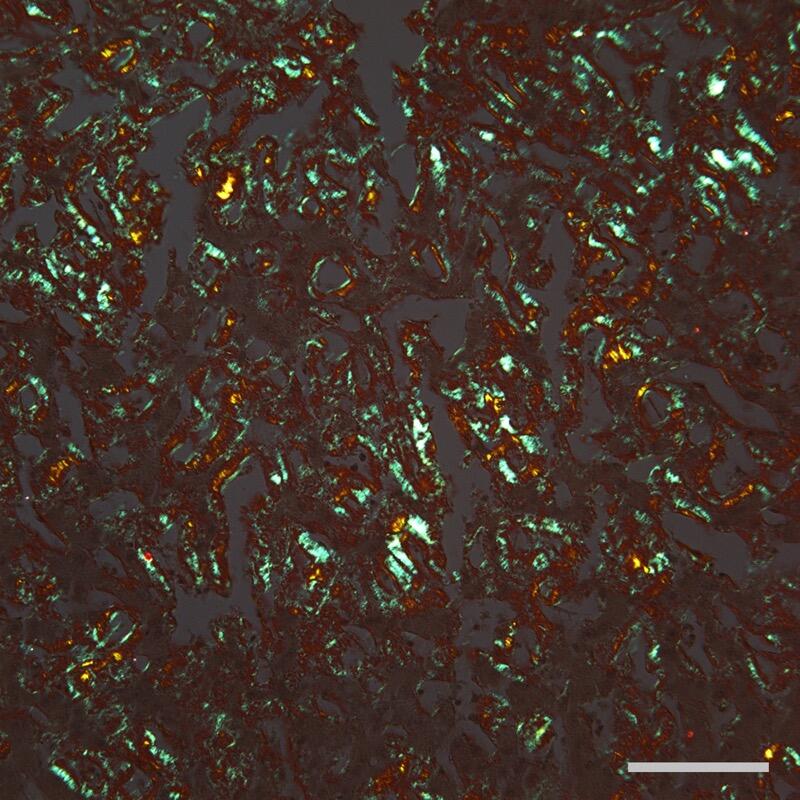
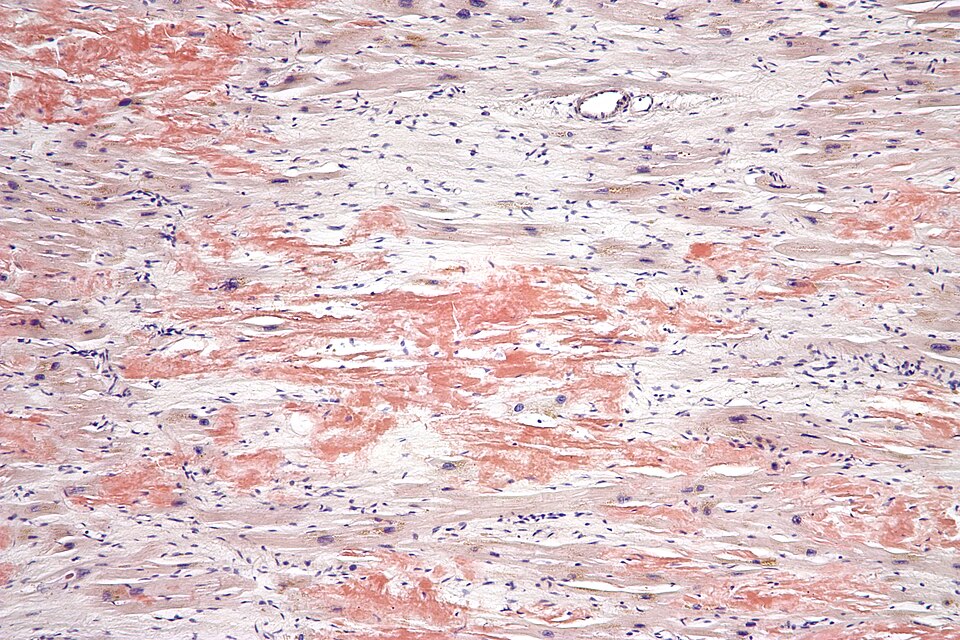
Why should iodinated IV contrast be avoided in this patient?A 61-year-old man with known AL amyloidosis develops progressive exertional dyspnea and lower extremity edema. Echocardiogram shows thickened left ventricular walls with a "granular sparkling" appearance and impaired relaxation. His ejection fraction is preserved at 55%.
What finding on his 12-lead EKG would be characteristic despite the thickened ventricle walls?A 58-year-old woman is found to have an M-spike on SPEP obtained during workup for fatigue. SPEP shows M-protein of 2.1 g/dL. Bone marrow biopsy shows 8% plasma cells. She has normal calcium, creatinine, hemoglobin, and no bone lesions on imaging. Her only complaint is mild fatigue, which workup attributes to iron deficiency rather than marrow infiltration.
Which single criterion most definitively distinguishes her diagnosis from multiple myeloma?Original clinical vignettes. Shuffled, never-repeat, full explanations for every choice.