The question isn't "what type of anemia?" -- it's "WHY is this person iron deficient?" Demographics decide the workup. Get the demographic, get the answer.
Before you learn anything, take the shot:
A 57-year-old postmenopausal woman presents with fatigue and pallor. Labs: hemoglobin 8.2 g/dL, MCV 68 fL, serum iron low, TIBC elevated, ferritin 8 ng/mL. Peripheral smear shows microcytic hypochromic red cells with pencil cells. Which finding would you MOST expect on further workup?
Decreased haptoglobin
Positive stool guaiac
Elevated reticulocyte count
Positive direct Coombs test
Elevated LDH with schistocytes
That's it. In a postmenopausal woman (or any adult male) with iron deficiency anemia, the cause is GI bleeding until proven otherwise. She can't blame menstruation anymore. Positive stool guaiac confirms occult GI blood loss. Next step is colonoscopy to rule out colon cancer. Demographics drive the workup, always.
Decreased haptoglobin means hemolysis -- the haptoglobin gets consumed binding free hemoglobin released from lysed red cells. But look at the smear: microcytic hypochromic + pencil cells. That's IDA, not hemolysis. Low haptoglobin = hemolysis. High TIBC + low ferritin + pencil cells = IDA.
Elevated reticulocyte count means the marrow is cranking out new cells -- that's hemolytic anemia or acute blood loss. In IDA, the marrow WANTS to make cells but CAN'T because there's no iron. Low reticulocytes = production problem (IDA). High reticulocytes = destruction problem (hemolysis).
Positive direct Coombs test means antibodies are stuck to red blood cells -- autoimmune hemolytic anemia. But this patient has microcytic hypochromic cells with pencil cells and a ferritin of 8. Autoimmune hemolysis causes normocytic anemia, not microcytic. Direct Coombs+ = autoimmune hemolysis. Ferritin 8 + microcytic = IDA.
Elevated LDH with schistocytes = intravascular hemolysis (TTP, HUS, DIC). Schistocytes are red cell fragments from physical shearing. This patient's smear shows pencil cells -- not schistocytes. Schistocytes + high LDH = microangiopathic hemolysis. Pencil cells + low ferritin = IDA.
THE PATTERN
Demographics Decide Everything
The labs confirm IDA. The demographic tells you WHY.
The One Rule That Runs the Whole Topic
Once you confirm IDA (low ferritin, low iron, high TIBC, microcytic hypochromic), the next question is always: "Why is this person losing iron?"
The answer depends entirely on who the patient is:
Postmenopausal woman or adult male → GI bleeding → colon cancer until proven otherwise
Postmenopausal woman + IDA = colon cancer workup. Highest-yield association in clinical practice. She can't lose iron through menstruation anymore. If she's iron deficient, she's bleeding somewhere you can't see, and the GI tract is suspect #1. Stool guaiac → colonoscopy.
🔑IDA cause by who: Post-meno = Poop (GI bleed). Pre-meno = Period. Kid = Kow milk. Pregnant = Picking for two.
THE SUSPECTS
IDA Lab Panel
Each test tells part of the story. Tap a card to see what it means and when it lies.
1
Serum Ferritin
tap to flip →
Storage Iron
Ferritin = stored iron. Most specific test for IDA. Low ferritin basically confirms it. Caveat: ferritin is an acute phase reactant -- inflammation, infection, and malignancy can raise it falsely. A "normal" ferritin in an inflamed patient might be hiding true IDA. When in doubt, check soluble transferrin receptor (sTfR).
2
Serum Iron
tap to flip →
Iron in Transit
Low in BOTH IDA and anemia of chronic disease (ACD). Not specific enough alone to separate them. Always pair with TIBC and ferritin. Low serum iron + low ferritin + high TIBC = IDA. Low serum iron + high ferritin + low TIBC = ACD.
3
TIBC
tap to flip →
The Hunger Signal
Total Iron Binding Capacity = how many transferrin trucks are available. HIGH in IDA (body sends more trucks to find iron). LOW in ACD (body isn't hunting -- iron is just locked away). HIGH TIBC is the ONE value that goes UP in IDA while everything else drops.
4
Transferrin Sat
tap to flip →
Cargo-to-Truck Ratio
Transferrin saturation = serum iron / TIBC. In IDA: low iron / high TIBC = very small fraction. Less than 15% essentially confirms IDA. Lots of trucks (high TIBC) with almost no cargo (low iron) -- saturation crashes. Normal is 20-50%.
5
Soluble TfR
tap to flip →
Inflammation-Proof
Soluble transferrin receptor (sTfR) is elevated in true IDA even when inflammation is present. Unlike ferritin, it does NOT rise with acute-phase reactions. When a patient has RA AND iron deficiency, ferritin might look falsely normal. Elevated sTfR unmasks the true IDA hiding behind ACD.
6
Bone Marrow Bx
tap to flip →
Gold Standard
Bone marrow biopsy with Prussian blue iron stain = gold standard for iron stores. Absent stainable iron = confirmed IDA. You rarely need this -- low ferritin is usually enough. But in complex cases (concurrent inflammation, overlap of IDA + ACD, unexplained microcytic anemia), the bone marrow settles the debate definitively.
CLINICAL IMAGES
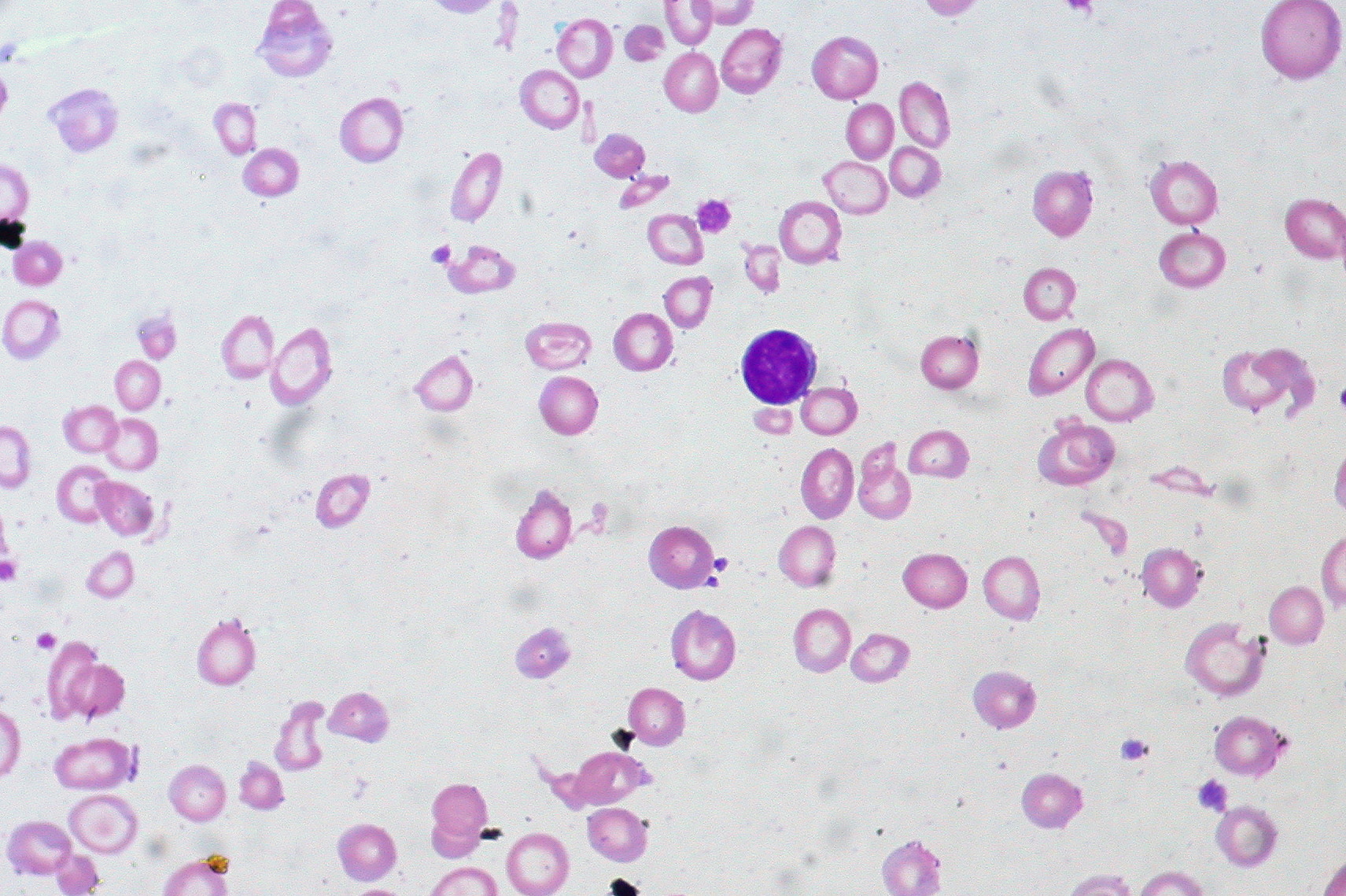
📷 IDA Peripheral Smear · tap to expand
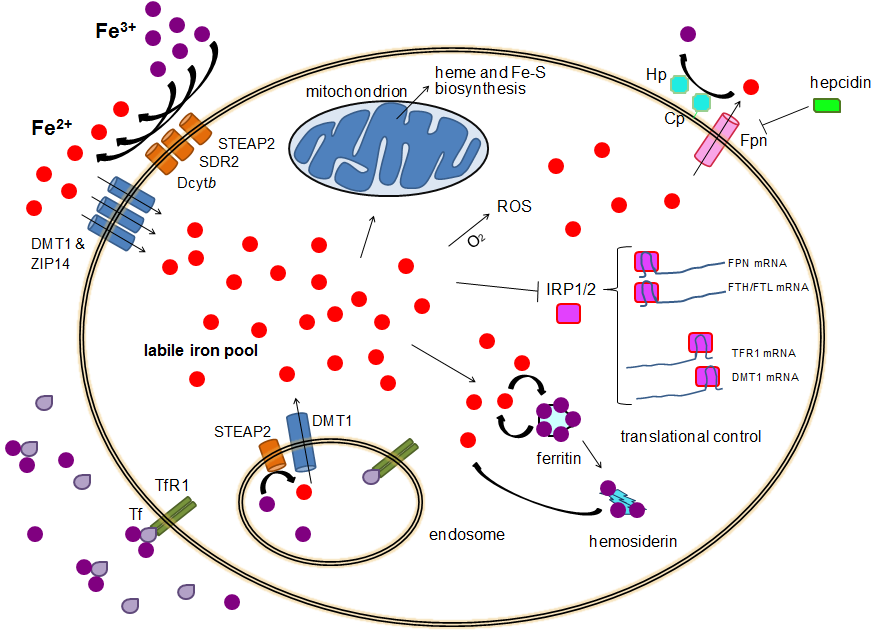
📷 Iron Homeostasis · tap to expand
LAB VALUE MAP
Microcytic Anemia: The Four-Way Comparison
Same MCV. Different iron stories. Bar height encodes the lab value: short = LOW, medium = NORMAL, tall = HIGH.
Reading the map: IDA is the only column with LOW Fe + HIGH TIBC + LOW ferritin. ACD mirrors IDA on serum Fe but flips TIBC and ferritin (locked iron). Thalassemia keeps iron normal/high (genetic globin problem, not iron). Sideroblastic loads iron everywhere except into hemoglobin.
DEMOGRAPHIC ALGORITHM
Confirmed IDA → Demographic Branch Point
Once iron studies confirm IDA, the patient's age and sex dictate the workup. Same labs, four different next steps.
INTERACTIVE WORKUP
IDA Diagnosis Decision Tree
Microcytic anemia confirmed. Walk the labs to the diagnosis. Tap each choice to advance.
Step 1: Patient has MCV 68, hemoglobin 9.0 g/dL. First test to order?
Serum ferritin + iron + TIBC panel
Bone marrow biopsy right now
Hemoglobin electrophoresis
Correct. Start with the iron panel. Ferritin + serum iron + TIBC gives you the complete iron picture in one draw. Bone marrow is the gold standard but is invasive -- save it for when the panel is inconclusive. Electrophoresis is for thalassemia, but you don't know that yet.
Not the move. Bone marrow biopsy is invasive and overkill as a first step. Start with the non-invasive iron panel. Biopsy is reserved for cases where serum studies are ambiguous or contradictory.
Not yet. Hemoglobin electrophoresis diagnoses thalassemia, but you haven't ruled in IDA yet. The iron panel comes first. If the iron panel is normal (ferritin normal, TIBC normal), THEN you suspect thalassemia and run the electrophoresis.
Step 2: Ferritin 6 ng/mL, serum iron low, TIBC 420 ug/dL (elevated). IDA confirmed. Patient is a 62-year-old man. What's the workup?
Colonoscopy to rule out GI malignancy
Start oral iron, reassess in 3 months
Dietary counseling for iron-rich foods
Right. Adult male with IDA = GI bleeding until proven otherwise = colonoscopy. You're hunting for colon cancer. IDA is often the FIRST sign -- the tumor bleeds slowly into the GI tract, just enough to drain iron stores over months. Finding it early saves his life. Treat the iron too, but colonoscopy is the priority.
Missing the bigger picture. Yes, he needs iron -- but the IDA is the alarm, not the disease. A 62-year-old man can't blame poor diet or menstruation. Something is bleeding. Starting iron without finding the source is like silencing a fire alarm while the building burns. Colonoscopy first.
Wrong demographic reasoning. Dietary IDA is for toddlers drinking too much cow's milk. In a 62-year-old man, IDA means GI blood loss. Dietary changes won't fix a bleeding colon tumor. This is colonoscopy territory.
Step 3: Colonoscopy negative. Upper endoscopy negative. Patient still has IDA. What next?
Capsule endoscopy (small bowel evaluation)
Check tTG antibodies for celiac disease
Both -- capsule endoscopy AND tTG antibodies
Full workup is right. When both scopes are negative, the small bowel becomes suspect. Capsule endoscopy catches small bowel lesions. AND celiac destroys duodenal villi -- the exact place iron is absorbed. Celiac causes IDA through malabsorption, not bleeding. Check both simultaneously. tTG positive + villous atrophy on biopsy = celiac as the culprit.
Partially right. Capsule endoscopy for the small bowel is correct. But don't forget celiac -- it causes IDA through iron malabsorption in the duodenum. tTG antibodies are cheap and fast. Check both rather than working sequentially.
Good instinct but incomplete. tTG for celiac is correct -- common cause of IDA through iron malabsorption in the duodenum. But also evaluate the small bowel for other lesions via capsule endoscopy. Both together give the complete picture after negative upper and lower scopes.
Step 4: RA patient. Ferritin 180 ng/mL. Serum iron LOW, TIBC LOW, MCV 74. This is NOT IDA -- what is it?
Anemia of Chronic Disease (ACD)
Still IDA -- ferritin elevated by inflammation
Beta-thalassemia trait
Correct. ACD: IL-6 from RA drives hepcidin production. Hepcidin locks iron in macrophages and blocks duodenal absorption. Iron is TRAPPED, not absent. Ferritin is high (stores are full but locked). TIBC is low (body isn't hunting for iron -- it's sequestered). IDA = low ferritin + high TIBC. ACD = high ferritin + low TIBC.
Tempting but wrong. Yes, ferritin can be elevated by inflammation. But TIBC is also LOW here. In true IDA, the body makes MORE transferrin (high TIBC) to hunt for iron. In ACD, the body doesn't need to hunt -- the iron is there, just locked. Low TIBC + high ferritin + inflamed patient = ACD, not IDA.
Wrong track. Thalassemia trait has NORMAL iron studies -- ferritin normal, TIBC normal, serum iron normal. This patient has abnormal iron distribution (high ferritin, low serum iron, low TIBC) in the context of chronic inflammation. That's ACD.
IRON LOGIC
IDA Lab Pattern
Every lab value in IDA follows a single logic chain.
The Cause-Effect Chain
Iron stores depleted → body can't make hemoglobin properly → every lab reflects this:
Ferritin LOW -- ferritin = stored iron. Empty stores = low ferritin. Most specific test for IDA.
Serum iron LOW -- no iron floating around in the blood🔑Serum iron = iron in the blood RIGHT NOW. Ferritin = stored iron. Both low in IDA. Serum iron is also low in ACD -- so ferritin and TIBC are what separate them.
TIBC HIGH -- body makes MORE transferrin trying to grab any iron it can find. More trucks, no cargo.🔑TIBC high = body is Trying Incredibly hard to Bind iron it Can't find. Only goes UP in IDA. Goes DOWN in ACD.
Transferrin saturation LOW -- lots of trucks (high TIBC) but almost no cargo (low iron). Sat = iron/TIBC. Less than 15% = IDA.
Ferritin is the MOST SPECIFIC test for IDA. Low ferritin basically confirms IDA. The only caveat: ferritin is an acute phase reactant -- in inflammation, infection, or malignancy, ferritin can be falsely elevated. A "normal" ferritin might actually be low for that patient. Use sTfR to unmask the truth in inflamed patients.
🔑RA + IDA patient. Ferritin is 95 -- looks normal. But inflammation drove it up from 8. sTfR will be elevated (not affected by inflammation) -- that's the tell.
The Peripheral Smear
Three findings on the smear that scream IDA:
Microcytic hypochromic RBCs -- small, pale cells (not enough hemoglobin to fill them)
Pencil cells (elliptocytes) -- elongated, cigar-shaped RBCs. Relatively specific for IDA.🔑Pencil cells = iron so low the RBC collapses into a pencil shape. Also called elliptocytes. IDA-specific. NOT seen in thalassemia or ACD.
What you will NOT see: schistocytes (hemolysis), spherocytes (hereditary spherocytosis / autoimmune), bite cells (G6PD). If any appear, you're not dealing with IDA.
Feature
IDA
ACD
Thalassemia
Ferritin
LOW
Normal/HIGH
Normal
TIBC
HIGH
LOW
Normal
Serum iron
Low
Low
Normal
Smear
Pencil cells, targets
Normocytic usually
Targets, microcytes
Electrophoresis
Normal
Normal
Elevated HbA2
🔑IDA labs: everything goes DOWN except TIBC. TIBC goes UP because the body is Trying Incredibly hard to Bind iron it Can't find.
THE STAKES
IDA vs Hemolysis: The Board Trap
They LOVE mixing these up. Here's how to separate them instantly.
Feature
Iron Deficiency
Hemolytic Anemia
MCV
Low (microcytic)
Normal or high
Reticulocytes
Low (can't make cells)
HIGH (marrow compensating)
Haptoglobin
Normal
LOW (consumed binding free Hgb)
LDH
Normal
HIGH (released from lysed cells)
Indirect bili
Normal
HIGH (heme breakdown)
Ferritin
LOW
Normal or high
TIBC
HIGH
Normal
Smear
Pencil cells, targets
Schistocytes, spherocytes, bite cells
Board Trap: The question that tripped you. Postmenopausal woman with microcytic hypochromic anemia and pencil cells. They offer "decreased haptoglobin" as an answer. You pick it because you associate anemia with hemolysis. But low haptoglobin = hemolysis, NOT iron deficiency. In IDA, haptoglobin is NORMAL -- red cells aren't being destroyed, they're just poorly made. Pencil cells = IDA. Schistocytes = hemolysis. No overlap.
Board Trap: Normal ferritin rules out IDA. Wrong. Ferritin is an acute phase reactant. In a patient with RA or cancer, ferritin is elevated by inflammation. A ferritin of 95 in a patient with RA might represent true IDA masked by the acute phase response. Check soluble transferrin receptor (sTfR) -- elevated in true IDA and NOT affected by inflammation.
The weird associations that show up once a year in clinical practice and everyone misses.
Plummer-Vinson Syndrome
The triad: IDA + esophageal webs + dysphagia
Iron deficiency causes mucosal atrophy → thin membranes (webs) form in the upper esophagus → food gets stuck. Classic board: middle-aged woman with IDA who can't swallow her steak.
The high-yield detail: Plummer-Vinson increases the risk of squamous cell carcinoma of the esophagus.
🔑Plummer-Vinson = PVS = Poor Vitamin (iron) Swallowing. IDA + can't swallow + esophageal web. Cancer risk = squamous, not adeno.
Pica: The Weird Cravings
IDA patients crave non-food items. If a question mentions a patient who chews ice all day and is anemic, it's IDA.
Pagophagia = craving ice. Most common form of pica in IDA.🔑Pago = frozen. Ice = pagophagia. Dirt = geophagia. Starch = amylophagia. All resolve when you treat the iron deficiency.
Geophagia = craving dirt/clay
Amylophagia = craving starch
Treatment: Oral Ferrous Sulfate
First-line: Oral ferrous sulfate. Take on an empty stomach with vitamin C (enhances absorption in the duodenum).
Earliest sign of response:Reticulocyte count rises in 5-7 days. Hemoglobin takes weeks. MCV normalizes over months. Reticulocytes are the canary.🔑Reticulocytes (5-7 days) = bone marrow saying "I finally have iron, let me crank." If they don't bump, patient isn't absorbing or taking the iron.
If oral iron fails: IV iron (ferric carboxymaltose, iron sucrose). Used in: malabsorption (celiac, IBD, post-gastric bypass), pregnancy with severe GI intolerance, dialysis patients.
DANGER ZONES
More Board Traps
The wrong answers that feel right, and how to kill them.
Trap: Elevated ferritin rules out IDA. Not always. Ferritin is an acute phase reactant. In a patient with concurrent inflammation (RA, infection, cancer), ferritin can be normal or elevated despite true iron deficiency. In these cases, use soluble transferrin receptor (sTfR) -- elevated in IDA and NOT affected by inflammation.
Trap: MCV 68 fL = thalassemia. Thalassemia and IDA both cause microcytic anemia. But thalassemia has NORMAL iron studies (ferritin normal, TIBC normal, serum iron normal). The Mentzer index (MCV/RBC count) can help: less than 13 suggests thalassemia, greater than 13 suggests IDA. Also, thalassemia has target cells WITHOUT pencil cells, and the RBC count is often HIGH.
Trap: Lead poisoning on the smear. Lead poisoning also causes microcytic anemia, but the smear shows basophilic stippling (tiny blue dots in the RBC). IDA doesn't do that. If they show you microcytic anemia with basophilic stippling, it's lead, not IDA.
🔑The Mentzer Index: MCV / RBC count. Less than 13 = thalassemia (lots of tiny cells). More than 13 = IDA (fewer, tinier cells). Not perfect, but a fast screen.
TEST YOURSELF
Quiz
10 questions, 5 shown at random. All original.
First prove iron deficiency with the iron panel, then ask why the stores got drained.
Age, sex, pregnancy, diet, inflammation, and absorption decide the next clinical step.
After you answer, the stem clues glow so the pattern is visible, not guessed.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 5, 2026 at 8:17 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.