Macrocytic, Normocytic & PNH
Random iron panel pops up. Read the four arrows. Pick the anemia. The pattern is the test · memorize the table once and you own the bench question.
Read the scenario, classify by MCV, then click to drill down to the diagnosis.
Defective nuclear division
Normal RBC size, not enough of them
Iron issues or thalassemia
MCV is the first triage gate on every anemia stem. <80 = microcytic → iron deficiency, thalassemia, anemia of chronic disease (late), lead, sideroblastic. 80·100 = normocytic → ask: hemolysis (retics up) or underproduction (retics down, BM, kidney, ACD)? >100 = macrocytic → ask: megaloblastic (B12, folate, drugs) or non-megaloblastic (liver, alcohol, hypothyroid, MDS, reticulocytosis)? The single number splits the entire workup tree · never start anemia from "what's the Hgb"; start from MCV + retics.



Tap each card to reveal the crime file (key labs and clinical features).
Follow the algorithm to reach the diagnosis.
Defective nuclear division slows down, RBCs become bigger
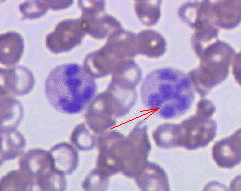
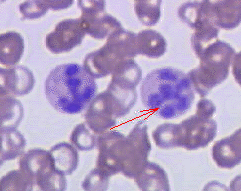
Macrocytic splits cleanly: megaloblastic (B12 or folate) vs non-megaloblastic. The smear tells you: hypersegmented neutrophils (>5 lobes) = megaloblastic. B12 vs folate · both give pancytopenia and macrocytosis, but only B12 deficiency causes subacute combined degeneration (posterior columns + corticospinal tracts → loss of vibration/proprioception + UMN signs). Folate gives no neuro findings. Pregnancy + macrocytic + no neuro = folate. Vegan or pernicious anemia + numb feet = B12. Give folate alone to a B12-deficient patient and you'll fix the anemia but accelerate the neuro damage.
| Feature | Vitamin B12 Deficiency | Folate Deficiency |
|---|---|---|
| Anemia Type | Megaloblastic | Megaloblastic |
| Neurologic Symptoms | YES - Subacute Combined Degeneration | NO - Never |
| Paresthesias | Dorsal columns affected | Not present |
| Elevated Homocysteine | YES | YES |
| Elevated Methylmalonate | YES (B12-specific) | NO |
| Most Common Cause | Type A Gastritis (Pernicious) | Overcooked vegetables |
Cofactors B12 Regulates:
Elevated methylmalonate is pathognomonic for B12 deficiency (not seen in folate deficiency)
Folate is the first vitamin to become depleted during periods of rapid cellular division because the body has minimal stores. Unlike B12 (which can be stored for years), folate reserves last only months.
Folate deficiency causes anemia only. Never causes neurologic symptoms (no myelin damage).
Thyroid hormones are permissive for all body functions. Without them, everything slows down → including bone marrow. RBCs grow large but slowly.
Denatures all proteins. Impairs nuclear division directly. Also commonly causes folate deficiency (poor diet + malabsorption).
Drugs damage DNA and stop nuclear replication. Cytoplasm keeps growing → macrocytic cells.
All anticonvulsants that cause macrocytic anemia block calcium and/or folate metabolism. Calcium is needed for microtubules during cell division.
Normal MCV, Normal MCH → nothing wrong with the RBC itself, just not enough of them
Normocytic forks on reticulocyte count. Retics up (>2% corrected) = bone marrow is responding · you're losing or destroying RBCs (hemorrhage, hemolysis). Then ask: extravascular (spleen) vs intravascular (haptoglobin down, LDH up, hemoglobinuria). Retics down or inappropriately normal = marrow can't keep up · think kidney (low EPO), chronic disease, marrow failure (aplastic, MDS, infiltration), early iron deficiency. "Normocytic + retics 4% + indirect bili up + LDH 800 + haptoglobin undetectable" is intravascular hemolysis until proven otherwise. The retic count is the second triage gate after MCV.
When a patient bleeds out suddenly, the body loses RBCs faster than it can replace them. Reticulocytes (immature RBCs) don't show up until day 3-4. Before that: normal RBC size, low count.
Infections, cancer, rheumatologic diseases trigger mild anemia by damping down erythropoietin (EPO). Before iron stores fully deplete (which takes months), the anemia is normocytic.
Kidneys make erythropoietin (EPO). No kidneys = no EPO = bone marrow doesn't make RBCs.
Thyroid hormones are required for EPO to work. Even if kidneys make EPO, without T3/T4 it's useless.
Most Common Cause: Idiopathic (Autoimmune T-Cell Mediated)
In most cases, autoreactive T-cells attack and destroy hematopoietic stem cells. Marrow becomes replaced with fat and cannot make any blood cells (pancytopenia). Parvovirus B19 causes aplastic crisis in patients with chronic hemolysis (e.g., sickle cell), and pure red cell aplasia in immunocompromised patients, but it is NOT the most common cause of acquired aplastic anemia.
Other Causes:
Cancer of the bone marrow. Marrow becomes fibrotic (scarred, rigid) instead of making blood. RBCs can't be produced.
Genetic aplastic anemia (autosomal recessive DNA repair defect). ALL cell lines fail (pancytopenia, not just RBCs). Associated with physical anomalies including absent or hypoplastic thumbs and radius abnormalities. Increased cancer risk. Do NOT confuse with Diamond-Blackfan (pure RBC aplasia).
RBC aplasia + finger abnormality (classically triphalangeal thumb → thumb with 3 bones instead of 2).
Rare, acquired, life-threatening hemolytic anemia
Watch how the GPI anchor (yellow) protects RBCs from complement attack.
Hemolysis is chronic but episodic. Patients are constantly exhausted because they're losing RBCs constantly.
Hemolysis releases bilirubin. Yellowing of skin and sclera.
Hemoglobin gets filtered into urine. Concentrated in the morning (hence "nocturnal"). Not always at night → can happen anytime, despite the name.
PNH has a weird tendency to cause clots in abnormal places:
RBCs placed in a petri dish + complement + acid (decreased pH) → RBCs lyse (hemoglobinuria visible). Positive = PNH. But outdated.
Detects absence of CD55 and CD59 on RBC surface. Much more sensitive and specific.
Block the C5 protein of the complement system to prevent RBC destruction.
C5 Blockers (complement inhibitors):
Start with MCV. Click each branch to follow the workup algorithm.
25 clinical vignettes covering macrocytic, normocytic, hemolytic, and PNH. Shuffled each session.