GH excess before the growth plates close. Everything grows. Everything. Let's figure out why and what to do about it.
🆕 OPENER · Can you crack it?
A 14-year-old boy is brought in because none of his clothes fit anymore. His height is at the 99th percentile, his feet are two sizes wider than last year, and his forehead seems to be pushing forward. His palms are notably broad and doughy. He sweats constantly, even in air conditioning. Fasting glucose comes back at 138 mg/dL. X-ray shows bone age of 16. What single test would both screen and confirm the underlying hormonal excess?
Correct. IGF-1 is the screening test because GH has a short half-life and pulses unpredictably. IGF-1 is a stable, downstream marker. If IGF-1 is elevated, you confirm with the oral glucose suppression test: 100g glucose should suppress GH below 5 ng/mL in a normal person. If it doesn't suppress, you have your answer. Then MRI to find the adenoma.
Think about what's driving this kid's growth. The clue is the hands, the sweating, the glucose, AND the tall stature together. That combination points to one hormone. Cortisol causes short stature, not tall. Catecholamines come with hypertensive crises. TSH doesn't explain the linear growth or the broad hands. The hormone you want is the one that drives bone and soft tissue growth. Try again or tap C to see why.
THE MECHANISM
The GH-IGF-1 Axis
Tap each node to see what it does and what goes wrong when it breaks
Step 1 · Hypothalamus
GHRH
Growth Hormone Releasing Hormone
GHRH is the trigger. When your body needs to grow (or is stressed), the hypothalamus fires GHRH. Think of it like the hypothalamus sending a text to the pituitary saying "turn on the growth factory." Somatostatin is the hypothalamus's "stop" text, sent after growth occurs.
Board angle: Octreotide works as a somatostatin analogue, which is exactly why it shuts down GH release. It mimics the "stop" signal.
↓
Step 2 · Anterior Pituitary
GH
Growth Hormone (Somatotropin)
The pituitary releases GH in pulses, mainly after the first REM cycle of sleep. This is why kids grow at night.
In gigantism and acromegaly, a somatotroph adenomaA benign tumor of the growth hormone-secreting cells in the anterior pituitary. Autonomous = it ignores all feedback signals. keeps firing GH nonstop regardless of what the hypothalamus says. It's gone rogue. No off switch.
Why the glucose test works: Normally, eating glucose tells GH to shut up (sugar means you're fed, not stressed). In a GH-secreting adenoma, glucose suppression fails because the tumor doesn't listen.
↓
Step 3 · Liver
IGF-1
Insulin-like Growth Factor 1 (Somatomedin)
GH tells the liver to make IGF-1. IGF-1 is the actual growth signal that reaches bones, tendons, and muscles.
Why screen with IGF-1 and not GH? GH has a half-life of about 20 minutes and pulses unpredictably. One random GH level tells you almost nothing. IGF-1 is stable and reflects the running average of GH over days. If IGF-1 is elevated, GH has been chronically high.
Liver disease caveat: A cirrhotic liver can't make IGF-1 even with high GH. So a patient with liver disease can have low IGF-1 despite elevated GH. Board trap incoming.
↓
Step 4 · Growth Plates
Bone & Soft Tissue
Where size happens
In children (open growth plates): IGF-1 drives linear growth. The long bones get longer. Kid becomes extremely tall. This is gigantism.
In adults (closed growth plates): The bones can't get longer. Instead they get wider. Hands and feet expand. Jaw protrudes. Forehead pushes forward. Organs enlarge. This is acromegaly.
The hat and shoes clue: "My hat doesn't fit anymore" = skull/jaw expanding. "I went up a shoe size" = feet widening. Classic board-exam signal for acromegaly.
Tap any node to expand the detail. Each step matters for the quiz later.
⚠️
Board Trap: Gigantism vs Acromegaly is ONLY About Growth Plate Status
The cause is identical (usually a pituitary adenoma). The diagnosis workup is identical. The treatment is identical. The only difference is whether the epiphyseal plates are open or closed when GH excess starts. Open plates = gigantism (linear growth). Closed plates = acromegaly (widening growth only). Some people get GH excess as a teen and end up with BOTH: they're very tall AND have acromegalic features.
🔑
One disease, two names, one difference. Growth plates open = Gigantism. Growth plates closed = Acromegaly. The tumor is the same. The workup is the same. The plates decide the phenotype.
QUICK REFERENCE
The Six Players
Tap each card to flip it. Board-critical facts on the back.
Before Growth Plate Fusion
Gigantism
GH excess in childhood
Linear growth explodes. The bones get longer, not just wider.
tap to flip
The Setup
Somatotroph adenoma secreting GH before epiphyseal plates close. IGF-1 drives linear bone growth. Long bones lengthen unrestricted. Child grows far beyond normal height trajectory.
Key Features
Height at or above 99th percentile
Advanced bone age on X-ray
Broad hands and feet (soft tissue + bone)
Sweating, elevated glucose
Normal Tanner staging (not precocious puberty)
key pattern: Open growth plates + GH excess = linear growth = gigantism. Closed plates + same excess = only widening = acromegaly.
After Growth Plate Fusion
Acromegaly
GH excess in adulthood
Bones widen instead of lengthen. Ring and shoe sizes increase. Jaw juts forward.
tap to flip
The Setup
Same root cause as gigantism. But fused epiphyses can't lengthen. GH and IGF-1 drive periosteal bone widening and soft tissue overgrowth instead. Slow, insidious onset over years.
Key Features
Shoe/ring size increasing (classic board clue)
Jaw protrusion (prognathism), widened nose
Carpal tunnel syndrome (bilateral)
Cardiomegaly (#1 cause of death if untreated)
Sleep apnea, colon polyps, diabetes
key pattern: "My hat and shoes don't fit anymore" = acromegaly. Insidious, diagnosed late. Always post-epiphyseal closure.
Primary Mediator
IGF-1
Insulin-like Growth Factor 1
The real growth signal. GH just tells the liver to make it. IGF-1 does all the work.
tap to flip
Why IGF-1 Matters More Than GH
GH has a 20-minute half-life and pulses unpredictably throughout the day. A single random GH level is nearly useless. IGF-1 is stable and reflects the running average of GH over days.
Board Logic
Screen with IGF-1 first, not random GH
Elevated IGF-1 = chronic GH excess
Confirm with oral glucose suppression test
Liver disease caveat: cirrhosis lowers IGF-1 even with high GH
key pattern: IGF-1 is the screening test. Never use a random GH level to screen. Random GH can be normal even in a GH-secreting tumor.
Root Cause
Somatotroph Adenoma
GH-secreting pituitary tumor
Autonomous. Ignores all feedback. GH production doesn't stop regardless of glucose, IGF-1, or somatostatin.
tap to flip
The Tumor
Located in the anterior pituitary. Grows silently. Macroadenomas (>1cm) compress the optic chiasm above → bitemporal hemianopia. Compresses normal pituitary → hypopituitarism.
Cardiomegaly is the #1 cause of death. But there are several other complications that make it to clinical medicine.
tap to flip
High-Yield Complications
Cardiomegaly (IGF-1 on cardiomyocytes) = #1 killer
Carpal tunnel syndrome (median nerve compression)
Sleep apnea (macroglossia, soft tissue expansion)
Diabetes mellitus (GH is anti-insulin)
Colon polyps / colonoscopy screening required
Hyperhidrosis tracks with disease activity
key pattern: Cardiomegaly is the top killer in untreated acromegaly. Normalize IGF-1 = protect the heart. Sweating that gets worse = disease not controlled.
Treatment Ladder
Surgery to Radiation
4-step management
Transsphenoidal surgery first. Then octreotide. Then pegvisomant. Radiation is the last resort.
3. Pegvisomant (GH receptor blocker, different mechanism)
4. Radiation (last resort, slow, risk of hypopituitarism)
Critical Distinction
Octreotide suppresses GH secretion. Pegvisomant blocks GH action at the receptor. Different points of attack.
key pattern: Surgery fails → octreotide. Octreotide fails → pegvisomant. Never jump to radiation when medical options remain.
RECOGNITION
What They Look and Feel Like
Gigantism vs acromegaly side by side, and what connects them both
Gigantism
GH excess BEFORE epiphyseal closure
📷 Coarsened facial features · tap to expand
Feature
What You See
Why
Height
99th percentile or higher
Open growth plates respond to IGF-1, bones lengthen
Bone age
Advanced (bone age > chronologic age)
Excess GH/IGF-1 accelerates ossification
Facial bones
Frontal bossing, jaw protrusion
Flat bones of skull still respond to GH even with open plates
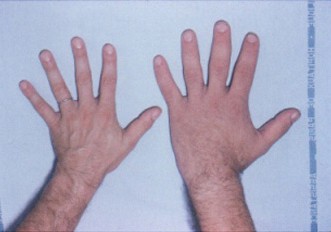
Hands/feet
Broad, doughy
Soft tissue hypertrophy from IGF-1
Glucose
Elevated (138 mg/dL in stem)
GH is catabolic, drives gluconeogenesis, causes insulin resistance
🔥The dead giveaway: tall kid + broad hands + sweating + elevated glucose + advanced bone age. That cluster on a clinical practice is gigantism until proven otherwise.
Acromegaly
GH excess AFTER epiphyseal closure
📷 Enlarged hands · tap to expand
Feature
What You See
Why
Height
Normal (plates already closed)
Can't lengthen what's already fused
Hands/feet
Ring/shoe size increasing over years
Periosteal bone widening + soft tissue expansion
Face
Jaw juts forward (prognathism), widened nose
Membranous bone continues to respond to GH
Carpal tunnel
Bilateral hand numbness/tingling
Soft tissue overgrowth compresses median nerve
Heart
CardiomegalyThe #1 cause of death in untreated acromegaly. The heart muscle (also soft tissue) hypertrophies, leading to heart failure over decades.
Most dangerous long-term complication. Kills before diabetes does.
💡"My hat and shoes don't fit anymore." Classic board setup for acromegaly. If you also see Paget's mentioned, distinguish: Paget's = high alk phos + sclerotic bones + older patient. GH excess = normal alk phos + soft tissue growth + young-to-middle age.
Features Shared by Both
Same root cause, same metabolic wreck
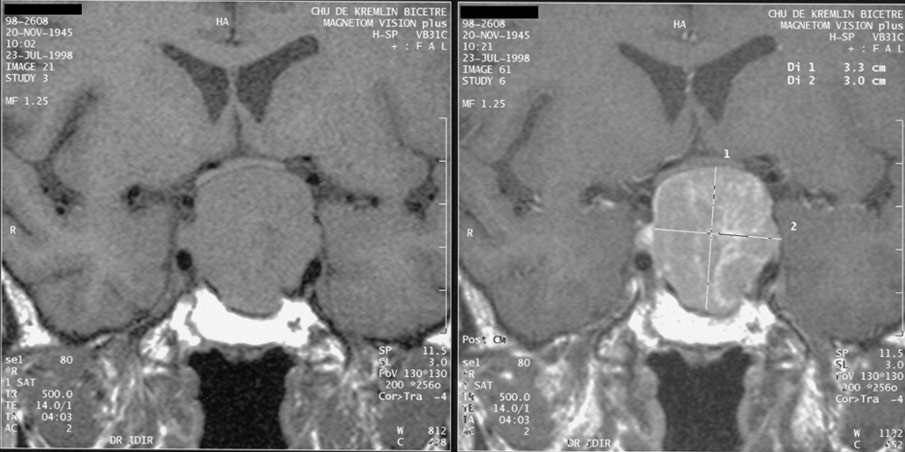
📷 Pituitary macroadenoma on MRI · tap to expand
Metabolic Effects
Insulin resistance (GH is anti-insulin)
Glucose intolerance or frank diabetes
Dyslipidemia
Autonomic / Secretory
Hyperhidrosis (excessive sweating)
Oily skin (sebaceous gland overgrowth)
Fatigue, weakness
Mass Effects (Adenoma)
Headaches (pressure)
Bitemporal hemianopia (optic chiasm compression)
Hypopituitarism if big enough
Organomegaly
Cardiomegaly (biggest killer)
Visceromegaly (liver, spleen, kidney)
Macroglossia (enlarged tongue)
Thyroid enlargement
⚠️
Board Trap: Sweating is Not Just "A Symptom"
Hyperhidrosis (excessive sweating) is one of the most reliable clinical markers of active GH excess and is actually used to track disease activity. If a patient with treated acromegaly says their sweating has gotten worse, that's a red flag for recurrence or inadequate control. The clinical medicine love this as a "symptom that tracks with disease activity."
THE WORKUP
How to Diagnose It
The clinical medicine test whether you know the order. Get the order wrong, get it wrong.
Here's the trap most students fall into: they order an MRI first. That's wrong. You confirm the hormone problem before you go hunting for the tumor. Why? Because a random GH level is useless (it pulses all day), and an MRI without biochemical confirmation is just expensive photography.
DIAGNOSTIC SEQUENCE
1
Serum IGF-1Also called somatomedin C. Stable marker that reflects average GH secretion over days. High IGF-1 = chronic GH excess. This is your screening test. level
Screening test. If elevated, proceed. Do NOT order a random GH level, it fluctuates too much to be useful.
2
Oral Glucose Suppression Test🔑100g glucose, check GH at 1-2 hours. Normal: GH suppresses below 5 ng/mL. GH-producing tumor: GH stays high because the adenoma doesn't care about glucose.
CONFIRMATORY test. Give 100g oral glucose. Measure GH at 1-2 hours. Normal suppression = GH falls below 5 ng/mL. Failure to suppress = GH-secreting adenoma confirmed.
3
MRI of the pituitary gland
Only AFTER biochemical confirmation. This localizes the adenoma. Most are macroadenomas (>1cm) by the time symptoms appear because growth is slow.
⚠️
Why does the oral glucose suppression test work as a confirmation test? You already know about the feedback loop: when blood sugar rises, GH should shut off (you're fed, not stressed, so stop growing). A normal pituitary responds to glucose and kills GH secretion. A somatotroph adenoma doesn't get that memo. It just keeps pumping. GH stays high. Diagnosis confirmed.
DIAGNOSTIC REASONING
Walk Through the Workup
A patient walks in with signs of GH excess. Walk through each decision point.
Step 1: A patient has extreme tall stature, broad doughy hands, and sweating. You suspect GH excess. What is your first test?
Exactly. IGF-1 is the screening test. GH pulses unpredictably with a 20-minute half-life. One random level can be normal even in a GH-producing tumor. IGF-1 reflects the running average of GH over days. Screen with IGF-1. Confirm later.
Not quite. Random GH is the classic trap. It pulses and can look normal even with a GH-secreting adenoma. Imaging before biochemical confirmation is expensive and non-specific. The right first move is IGF-1: stable, reliable, reflects chronic GH status.
Step 2: IGF-1 comes back elevated. What do you do to confirm GH excess?
Right. 100g oral glucose should suppress GH below 5 ng/mL in a healthy person. When blood sugar rises, the pituitary gets the "we're fed, stop growing" signal. A somatotroph adenoma ignores this signal. GH stays elevated. Failure to suppress = confirmed autonomous GH secretion.
The confirmatory test is the oral glucose suppression test. It exploits the normal negative feedback: glucose should suppress GH. If the adenoma ignores glucose, GH fails to suppress. That failure confirms autonomous secretion. GHRH stimulation would stimulate more GH, which is the opposite of what you want for confirmation.
Step 3: GH does not suppress below 5 ng/mL after 100g glucose. What is your next step?
Now you get the MRI. Biochemical confirmation came first. Now you know a GH-producing tumor exists. The MRI will localize it. Most are macroadenomas (>1cm) by the time symptoms are severe enough to bring the patient in, because the tumor grows slowly and symptoms develop over years.
You have biochemical confirmation now: image before treating. Octreotide is second-line after surgery, and you need to know what you are dealing with first. Repeating the OGTT after a clear failure adds nothing. MRI is the logical next step: find the tumor before deciding how to remove or treat it.
Step 4: MRI shows a 1.8cm pituitary macroadenoma. Surgery removes most of it. Post-op IGF-1 is still 3x the upper limit. What is the most appropriate next step?
Octreotide is second line. It mimics somatostatin, which suppresses GH release from the adenoma. Somatotroph tumors retain somatostatin receptors, so octreotide often works on the residual tumor cells directly. It also helps shrink the remaining tumor. Pegvisomant comes after octreotide fails, and radiation is last resort because it is slow and damages normal pituitary.
The escalation order matters here. Radiation takes years to work and causes hypopituitarism as collateral damage. Pegvisomant is third-line: it blocks GH at its receptor, a different mechanism from octreotide. But you go to octreotide first after failed surgery because it works in most patients and preserves pituitary function. Escalate in order.
THE FIX
Treatment Algorithm
Tap each step to see the mechanism and when you'd use it
First Line
Transsphenoidal Surgery
Remove the adenoma. The cure, when it works.
The anterior pituitary is tucked right behind the sphenoid sinus, which is why surgeons go through the nose ("transsphenoidal") rather than cracking open the skull. It's elegant: no brain retraction needed for small tumors.
When it works: Microadenomas (<1cm) have cure rates above 80-90%. Macroadenomas are harder to fully resect.
Success check: Post-op IGF-1 + oral glucose suppression test. If IGF-1 normalizes and GH suppresses, you're cured. If not, move to step 2.
Board pearl: Always ask "what confirms surgical cure?" Answer: normal IGF-1 + GH suppression below 1 ng/mL on OGTT.
Second Line (Medical)
Octreotide (Somatostatin Analogue)
When surgery doesn't fully work. Mimics somatostatin to suppress GH release.
Remember the feedback loop: somatostatin from the hypothalamus tells the pituitary to stop making GH. Octreotide is a synthetic somatostatin that works longer and more powerfully.
The adenoma STILL has somatostatin receptors (unlike its resistance to glucose). So octreotide actually works on tumor cells to suppress GH secretion.
Also used for: pre-op tumor shrinkage, patients who can't have surgery, carcinoid syndrome, glucagonoma, insulinoma, portal hypertension (remember for clinical practice).
Side effects: GI upset (nausea, diarrhea), cholelithiasis (it slows gallbladder emptying), and bradycardia.
Third Line (Refractory)
Pegvisomant (GH Receptor Antagonist)
Blocks GH from binding its receptor. Different mechanism from octreotide.
Pegvisomant is a GH receptor blocker. Instead of suppressing GH secretion, it blocks GH from doing anything at all. Think of it like changing the locks on the door.
Why third line? It's expensive, requires daily injections, and because it blocks GH action rather than GH release, it doesn't shrink the tumor. You have to keep monitoring for tumor growth with MRI.
Board distinction: Octreotide suppresses GH release. Pegvisomant blocks GH action. Both lower IGF-1. Different points of attack.
Break it down: If the question says "IGF-1 is still elevated after surgery and octreotide," the answer is pegvisomant.
Last Resort
Radiation Therapy
Slowly destroys remaining tumor cells. Takes years. Hypopituitarism risk.
Radiation works by killing adenoma cells, but GH and IGF-1 drop very slowly over years (sometimes a decade). During that time you still need medical therapy.
The big risk: Hypopituitarism. Radiation isn't precise enough to spare the rest of the pituitary. Patients often need replacement therapy for thyroid, cortisol, and sex hormones afterward.
Stereotactic radiosurgery (Gamma Knife) is more precise and has a slightly better profile, but still carries hypopituitarism risk.
💥Treatment order to memorize: Surgery (cure) → Octreotide (suppress GH release) → Pegvisomant (block GH receptors) → Radiation (last, slow, risky). The clinical medicine love asking which drug to add when surgery didn't fully work.
GAME TIME
Eliminate the Imposters
One tall teenager. Four possible diagnoses. Clues will eliminate them one by one. You click who's out.
A 15-year-old is brought in for "just growing too fast." You have four working diagnoses. Each clue eliminates one. Click the card you think the clue rules out. Be wrong and you'll hear about it.
Familial Tall Stature
Both parents are tall
Marfan Syndrome
Fibrillin-1 mutation
Precocious Puberty
Early sex hormone surge
Gigantism (GH Excess)
Pituitary adenoma
Loading first clue...
PROVE IT
Clinical Vignettes
Six patients walk in. All of them are about to test you. Don't let them win.
clinical Walkthrough
clinical Walkthrough
Original clinical vignettes. Shuffled, never-repeat, full explanations for every choice.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 5, 2026 at 8:04 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.