PT vs PTT, the cascade, and every bleeding question clinical medicine will throw at you.
Quick · before we start
A 6-year-old boy has prolonged bleeding after a tooth extraction. His PT is normal but PTT is elevated. Mixing study corrects. What's the most likely diagnosis?
Hemophilia A
von Willebrand Disease
DIC
Factor V Leiden
Nice. Isolated PTT elevation + corrects on mixing = factor deficiency. Young boy + bleeding after procedure = X-linked hemophilia. vWD would also elevate PTT and correct on mixing, but the X-linked pattern (boy) and post-procedural bleeding (deep, not mucosal) points to hemophilia A. DIC would tank BOTH PT and PTT. Factor V Leiden causes clotting, not bleeding.
Not quite. Think about the clues: isolated PTT elevation (PT normal), corrects on mixing, young boy. That's a classic setup. Keep reading · you'll nail this by the end.
↓ scroll to begin
The Cascade: Intrinsic, Extrinsic, Common
Here's the thing about the coagulation cascade: clinical medicine doesn't care if you memorize every Roman numeral. They care if you can read a PT/PTT result and know which pathway is broken.
Three pathways. Two lab tests. That's the whole game.
INTRINSIC Measured by PTT
XII → XIIa
↓
XI → XIa
↓
IX → IXa
↓
VIII + IXa = TenaseThe tenase complex (VIIIa + IXa) activates Factor X. VIII is what's missing in Hemophilia A. Think: Eight = Ate = the one that gets consumed.
↓ to Common
EXTRINSIC Measured by PT/INR
Tissue damage releases TFTissue Factor (Factor III) · exposed when endothelium is damaged. This is why the extrinsic pathway is "extrinsic" · it needs something from OUTSIDE the blood (tissue factor from damaged cells).
↓
VII + TF = active complex
↓ to Common
Factor VII has the shortest half-life of all clotting factors. That's why PT rises first in liver disease and warfarin.
COMMON Affects BOTH PT & PTT
X → Xa
↓
Xa + V = ProthrombinaseThe prothrombinase complex (Xa + Va) converts prothrombin (II) to thrombin (IIa). Factor V is what Factor V Leiden makes resistant to degradation · hence hypercoagulable.
↓
II (Prothrombin) → IIa (Thrombin)
↓
I (Fibrinogen) → Ia (Fibrin)
↓
XIII cross-links fibrin
🔑PT = Path of Tissue factor (extrinsic). PTT has the extra T: more letters, more factors, longer pathway (intrinsic).📹Intrinsic pathway starts with XII (12). Count down: 12, 11, 9, 8. That's the order. Factor XII activates XI, XI activates IX, IX + VIII activate X.🎯Both pathways converge at factor X. Think of factor X as the drain everything flows into. Hemophilia blocks the left pipe (intrinsic). The right pipe (extrinsic) still drains. PT stays normal.
PT vs PTT: The Two Tests That Matter
PT / INR
Tests the extrinsic + common pathway
Factors: VII, X, V, II, I
Monitors warfarin therapy
Rises FIRST in liver disease (VII = shortest half-life)
Uses tissue thromboplastinThe PT test adds tissue factor + calcium to plasma and measures how fast it clots. Since tissue factor activates VII directly, it tests the extrinsic path. as reagent
PTT (aPTT)
Tests the intrinsic + common pathway
Factors: XII, XI, IX, VIII, X, V, II, I
Monitors heparin (unfractionated) therapy
More factors = more things that can go wrong
Uses phospholipid + activatorThe PTT test adds a contact activator (like kaolin or silica) + phospholipid + calcium. It bypasses tissue factor entirely, testing only the intrinsic path's ability to generate thrombin. as reagent
The pattern-reading cheat sheet: PT up alone = extrinsic (VII). PTT up alone = intrinsic (XII, XI, IX, VIII). Both up = common pathway (X, V, II, I) or DIC or severe liver disease.
Board Trap
Factor XII deficiency causes elevated PTT but NO bleeding risk. clinical medicine loves testing this. XII is needed for the lab test to work but isn't important for in-vivo clotting. A patient with prolonged PTT and no bleeding history? Think XII deficiency. Don't anticoagulate them.
The Mixing Study: Factor Deficiency vs Inhibitor
When PTT is elevated, the next question is always: why? The mixing study answers it.
Mix the patient's plasma 1:1 with normal plasma (which has all factors). Then re-run the PTT.
Patient plasma + Normal plasma (1:1 mix)
↓ re-run PTT
PTT corrects = Factor deficiency Normal plasma donated the missing factor
PTT doesn't correct = Inhibitor present Something in patient's plasma is blocking clotting
🔑Mixing study = asking "can normal plasma fix this?" If yes, patient was just missing something. If no, patient has something fighting the clotting (an inhibitor).🧡Lupus anticoagulant name is a triple lie: not always lupus, not a true anticoagulant (it clots in vivo), and not always associated with clinical lupus symptoms. It's an antiphospholipid antibody that causes THROMBOSIS.🛒Acquired factor VIII inhibitor vs lupus anticoagulant: both don't correct on mixing. The difference is clinical: bleeds = acquired VIII inhibitor. Clots + pregnancy loss = lupus anticoagulant (antiphospholipid syndrome).
The two big inhibitors clinical medicine tests:
Lupus anticoagulant · PTT up, but causes clotting in vivo (paradox!). Part of antiphospholipid syndromeAntiphospholipid syndrome: lupus anticoagulant, anti-cardiolipin, anti-beta-2-glycoprotein I antibodies. Causes arterial AND venous thrombosis, recurrent pregnancy loss. The "anticoagulant" name is misleading · it's only an anticoagulant in the test tube.
Factor VIII inhibitor · acquired antibody against factor VIII. Rare but classic board question: older adult with new-onset severe bleeding + elevated PTT + doesn't correct.
Board Trap
Lupus anticoagulant elevates PTT but causes thrombosis, not bleeding. The name is a lie. "Anti-coagulant" in the tube, pro-coagulant in the body. If a question gives you elevated PTT + recurrent DVTs or pregnancy loss, that's lupus anticoagulant · not a bleeding disorder.
The Big Bleeding Disorders
Tap any card to expand the details.
⚔️Deep bleeding (joints, muscles) = coagulation disorder (weak fibrin clot). Superficial bleeding (nosebleeds, gum, heavy periods) = platelet/vWF disorder (can't make the plug). Bleeding LOCATION tells you the MECHANISM.🌟TTP pentad: Thrombocytopenia, MAHA (schistocytes), Fever, Renal failure, Neuro changes. Normal PT/PTT. Emergency = plasma exchange. NEVER give platelets: it's adding fuel to the fire of microthrombi.📅HIT timeline: 5-14 days after starting heparin. Platelet count drops more than 50% from baseline. New clot forms despite low platelets. Stop ALL heparin (including flushes). Switch to argatroban or bivalirudin. Never switch to just LMWH: cross-reacts with the antibody.
Hemophilia A
Factor VIII deficiency. X-linked recessive.
Deep bleeding: joints (hemarthrosis), muscles, post-surgical
PTT ↑ | PT normal | Mixing: corrects | Bleeding time: normal
Most common severe inherited bleeding disorder. Almost exclusively males (X-linked). Severity depends on factor VIII level: <1% = severe (spontaneous joint bleeds), 1-5% = moderate, 5-40% = mild (bleed after surgery/trauma).
Treatment: Factor VIII concentrate (recombinant). Desmopressin (DDAVP) for mild hemophilia · it releases stored vWF and factor VIII from endothelial cells.
Complication: ~30% develop inhibitors (antibodies against infused factor VIII). Then mixing study won't correct anymore.
tap to expand
Hemophilia B (Christmas Disease)
Factor IX deficiency. X-linked recessive.
Clinically identical to Hemophilia A · distinguish by factor assays
PTT ↑ | PT normal | Mixing: corrects | Bleeding time: normal
5x less common than Hemophilia A but clinically indistinguishable. Named after Stephen Christmas, the first patient described. Same X-linked pattern, same joint/deep bleeding.
Treatment: Factor IX concentrate. DDAVP does NOT work for Hemophilia B · it only releases VIII and vWF, not IX.
Board clue: If they give you an X-linked bleeder with PTT elevation and say "DDAVP didn't help," they're telling you it's Hemophilia B, not A.
Mucosal bleeding: nosebleeds, heavy periods, GI bleeds, easy bruising
PTT ↑ or normal | PT normal | Mixing: corrects | Bleeding time ↑
Most common inherited bleeding disorder overall (1% of population). vWF does two jobs: (1) helps platelets stick to damaged vessels, (2) carries and stabilizes factor VIII in blood.
Types: Type 1 (partial quantitative, ~80% of cases, mild), Type 2 (qualitative, multiple subtypes), Type 3 (complete absence, severe, autosomal recessive).
Why PTT rises: Without vWF to stabilize it, factor VIII gets degraded faster → functional VIII drops → PTT goes up. But in mild vWD, factor VIII may be preserved enough that PTT stays normal.
Treatment: DDAVP (releases stored vWF from endothelial Weibel-Palade bodies). Avoid in Type 2B · releasing more defective vWF worsens platelet aggregation and causes thrombocytopenia.
tap to expand
DIC (Disseminated Intravascular Coagulation)
Systemic activation of coagulation → uses up everything.
Bleeding AND clotting simultaneously. Fibrin meshes shred RBCs = schistocytes
Not a disease · a complication. Something triggers massive coagulation: sepsis, trauma, obstetric complications (placental abruption, amniotic fluid embolism), malignancy (especially acute promyelocytic leukemiaAPL (M3 AML) releases tissue factor from leukemic granules, triggering DIC. This is why APL presents with severe bleeding. Treatment: all-trans retinoic acid (ATRA) differentiates the leukemic cells and stops the DIC trigger.).
The paradox: You clot so much that you run out of clotting factors AND platelets. Now you can't clot at all. Bleed and clot at the same time.
Lab pattern: Everything is consumed. PT up, PTT up, platelets down, fibrinogen down, D-dimer sky-high (fibrin is being made AND broken down). Schistocytes on smear (RBCs shredded by fibrin strands).
Treatment: Treat the cause. Support with FFP (factors), cryoprecipitate (fibrinogen), platelets.
tap to expand
HIT (Heparin-Induced Thrombocytopenia)
Antibodies against heparin-PF4 complex.
Platelets drop 5-14 days after heparin → paradoxical thrombosis
Platelets ↓ (>50% from baseline) | PT/PTT may be normal | Serotonin release assay confirms
Type II HIT is the dangerous one (immune-mediated). Type I is mild, non-immune, and doesn't matter for clinical practice.
Timeline: Typically 5-14 days after starting heparin. Can be sooner if prior heparin exposure. Platelets drop >50% from baseline (usually to 20-100K range).
The paradox: Low platelets but they CLOT. Activated platelets release procoagulant microparticles. Venous thrombosis is more common than arterial.
Management: STOP all heparin (including flushes). Start a direct thrombin inhibitorArgatroban (hepatic clearance) or bivalirudin. NOT LMWH · cross-reacts with the antibody. NOT warfarin alone · causes skin necrosis from protein C depletion. Start warfarin only after platelets recover.. Do NOT just switch to LMWH (cross-reacts). Do NOT give warfarin until platelets recover.
Key distinction from DIC: In TTP, the coagulation cascade is NOT activated. PT and PTT are NORMAL. The problem is platelet-mediated microthrombi, not fibrin.
Pathophysiology: ADAMTS13 normally cleaves ultra-large vWF multimers. Without it, giant vWF strings hang off endothelium and snag platelets → microthrombi in small vessels → end-organ damage.
Treatment:Plasma exchange (plasmapheresis) · removes the antibody, replaces ADAMTS13. This is the emergency. Do NOT give platelets · it's fuel on the fire (more platelets to clump).
vs HUS: HUS = similar picture but renal-dominant, often triggered by E. coli O157:H7 (Shiga toxin). Typical HUS = child with bloody diarrhea → renal failure + MAHA + thrombocytopenia. Atypical HUS = complement-mediated.
tap to expand
Tap Each Card to Flip
Front: the fast board facts. Back: the mechanism.
Intrinsic Pathway
💧
XII → XI → IX → VIII
Measured by PTT (aPTT)
TriggerContact with collagen / phospholipid
Lab testPTT elevated if broken
Key complexTenase (VIIIa + IXa)
DiseasesHemophilia A, B, C
🔍 Activated from INSIDE the blood vessel
tap to flip →
Why PTT Measures This Pathway
The Test Reagent
PTT adds a contact activator (kaolin or silica) + phospholipid + calcium to plasma. This bypasses tissue factor entirely, testing only the intrinsic path. If any factor in XII, XI, IX, or VIII is missing, PTT prolongs.
The Tenase Complex
VIIIa + IXa form the tenase complex on a phospholipid surface. This complex activates factor X. Without this complex (Hemophilia A or B), factor X can still be activated by the extrinsic pathway via VII, which is why PT stays normal.
Board Clue
Isolated PTT elevation = intrinsic pathway only. PT normal = extrinsic pathway intact. Differential: Hemophilia A/B/C, factor XII deficiency, heparin, lupus anticoagulant, factor VIII inhibitor.
Extrinsic Pathway
🩹
VII + Tissue Factor
Measured by PT / INR
TriggerTissue factor from damaged cells
Lab testPT elevated if broken
Key factorFactor VII (shortest half-life)
Monitored byWarfarin INR
🔍 Factor VII: first to fall in liver disease and warfarin
tap to flip →
Why Factor VII Is the Key Indicator
Shortest Half-Life
Factor VII half-life is ~4-6 hours. In liver disease or early warfarin therapy, VII falls before other factors, causing PT/INR to rise while PTT stays normal. PT is more sensitive to liver dysfunction and warfarin than PTT.
Warfarin Logic
Warfarin inhibits VKOR, blocking regeneration of active vitamin K. Vitamin K-dependent factors (II, VII, IX, X) can't be carboxylated. Factor VII falls first (shortest half-life), so PT rises earliest. Monitor warfarin with PT/INR, not PTT.
Isolated PT Elevation
PT up, PTT normal = only extrinsic pathway affected. Differential: warfarin early dose, vitamin K deficiency (early), isolated factor VII deficiency, mild liver disease affecting VII first.
Common Pathway
⚡
X → V → II → Fibrinogen
Affects BOTH PT and PTT
ActivationProthrombinase complex (Xa + Va)
Master enzymeThrombin (IIa)
End productFibrin cross-linked by XIII
Both PT + PTT upThink DIC, liver, warfarin
🔍 Both tests probe this pathway eventually
tap to flip →
Thrombin: The Master Enzyme
What Thrombin Does
Thrombin (IIa) converts fibrinogen to fibrin, activates factors V, VIII, and XIII, activates Protein C (anticoagulant feedback), and activates platelets via PAR-1 and PAR-4 receptors. One enzyme, entire system.
Both PT and PTT Elevated
If both are elevated, the problem is either in the common pathway (X, V, II, I deficiency) or something systemic that depletes everything: DIC (consumption), liver failure (can't synthesize), or warfarin/Vit K deficiency.
Factor V Leiden Trap
Factor V Leiden is a mutation making factor Va resistant to Protein C degradation. PT and PTT are NORMAL. It's a hypercoagulable state, not a bleeding disorder. Don't confuse it with factor V deficiency.
Vitamin K Factors
🌿
II, VII, IX, X, Protein C/S
Require gamma-carboxylation to function
Mnemonic1972 (IX, VII, II, X)
Inhibited byWarfarin (blocks VKOR)
Also deficient inMalabsorption, liver disease
ReversalVitamin K, FFP, 4-factor PCC
🔍 VII falls first (shortest half-life)
tap to flip →
Why Warfarin Takes Days to Work
Trace It
Warfarin inhibits VKOR, stopping recycling of vitamin K epoxide back to active vitamin K. Without active vitamin K, factors II, VII, IX, X, Protein C, and Protein S can't be gamma-carboxylated. They're made but non-functional.
Day 1 Warfarin Paradox
Protein C (half-life ~8h) and Protein S fall FIRST before procoagulant factors. Transient hypercoagulable state. That's why you bridge with heparin when starting warfarin for acute VTE. Without bridging, a warfarin-induced clot can form.
Emergency Reversal
For urgent reversal: 4-factor PCC gives immediate factor replacement. Add IV vitamin K for sustained reversal (12-24h to work alone). For non-urgent: oral vitamin K alone. Time-to-reversal matters for the management question.
Warfarin Mechanism
💊
VKOR Inhibitor
Vitamin K epoxide reductase complex inhibitor
PT/INRElevated (monitored)
PTTNormal at low doses
ReversalVitamin K + 4-factor PCC / FFP
NOT reversed byProtamine (that's heparin)
🔍 PT rises first because VII has shortest half-life
tap to flip →
Warfarin vs Heparin: Know the Differences
Warfarin Monitoring
Monitored with PT/INR. Target INR 2-3 for most indications (2.5-3.5 for mechanical heart valves). Takes 3-5 days to reach therapeutic effect. The delay is how long it takes existing functional factors to be used up.
Heparin Monitoring
Unfractionated heparin (UFH) monitored with PTT. LMWH monitored with anti-Xa level (PTT doesn't reliably reflect LMWH). UFH reversed with protamine sulfate. LMWH: protamine partially reverses.
DOACs
Rivaroxaban, apixaban (anti-Xa), dabigatran (direct thrombin inhibitor). No routine monitoring needed. They may prolong PT or PTT but the levels don't correlate well with anticoagulation intensity. Use specific anti-Xa or anti-IIa assays if needed.
Thrombin
📸
Factor IIa: Converts fibrinogen → fibrin
The master enzyme of the common pathway
ConvertsFibrinogen → Fibrin
ActivatesV, VIII, XIII, Protein C
Activates platelets viaPAR-1 and PAR-4 receptors
Inhibited byAntithrombin III (heparin cofactor)
🔍 Thrombin both amplifies clotting AND shuts it off via Protein C
tap to flip →
Thrombin's Dual Role
Procoagulant Amplification
Thrombin activates factors V and VIII (positive feedback, amplifying the cascade), XIII (cross-links fibrin for a stable clot), and platelets via PAR-1 and PAR-4. One molecule of thrombin triggers a massive downstream amplification.
Anticoagulant Feedback
When thrombin binds thrombomodulin on intact endothelium, it activates Protein C. Activated Protein C + Protein S destroys factors Va and VIIIa, shutting down amplification. The clot self-limits in healthy areas.
Heparin Target
Unfractionated heparin activates antithrombin III, which then inhibits thrombin (IIa) AND factor Xa. That's why UFH prolongs PTT. LMWH mainly inhibits Xa, less effect on IIa, which is why PTT doesn't reliably reflect LMWH activity.
🔑1972 = Vitamin K-dependent factors: write 1, 9, 7, 2 and you get factors IX, VII, II, X. Add Protein C and S. Everything warfarin depletes.⚡Thrombin does EVERYTHING: converts fibrinogen, activates platelets, amplifies V and VIII, AND shuts itself off via Protein C. One enzyme, the whole show.📈PT up alone = extrinsic (VII). PTT up alone = intrinsic (XII, XI, IX, VIII). Both up = common pathway OR DIC OR liver disease OR high-dose warfarin. The tests tell you the pathway.
The Master Comparison
Feature
Hemophilia A/B
vWD
DIC
TTP
HIT
PT
Normal
Normal
↑↑
Normal
Normal
PTT
↑↑
↑ or normal
↑↑
Normal
Normal
Platelets
Normal
Normal (except 2B)
↓↓
↓↓↓
↓↓
Bleeding time
Normal
↑
↑
↑
Normal
Bleeding type
Deep (joints, muscle)
Mucosal (nose, GI, menses)
Both + oozing
Purpura + organ damage
Thrombosis (not bleeding)
Mixing study
Corrects
Corrects
Corrects (factors consumed)
N/A (PTT normal)
N/A (PTT normal)
Schistocytes
No
No
Yes
Yes
No
D-dimer
Normal
Normal
↑↑↑
Normal or mild ↑
Normal
Key test
Factor VIII/IX assay
vWF antigen, ristocetin
Fibrinogen, D-dimer
ADAMTS13
PF4-heparin Ab, SRA
Clinical Images
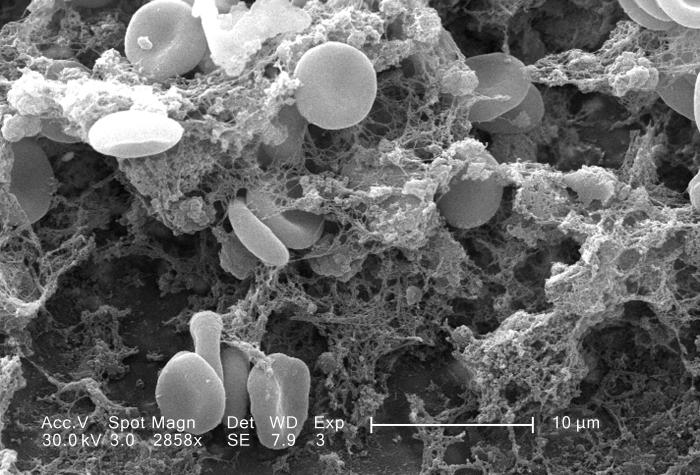
📷 Fibrin clot SEM · tap to expand
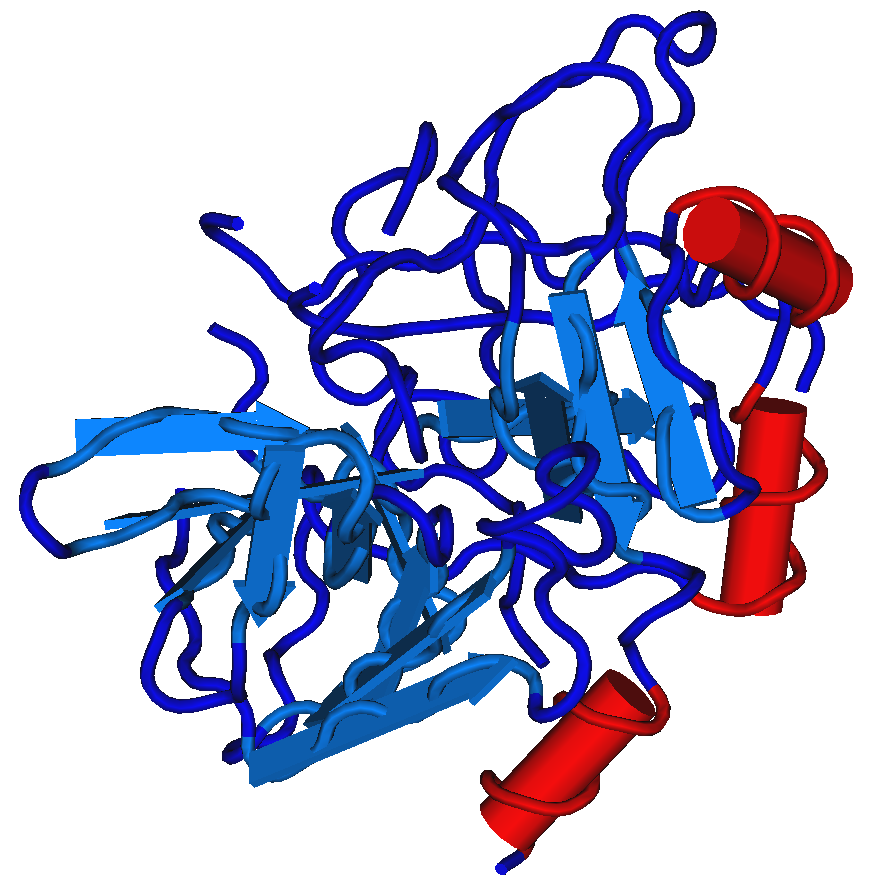
📷 Thrombin structure · tap to expand
📷The fibrin clot under electron microscopy looks like a mesh of yarn trapping red blood cells. In DIC that mesh is everywhere, shredding RBCs into schistocytes.🔪Thrombin's 3D structure has a deep groove (active site) where fibrinogen peptides dock before being cleaved. Dabigatran jams this groove directly, hence "direct thrombin inhibitor."🏴Coagulation cascade: BOTH pathways converge at factor X. Factor X to fibrin = common pathway. If you only know one fact: factor X is the bottleneck where both pathways meet.
Decision Tree: Elevated PTT, Now What?
Walk through this the way you'd think on test day. I'll quiz you at each branch.
PTT is elevated. First question: what's the PT?
PT is normal (isolated PTT elevation)
PT is also elevated (both up)
Good. Isolated PTT elevation. The problem is in the intrinsic pathway. Next step: order a mixing study. Does PTT correct?
Yes, PTT corrects → Factor deficiency
No, PTT doesn't correct → Inhibitor
Both PT and PTT elevated. The problem is in the common pathway or something systemic. Think about:
Liver disease · liver makes most factors (check albumin, LFTs)
Warfarin / Vitamin K deficiency · affects II, VII, IX, X
Common pathway factor deficiency (X, V, II, I)
Exactly. When BOTH PT and PTT are elevated, the differential is: DIC (sick patient, low fibrinogen, high D-dimer), liver failure (makes almost all factors), vitamin K deficiency/warfarin (factors II, VII, IX, X are vitamin K-dependent), or rare common pathway deficiencies. DIC is the emergency. Check the fibrinogen and D-dimer first.
PTT corrects on mixing = factor deficiency. Who's the patient?
Boy with deep bleeding (joints, muscles) → Hemophilia A or B (X-linked, order factor VIII then IX levels)
Anyone with mucosal bleeding (nosebleeds, heavy periods) + ↑ bleeding time → vWD (order vWF antigen, ristocetin cofactor)
No bleeding at all → Factor XII deficiency (lab finding only, no treatment needed)
That's the framework. Deep bleeding + boy = hemophilia.Mucosal bleeding + prolonged bleeding time = vWD.Elevated PTT + no bleeding = factor XII. The factor assays confirm which one.
PTT doesn't correct on mixing = inhibitor. Does the patient have bleeding or clotting?
Bleeding (severe, new-onset in older adult) → Acquired Factor VIII inhibitor
The paradox makes this a board favorite. Lupus anticoagulant: elevated PTT, doesn't correct, but the patient clots. Acquired factor VIII inhibitor: elevated PTT, doesn't correct, and the patient bleeds severely. The clinical picture tells you which one. Always ask: is this patient bleeding or clotting?
Elimination Game
Each scenario gives you clues. Eliminate diagnoses one by one until only the answer remains.
Clinical Vignettes
Patients are lining up. They're all bleeding (or clotting) for different reasons. Figure out why.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 5, 2026 at 8:17 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.
Bone Wizardry · Coagulation & Bleeding Disorders
clinical Walkthrough
clinical Walkthrough
Original clinical vignettes. Shuffled, never-repeat, full explanations for every choice.