Intrinsic (contact activation) and extrinsic (tissue factor) both funnel into the common pathway.
Why It Exists
Hemostasis prevents bleeding after vessel injury. Three steps: vasoconstriction, platelet plug (primary), fibrin clot (secondary, the cascade).
The Funnel
Both intrinsic and extrinsic pathways activate Factor X. Once Xa forms, it's the common pathway to thrombin to fibrin.
The Lab Readout
PT/INR measures the extrinsic pathway (Factor VII plus common). PTT measures the intrinsic pathway (XII, XI, IX, VIII plus common). Thrombin time measures fibrinogen conversion.
The High Yield Rule
Know which factor deficiency prolongs PT only (VII), PTT only (VIII, IX, XI, XII), or both (X, V, II, I). Factor XIII deficiency: both are NORMAL (clot forms, just doesn't crosslink).
Opening Challenge
A 28 year old woman is found to have isolated PTT prolongation on pre op labs. Her PT is normal. She has no personal or family history of bleeding. Which factor deficiency is most likely, and does it require surgical management?
Answer: B. Factor XII deficiency is the classic board trap: it prolongs PTT significantly but causes zero clinical bleeding. In the contact activation pathway, Hageman factor (XII) starts the cascade in the test tube, but in vivo thrombin generation is driven by the extrinsic pathway (TF/VIIa). Factor XII deficiency is discovered on pre op labs and NEVER treated. Factor VIII and IX deficiencies (hemophilia A/B) cause severe bleeding. Factor XI is variable (more bleeding with surgery and trauma, less so spontaneously).
The Cascade Step by Step
Tap any factor to see what it does.
Tap a factor
Click any node in the cascade to read what it does, what activates it, and why it matters clinically.
The Key Factors
Tap to flip. Front: where it fits. Back: why it matters.
🪨
Factor VIII
Hemophilia A when deficient
Pathway: Intrinsic cofactor
Activated by: Thrombin
Activates: IXa complex (tenase)
Lab: PTT prolonged, PT normal
MOST COMMON HEMOPHILIA
Tap to flip
What It Does
Cofactor for IXa in the tenase complex on phospholipid surfaces; IXa plus VIIIa activate Factor X.
Hemophilia A
X linked recessive; bleeds into joints (hemarthrosis), muscles, and CNS. Severity tracks with the Factor VIII level.
Treatment
Recombinant Factor VIII; DDAVP raises vWF which carries VIII and can help mild cases.
Lock It
PTT prolonged plus normal PT plus bleeding equals Hemophilia A; distinguish from vWD by ristocetin agglutination test.
🧬
Factor IX
Hemophilia B is Christmas disease
Pathway: Intrinsic
Activated by: XIa
Activates: X (with VIII)
Lab: PTT prolonged
X LINKED LIKE HEMOPHILIA A
Tap to flip
What It Does
Serine protease; forms the tenase complex with VIIIa on the membrane surface; activates Factor X.
Hemophilia B
X linked recessive; identical clinical picture to Hemophilia A; differentiated by factor assay.
Treatment
Recombinant Factor IX.
Lock It
Clinically identical to Hemophilia A; differentiated only by factor assay; both show PTT elevated plus PT normal plus male plus joint bleeds.
⚡
Factor VII
The Extrinsic Pathway Gate
Pathway: Extrinsic only
Activates: Tissue factor complex
Half life: 4 to 6 hours (SHORTEST)
Lab: PT/INR prolonged only
SHORTEST HALF LIFE, PT RISES FIRST
Tap to flip
What It Does
Becomes VIIa when TF is exposed after vessel injury; TF/VIIa complex activates both IX and X.
Warfarin Connection
Factor VII has the shortest half life of all vitamin K factors; PT/INR rises first when warfarin is started because VII falls first.
Liver Disease
Factor VII is most sensitive to acute liver injury because of its short half life; early indicator of synthetic dysfunction.
Lock It
Isolated PT prolongation equals Factor VII deficiency; early warfarin equals Factor VII falls first equals PT rises before PTT.
🔗
Von Willebrand Factor
Platelet bridge plus FVIII carrier
Source: Endothelium and platelets
Roles: Platelet adhesion plus carry FVIII
Lab: PTT elevated, bleeding time long
MOST COMMON INHERITED BLEEDING DISORDER
Tap to flip
What It Does
Binds subendothelial collagen; platelets adhere via GPIb; carries Factor VIII protecting it from degradation.
vWD Types
Type I is quantitative decrease, most common, DDAVP works; Type II is qualitative defect; Type III is complete absence, severe.
Lab Pattern
PTT elevated because VIII is low; bleeding time elevated because platelet adhesion is impaired; ristocetin agglutination test fails in Type I and III.
Lock It
DDAVP is the treatment for mild Type I vWD; platelet adhesion defect plus reduced Factor VIII equals vWD; ristocetin test distinguishes vWD from hemophilia.
🌀
Thrombin
The Central Enzyme (Factor IIa)
Source: Prothrombin (Factor II)
Activates: Fibrinogen, V, VIII, XIII, platelets
Inhibited by: Antithrombin III
ACTIVATES ITS OWN AMPLIFIERS
Tap to flip
What It Does
Converts fibrinogen to fibrin; activates Factor XIII for crosslinking; amplifies itself by activating V and VIII; activates platelets.
Positive Feedback
Thrombin activates V and VIII which in turn help make more thrombin: exponential amplification once started.
Anticoagulant Targets
Direct thrombin inhibitors: hirudin, bivalirudin, argatroban, dabigatran; antithrombin III inhibits thrombin when heparin binds and accelerates it 1000x.
Lock It
Dabigatran is a direct thrombin inhibitor; reversal agent is idarucizumab; antithrombin III deficiency equals recurrent VTE plus heparin resistance.
🎯
Factor Xa
The Common Pathway Start
Source: Intrinsic plus extrinsic converge
Activates: Prothrombin complex
Cofactor: Factor Va
Inhibited by: Antithrombin III
WHERE BOTH PATHWAYS MEET
Tap to flip
What It Does
With Factor Va (prothrombinase complex), activates prothrombin to thrombin; requires phospholipid surface and calcium.
Heparin Target
UFH and LMWH both inhibit Xa through antithrombin III; LMWH is more selective for Xa than UFH.
Direct Xa Inhibitors
Rivaroxaban, apixaban, edoxaban (the "xabans"); reversal: andexanet alfa.
Lock It
Rivaroxaban and apixaban directly inhibit Xa without needing antithrombin III; they are monitored by anti Xa levels, not PTT; reversal with andexanet alfa.
Reading the Coag Panel
PT plus PTT tells you where the problem is before you even order a factor assay.
PTT High, PT Normal
Factors: Intrinsic pathway: VIII, IX, XI, or XII.
Drug: Heparin (UFH) effect.
Clinical: Hemophilia A or B (joint bleeds, male), Factor XI deficiency (variable), or Factor XII deficiency (NO bleeding).
PT High, PTT Normal
Factors: Extrinsic only: Factor VII.
Drug: Early warfarin (VII falls first because shortest half life).
Clinical: Early liver dysfunction, mild vitamin K deficiency, isolated Factor VII deficiency.
Both PT and PTT High
Factors: Common pathway: X, V, II, I (fibrinogen).
Drug: Supratherapeutic warfarin, high dose heparin.
Clinical: Severe liver disease, DIC, vitamin K deficiency (advanced), or massive transfusion.
Both Normal, But Bleeding
Factors: Factor XIII deficiency (clot forms but doesn't crosslink).
Other: Platelet disorder, mild vWD, vascular cause (scurvy, Ehlers Danlos).
Clinical: Delayed bleeding after surgery or umbilical stump bleeding in newborns is classic for XIII deficiency.
Drug Targets at a Glance
Drug
Target
Monitor
Reversal
Heparin (UFH)
Xa and IIa via ATIII
PTT (mainly)
Protamine sulfate
LMWH (enoxaparin)
Mainly anti Xa
Anti Xa level (PTT unreliable)
Protamine (partial)
Warfarin
Vitamin K factors: II, VII, IX, X plus C, S
PT/INR
Vitamin K, FFP, PCC
Rivaroxaban, Apixaban
Direct Xa inhibition
Anti Xa (specialized)
Andexanet alfa
Dabigatran
Direct thrombin (IIa)
Thrombin time, ecarin time
Idarucizumab
Fondaparinux
Pure anti Xa via ATIII
Anti Xa level
No specific agent
Pearl: Heparin works only when antithrombin III is present. A patient with heparin resistance (PTT won't budge despite escalating doses) likely has ATIII deficiency. Treat with ATIII concentrate or FFP first, then resume heparin.
Which Factor is Missing?
The bleeding history plus the lab pattern plus the demographic equals the diagnosis.
Patient 1
8 year old male. Deep muscle hematoma after minor trauma. Uncle had similar problem. PTT: 72s (normal less than 35). PT: normal. Bleeding time: normal.
Tap to reveal diagnosis
Hemophilia A (Factor VIII deficiency). X linked, male, deep tissue bleeds (not mucosal), PTT up and PT normal. Order Factor VIII assay to confirm. Treatment: recombinant Factor VIII; DDAVP for mild cases. Hemophilia B (Factor IX) looks identical clinically; the factor assay is the only differentiator.
Patient 2
45 year old woman. Preoperative labs. No bleeding history. PTT: 78s. PT: normal. She had a DVT 2 years ago.
Tap to reveal diagnosis
Factor XII deficiency (Hageman factor). Paradoxically, Factor XII deficiency is associated with thrombosis (not bleeding) because XII normally activates fibrinolysis. The high PTT requires no treatment. Do NOT delay surgery. This is the classic pre op lab trap: massive PTT elevation with zero bleeding history.
Patient 3
30 year old woman. Heavy menstrual periods since menarche. Nosebleeds. Mother had similar history. PTT: 44s. Bleeding time: 10 min (elevated). Platelet count: normal. Ristocetin agglutination: reduced.
Tap to reveal diagnosis
Von Willebrand Disease Type I. vWD is the most common inherited bleeding disorder. Mucosal bleeding (menorrhagia, epistaxis), PTT mildly elevated (because vWF carries Factor VIII), and the ristocetin test locks it in. Treat with DDAVP for Type I (releases stored vWF from endothelium). Avoid aspirin and NSAIDs.
Patient 4
75 year old male on warfarin for AFib. INR: 1.1. Now has acute DVT. Heparin started. Day 3: PTT 24s (subtherapeutic). Required heparin doses increasing.
Tap to reveal diagnosis
Antithrombin III deficiency. Heparin works by binding and activating antithrombin III. Without ATIII, heparin cannot function. Key clue: heparin resistance (escalating doses, PTT won't rise). Treat with ATIII concentrate or FFP first, then resume heparin. ATIII deficiency is also a hypercoagulable state that explains the warfarin failure and the DVT.
When the Cascade Collapses
Disseminated Intravascular Coagulation: too much coagulation everywhere leads to clotting factors running out, then bleeding.
The Trap: DIC consumes clotting factors AND platelets AND fibrinogen, so you paradoxically bleed despite initial excess clotting. The patient who is hemorrhaging from every line, every wound, and every mucosal surface after sepsis or obstetric disaster has DIC until proven otherwise.
The Mechanism Chain
1
Trigger: massive activation of coagulation (obstetric disaster like placental abruption or amniotic fluid embolism, sepsis, trauma, acute leukemia especially APML).
2
Widespread fibrin clot formation in microvasculature (microthrombi everywhere).
3
Ischemia from microthrombi in organs: kidneys, brain, skin (purpura fulminans), lungs.
4
Clotting factors consumed: fibrinogen drops, PT and PTT both rise.
5
Platelets consumed: thrombocytopenia develops.
6
Fibrinolysis activated: D dimers and fibrin split products rise dramatically.
7
Bleeding from coagulation factor depletion: oozing from IV sites, mucosal hemorrhage, intracranial bleed.
DIC Lab Pattern
PT: elevated
PTT: elevated
Platelets: low
Fibrinogen: LOW (the key, because consumed)
D dimers: markedly elevated (often greater than 5x normal)
Treat the underlying cause first. FFP for active bleeding (replaces factors). Cryoprecipitate if fibrinogen is less than 100 mg/dL. Platelets if less than 50k with active bleeding. Heparin is controversial: only used in DIC from APML or thrombosis dominant DIC patterns.
Clinical Pearl: DIC vs Liver Disease. Both can give elevated PT/PTT and low platelets. The discriminators:
Liver disease: Factor VIII is NORMAL or elevated (made by endothelium, not just liver). D dimer mildly elevated (poor clearance). DIC: Factor VIII is LOW (consumed by massive thrombin activation). D dimer markedly elevated (active fibrinolysis). Fibrinogen drops rapidly.
If you see preserved Factor VIII with coagulopathy, think liver. If Factor VIII is consumed along with everything else, think DIC.
Challenge before reveal: which single lab pattern separates liver disease from DIC when PT, PTT, and platelets are all abnormal?
Preserved Factor VIII points to liver disease. Factor VIII is made by endothelium, so liver failure can spare it. DIC consumes Factor VIII with the rest of the cascade, so it falls with fibrinogen while D dimer rises sharply.
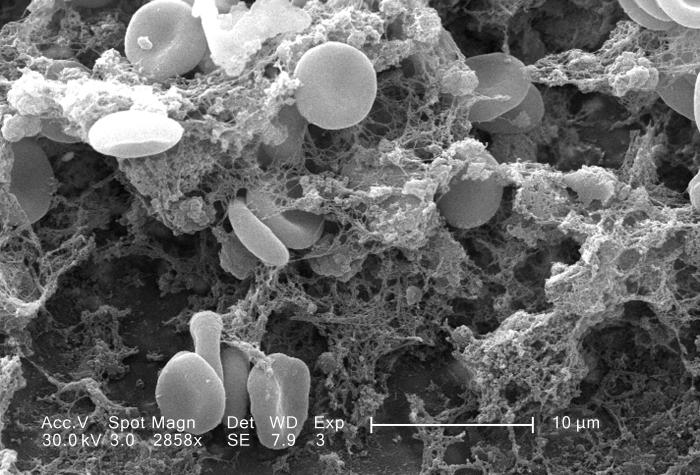
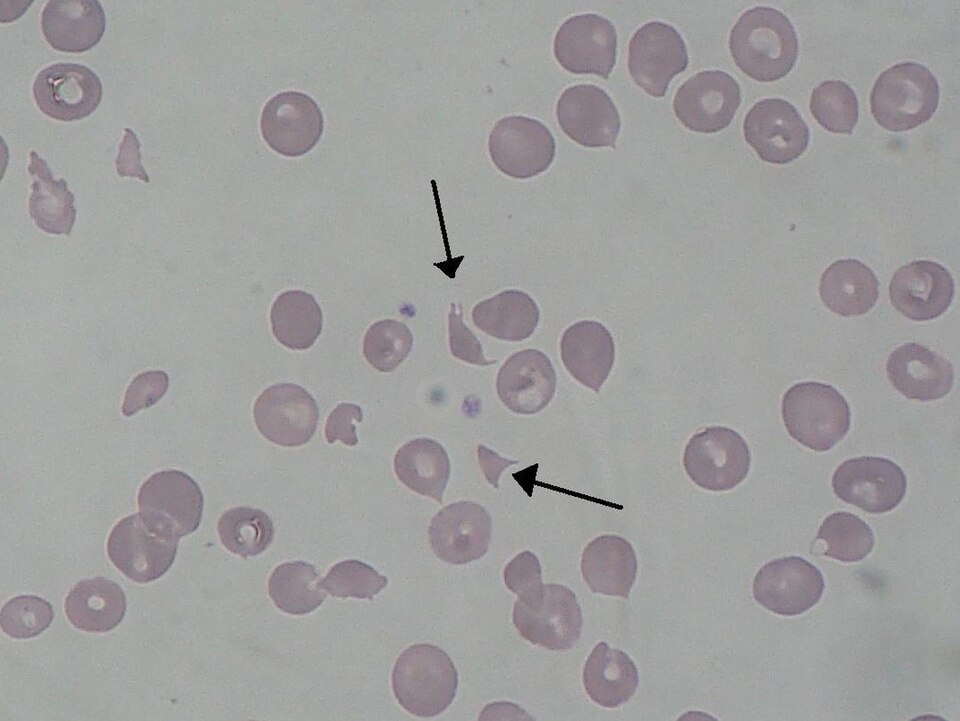
Fibrin mesh and trapped blood elements are the final physical product of thrombin activation.Hypercoagulable states push the cascade toward thrombosis rather than bleeding.Schistocytes support a microangiopathic process when fibrin strands shear red cells.
Coagulation: Board Style
5 vignettes. Tap to answer.
Question 1 of 5
A 32-year-old woman is brought to the preoperative clinic before an elective cholecystectomy. She reports no epistaxis, menorrhagia, easy bruising, hemarthroses, or prior surgical bleeding, and her family history is negative for bleeding disorders. Vital signs are within normal limits, and physical examination reveals no petechiae, ecchymoses, or joint swelling. Laboratory testing shows PTT 96 seconds, PT 12 seconds, platelet count 244,000/mm3, and hemoglobin 13.4 g/dL. Which of the following is the most likely next step for this coagulation abnormality?
Answer: B. Factor XII (Hageman) deficiency prolongs PTT markedly but causes NO clinical bleeding. It paradoxically associates with thrombosis (reduced fibrinolytic pathway activation). Never give FFP; never delay surgery; no treatment needed. This is a pre op lab trap. Distinguish from hemophilia by clinical history (no bleeding) and sex (Factor XII affects both sexes equally).
Question 2 of 5
A 71-year-old man is started on warfarin after new atrial fibrillation is found during an office visit. He has no bleeding, chest pain, or neurologic symptoms. Vital signs are stable, and physical examination shows an irregularly irregular pulse without edema or hepatosplenomegaly. Twenty-four hours later, laboratory testing shows INR 1.8, PT 19 seconds, PTT 31 seconds, platelet count 218,000/mm3, and normal liver enzymes. Which of the following best explains the early rise in PT before PTT?
Answer: B. Factor VII has a 4 to 6 hour half life, the shortest of II, VII, IX, X. When warfarin blocks vitamin K dependent carboxylation, Factor VII depletes first, prolonging the PT (extrinsic) before PTT (intrinsic). This is why early INR does NOT mean adequate anticoagulation for DVT treatment: intrinsic pathway factors (II especially, with 60 hour half life) are still functioning. Heparin bridge is needed until therapeutic INR for 2 plus days.
Question 3 of 5
Two adolescent brothers are evaluated in hematology clinic because of recurrent bleeding episodes. The older brother has painful knee swelling after minor trauma but no mucosal bleeding; examination reveals a warm knee effusion. His labs show PTT 68 seconds, PT 12 seconds, bleeding time 4 minutes, and Factor VIII activity 3%. The younger brother has frequent epistaxis and gingival bleeding; examination reveals scattered oral mucosal petechiae. His labs show PTT 52 seconds, bleeding time 14 minutes, Factor VIII activity 28%, and reduced ristocetin-induced platelet agglutination. Which of the following is the most likely diagnosis pair?
Answer: B. Brother 1: extremely low Factor VIII plus normal bleeding time plus normal ristocetin equals Hemophilia A (intrinsic problem, platelet adhesion intact, no vWF defect). Brother 2: mildly low Factor VIII plus prolonged bleeding time plus reduced ristocetin equals vWD (vWF deficiency means Factor VIII is less protected so it's low, AND platelet adhesion is impaired so bleeding time is prolonged). The ristocetin test is the key distinguisher: vWD fails ristocetin induced platelet agglutination; hemophilia does not.
Question 4 of 5
Two hospitalized patients are evaluated for abnormal coagulation tests. Patient A is a 58-year-old man admitted with alcoholic cirrhosis, ascites, and mild gum bleeding; examination reveals jaundice and spider angiomas. Patient B is a 64-year-old woman admitted with gram-negative sepsis who develops oozing from venipuncture sites and mottled extremities; examination reveals fever, hypotension, and diffuse ecchymoses. Both have PT and PTT elevation with platelets near 60,000/mm3. Patient A has fibrinogen 180 mg/dL, D dimer 2 times normal, and Factor VIII 140%. Patient B has fibrinogen 80 mg/dL, D dimer 18 times normal, and Factor VIII 35%. Which of the following is the most likely diagnosis pair?
Answer: C. The discriminating factors are fibrinogen level, D dimer elevation degree, and Factor VIII. In liver disease: Factor VIII is made by endothelial cells (not just hepatocytes) so it's preserved or even elevated. In DIC: Factor VIII is consumed by massive thrombin activation, so it drops. D dimer elevation in DIC is dramatic (greater than 5x); in liver disease it's modest (poor clearance). Fibrinogen is often preserved in liver disease until very late, while DIC consumes it rapidly.
Question 5 of 5
A 72-year-old man is brought to the emergency department after sudden headache, vomiting, and right-sided weakness. He takes dabigatran for atrial fibrillation and has not taken warfarin or heparin. Blood pressure is 178/96 mm Hg, and physical examination reveals confusion, right arm weakness, and slurred speech. CT of the head shows an acute intracranial hemorrhage; laboratory testing shows platelet count 231,000/mm3, INR 1.1, and prolonged thrombin time. Which of the following is the most appropriate pharmacologic reversal agent?
Answer: C. Dabigatran is a direct thrombin inhibitor (DTI). Its specific reversal agent is idarucizumab (a monoclonal antibody Fab fragment that binds dabigatran with extremely high affinity). Vitamin K reverses warfarin. Andexanet alfa reverses Factor Xa inhibitors (rivaroxaban, apixaban). Protamine reverses heparin (and partially LMWH). Each drug class has its own reversal agent: this is a high yield board pattern.
Board·Style Walkthrough
Board·Style Walkthrough
Original board·style vignettes. Shuffled, never·repeat, full explanations for every choice.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 1, 2026 at 10:03 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.