The pump is broken. But HOW it's broken changes everything you do about it. HFrEF vs HFpEF, NYHA staging, the GDMT algorithm clinical medicine loves, and when a patient's "shortness of breath" means five different things.
Opening Quiz
A 68-year-old man with HTN and diabetes presents with progressive dyspnea, bilateral crackles, and JVD. Echo shows EF 30%. Quick · which type of heart failure is this?
Yes. EF 30% = the pump is weak. That's HFrEF · heart failure with reduced ejection fraction. The cutoff is EF ≤ 40%. This is the type with the most proven drug therapies.
Not quite. EF 30% is the giveaway · that's way below normal (55-70%). When the EF is ≤ 40%, the ventricle can't squeeze hard enough. That's HFrEF (systolic failure). HFpEF would have a preserved EF ≥ 50% · the pump squeezes fine but can't relax.
↓ scroll to begin ↓
CLINICAL IMAGES
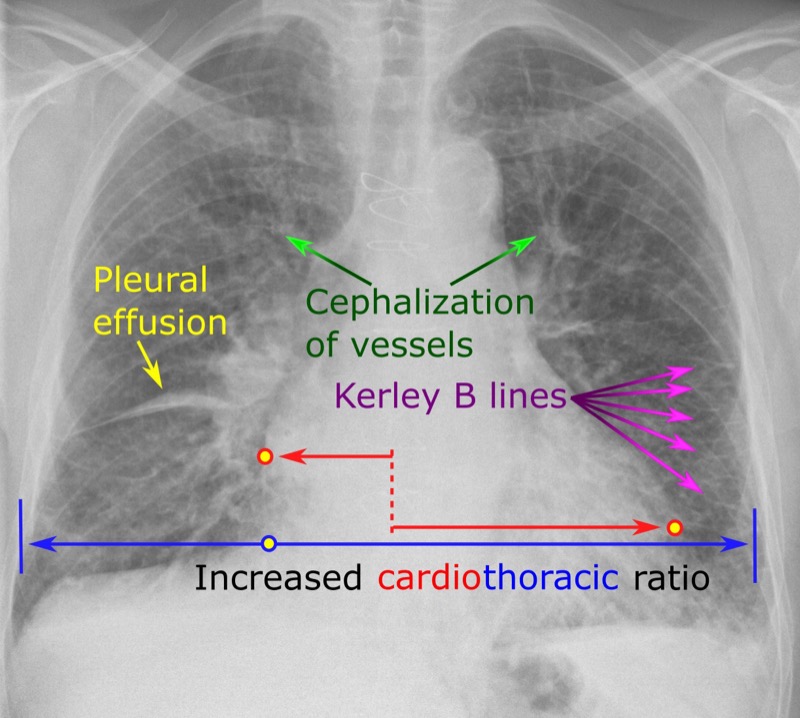
📷 CHF chest X-ray · cardiomegaly
1
First · What Broke?
Heart failure isn't one disease. It's a syndrome with two fundamentally different mechanisms. clinical questions ALWAYS give you the EF and expect you to know what follows from it.
The heart can fail in two ways:
HFrEF (Systolic)
HFpEF (Diastolic)
The Problem
Weak squeeze · ventricle dilates, can't pump enough out
Stiff wall · ventricle can't relax, can't fill properly
Fewer proven options · treat the underlying cause + SGLT2i
S3 Gallop
S3 · blood sloshing into a floppy ventricle
S4 · atria pushing against a stiff wall
💡There's also HFmrEF (EF 41-49%) · the "gray zone." clinical medicine rarely tests it directly, but treatment generally follows HFrEF guidelines. Think of it as HFrEF's less committed sibling.
🔑rEF = reduced squeeze. pEF = preserved squeeze but can't pull blood in.
Split-Screen Compare · Tap a Side to Light It Up
Two failures, same syndrome. Tap each ventricle to reveal how its profile differs.
HFrEF
Reduced EF · systolic failure
Ejection fraction40% or less
GeometryDilated, eccentric, thin
Heart soundS3 gallop
DefectWeak contraction
Classic patientPost-MI, dilated CMP
Drugs that save livesAll four pillars
HFpEF
Preserved EF · diastolic failure
Ejection fraction50% or more
GeometryConcentric, thick, stiff
Heart soundS4 gallop
DefectImpaired relaxation/filling
Classic patientElderly, HTN, diabetes, obese
Drugs that save livesSGLT2 inhibitor
⚡HFmrEF (EF 41 to 49%) is the bridge between the two. Modern guidance treats it like HFrEF, so when the EF lands in that gray band, reach for the four pillars.
Failure Archetypes
Four presentations clinical medicine throws at you. Each card pairs bedside clues with the mechanism and treatment move.
SYSTOLIC
💔
HFrEF
Heart failure with reduced EF
EF≤ 40%
ProblemWeak squeeze, dilated LV
SoundS3 gallop
Classic causePost-MI, dilated CMP
4 GDMT pillars all work here
core cue
HFrEF: Core Cues
Why EF drops
Myocyte loss (MI, myocarditis, alcohol, peripartum) or chronic pressure/volume overload → eccentric remodeling → dilated, thin-walled LV that can't generate enough pressure to push blood out.
The 4 pillars
ARNI (sacubitril/valsartan), beta-blocker (carvedilol, metoprolol succinate, bisoprolol), MRA (spironolactone), SGLT2i (dapagliflozin or empagliflozin). All have mortality benefit.
Device threshold
EF ≤35% after 3+ months GDMT → ICD. Add CRT if LBBB + QRS ≥150ms.
Board trap
Never uptitrate beta-blockers during acute decompensation. Metoprolol TARTRATE has no HFrEF mortality data. Only succinate.
DIASTOLIC
🥟
HFpEF
Heart failure with preserved EF
EF≥ 50%
ProblemStiff wall, can't relax/fill
SoundS4 gallop
Classic causeElderly woman, HTN, obesity
SGLT2i is the one drug with clear benefit
core cue
HFpEF: Core Cues
Why EF stays normal
The ventricle squeezes fine. The problem is relaxation (diastolic dysfunction). Long-standing HTN → LVH → stiff, non-compliant walls. Blood can't fill properly → low stroke volume despite preserved ejection.
Treatment (limited)
Empagliflozin (EMPEROR-Preserved). Diuretics for volume (careful: preload-sensitive). BP control. Rate control if AFib. Weight loss if obese. ARNI/BB/MRA lack proven mortality benefit here.
Diagnosis clue
Classic clinical medicine patient: 70s woman, obese, diabetic, HTN x20 years, exertional dyspnea, EF 58%, grade II diastolic dysfunction on echo. BNP mildly elevated.
Board trap
Don't give HFrEF drugs and expect HFpEF outcomes. Only SGLT2i crosses over reliably. Give the drug class that works, not the class that sounds right.
RIGHT-SIDED
🌊
Right HF
RV can't pump to lungs
Blood backs intoSystemic veins
SignsJVD, edema, hepatomegaly
LungsCLEAR
Most common causeLeft heart failure
Clear lungs + JVD + edema = right side
core cue
Right HF: Core Cues
Trace It
RV fails → blood backs up into systemic veins → increased venous pressure → JVD, peripheral pitting edema, ascites, hepatic congestion. No fluid in the lungs because the problem is BEFORE the lungs (right side doesn't pump there).
Inferior MI (RCA) + hypotension + clear lungs + JVD → suspect RV infarct. Check right-sided V4R lead for ST elevation. NO nitrates or diuretics (preload-dependent RV will crash). Give fluids instead.
Kussmaul sign
JVD that increases with inspiration (opposite of normal). Seen in RV infarct, constrictive pericarditis, tamponade. Classic clinical medicine physical exam finding.
COR PULMONALE
💨
Cor Pulmonale
Right HF from lung disease
CauseCOPD, pulmonary HTN, PE
Trace ItHigh pulm. pressure → RV fails
EKGRAD, P pulmonale, RVH
LungsAbnormal (the cause)
COPD + JVD = cor pulmonale until proven otherwise
core cue
Cor Pulmonale: Core Cues
Trace It
Chronic hypoxia or lung destruction → pulmonary vasoconstriction → elevated pulmonary vascular resistance → RV hypertrophy → RV dilation and failure. The lungs are killing the right heart.
EKG findings
Right axis deviation, P pulmonale (peaked P >2.5mm in II), RVH (tall R in V1). Also: low voltage in limb leads from hyperinflated lung tissue between heart and electrode.
Treatment
Treat the underlying lung disease. O2 therapy (reduces hypoxic vasoconstriction). Diuretics for volume. Avoid agents that drop pulmonary BP too fast. Heart transplant alone won't fix it if lungs are still the problem.
vs Primary Pulm HTN
Cor pulmonale = secondary to known lung/vascular disease. Primary (idiopathic) pulmonary HTN = no underlying cause. Young women. Treated with endothelin antagonists (bosentan), PDE-5 inhibitors (sildenafil), prostacyclins.
2
NYHA Classification · How Bad Is It?
clinical medicine gives you a patient and expects you to classify them. NYHA is functional · it's about what they can do, not what the echo shows.
I
No symptoms
II
Symptoms with ordinary activity
III
Symptoms with less-than-ordinary activity
IV
Symptoms at rest
Class I: Heart failure exists on echo, but the patient is living normally. They climb stairs, exercise, carry groceries. No shortness of breath beyond what's expected. Board question: "Asymptomatic patient found to have EF 35% on screening echo."
These patients STILL need GDMTGuideline-Directed Medical Therapy · the 4-pillar drug regimen for HFrEF. These drugs have mortality benefit, so you start them even when the patient feels fine. Waiting for symptoms means missing the window to prevent remodeling.. Just because they feel fine doesn't mean the ventricle isn't remodeling.
Class II: "I get winded walking up a flight of stairs" or "I can't keep up with my grandkids anymore." Ordinary activities cause symptoms. They're comfortable at rest. This is where most HF patients live in clinical practice.
Treatment: Full GDMT. Consider cardiac rehab. The goal is keeping them HERE and not letting them progress.
Class III: "I get short of breath walking to the bathroom." Less-than-ordinary activity triggers symptoms. They're limited but still comfortable sitting. Getting dressed is an effort.
Treatment: optimize GDMT first. Device check: EF <= 35% after 3+ months GDMT -> evaluate for ICD. Dyssynchrony check: LBBB with QRS >= 150 ms -> evaluate for CRT.
Class IV:Symptomatic at rest. Can't get out of bed without dyspnea. These patients are in and out of the hospital. This is end-stage.
Treatment: IV inotropes for low-output support. Escalation: LVAD or transplant evaluation. Disposition: advanced HF center referral.
Board Trap
NYHA class and ACC/AHA stage are different systems. NYHA fluctuates (patient can improve from III to II with treatment). ACC/AHA stages (A-D) only go forward · once you're Stage C, you never go back to B. clinical medicine loves asking which classification system allows regression. Answer: NYHA.
3
The Clinical Picture · Left vs Right
Heart failure symptoms depend on WHICH side failed. Blood backs up behind the broken pump.
A patient has bilateral pitting edema, JVD, and hepatomegaly but clear lungs. Which side failed?
Right. Clear lungs + peripheral edema + JVD + liver congestion = the right side can't pump blood forward into the lungs, so it backs up into the systemic venous system. Think: everything BEHIND the right heart · veins, liver, legs.
Good instinct, but left heart failure backs up into the lungs (crackles, dyspnea, orthopnea). This patient has clear lungs but peripheral congestion · that's the right side failing. Blood backs up behind whichever pump is broken.
Left Heart Failure
Right Heart Failure
Blood backs into
Pulmonary veins → lungs
Systemic veins → body
Dyspnea
Yes · exertional, orthopnea, PND
Usually only if biventricular
Crackles
Bilateral basilar crackles (fluid in alveoli)
Clear lungs
Edema
Pulmonary edema
Peripheral pitting edema, ascites
JVD
Only if right side also fails
JVD + hepatojugular reflux
Liver
Usually spared
Hepatomegaly, "nutmeg liver," elevated LFTs
S3/S4
S3 (HFrEF) or S4 (HFpEF)
Right-sided S3 (louder with inspiration)
Most Common Cause of Right HF
Left heart failure. It's almost always secondary. Increased pulmonary pressures from LHF → RV has to pump against higher resistance → RV fails.
💡OrthopneaDyspnea when lying flat. Gravity redistributes blood from legs to lungs. With a failing left ventricle, that extra preload overwhelms the pump → pulmonary congestion → "I need 3 pillows to sleep." The number of pillows IS the severity. = left side. PNDParoxysmal Nocturnal Dyspnea · waking up 1-2 hours after falling asleep, gasping for air. Same mechanism as orthopnea but delayed · interstitial fluid slowly redistributes back into the vascular space while supine. Classic board buzzword for left HF. = left side. JVD alone = right side. Both = biventricular (the most common presentation by the time patients reach the hospital).
🔑Left = Lungs. Right = the Rest of the body.
4
How You Diagnose It
Two things confirm heart failure: the clinical picture + objective evidence. clinical medicine always gives you labs and imaging and expects you to know what to order and what it means.
Test
What It Tells You
Board Pearl
BNP / NT-proBNPBrain Natriuretic Peptide · released by ventricular myocytes when they're stretched (volume overload). Elevated BNP (>100 pg/mL) or NT-proBNP (>300 pg/mL) strongly suggests heart failure. Used to differentiate cardiac from pulmonary causes of dyspnea. Falls with treatment → good prognostic marker.
Confirms volume overload / wall stress
Best initial test to distinguish HF from other causes of dyspnea. Normal BNP essentially rules OUT HF.
Echocardiogram
EF, wall motion, valves, chamber size, diastolic function
Most important test · this is what classifies HFrEF vs HFpEF. clinical medicine always gives you the EF.
CXR
Cardiomegaly, pulmonary congestion, effusions
Look for cephalization (upper lobe pulmonary veins distended), Kerley B lines, pleural effusions
EKG
Rhythm, ischemia, LVH, conduction disease
Wide QRS (esp LBBB) → consider CRT. Old Q waves → ischemic cardiomyopathy. A-fib → rate control critical
Board Trap
BNP can be falsely LOW in obesity. Fat tissue has natriuretic peptide clearance receptors. An obese patient with real HF might have a "borderline" BNP. If the clinical picture screams HF, don't let a normal-ish BNP in an obese patient fool you · get the echo.
Board Trap
BNP is elevated by ARNI (sacubitril/valsartan) because sacubitril inhibits neprilysin, which normally degrades BNP. So BNP goes UP on treatment even as the patient gets BETTER. Use NT-proBNP (not affected by neprilysin) to track patients on ARNI.
5
The GDMT Algorithm · HFrEF Treatment
This is the most testable part of heart failure. HFrEF has four pillars of therapy · all with mortality benefit. clinical medicine expects you to know all four, when to start them, and what to watch for.
Which of these is NOT one of the four pillars of GDMT for HFrEF?
Digoxin reduces symptoms and hospitalizations but has no mortality benefit. The four pillars that actually keep people alive: ARNI (or ACEi/ARB), beta-blocker, MRA, SGLT2i. Digoxin is a reasonable add-on for persistent symptoms but it's not GDMT.
That IS one of the four pillars. Digoxin is the odd one out · it's the classic trap. Digoxin improves symptoms and reduces hospitalizations, but it does NOT reduce mortality. The four mortality-reducing pillars are: ARNI, beta-blocker, MRA, and SGLT2i.
The Four Pillars of HFrEF (EF ≤ 40%)
Pillar 1 · RAAS Inhibition
ARNIAngiotensin Receptor-Neprilysin Inhibitor · sacubitril/valsartan (Entresto). Sacubitril blocks neprilysin → increases natriuretic peptides → vasodilation + diuresis + reduced fibrosis. Valsartan blocks AT1 receptors. PARADIGM-HF showed 20% mortality reduction vs enalapril. Must wash out ACEi for 36 hours before starting (risk of angioedema). (sacubitril/valsartan) preferred over ACEi/ARB
Reduces mortality 20% vs ACEi alone (PARADIGM-HF). If can't afford ARNI → use ACEi. If cough on ACEi → use ARB. Never combine ACEi + ARB.
Pillar 2 · Beta-Blocker
Carvedilol, metoprolol succinate, or bisoprolol · only these three
Reduces mortality ~35%. Blocks sympathetic overdrive that's remodeling the ventricle. Start LOW, titrate SLOW. Only these three have HF mortality data · metoprolol tartrate doesn't count.
Pillar 3 · MRA
SpironolactoneMineralocorticoid Receptor Antagonist · blocks aldosterone → reduces sodium retention, fibrosis, and potassium wasting. RALES trial showed 30% mortality reduction in severe HF. Watch for hyperkalemia (especially with ACEi/ARB) and gynecomastia (use eplerenone instead if this happens). or eplerenone
30% mortality reduction (RALES). Blocks aldosterone-driven fibrosis. Watch K+ · these patients are already on ACEi/ARB. Contraindicated if K+ > 5.0 or CrCl < 30.
Pillar 4 · SGLT2 Inhibitor
Dapagliflozin or empagliflozinOriginally diabetes drugs. DAPA-HF and EMPEROR-Reduced showed mortality + hospitalization benefit in HFrEF regardless of diabetes status. Mechanism in HF is still being clarified · likely involves osmotic diuresis, reduced preload, improved cardiac energetics, and anti-fibrotic effects. One of the biggest cardiology breakthroughs of the decade.
Works even WITHOUT diabetes. Reduces HF hospitalization and CV death. Newest pillar · added after DAPA-HF and EMPEROR-Reduced trials. This is the one most commonly missed on newer exams.
Build the Regimen · Tap Each Pillar
Each pillar you add to a 40%-or-less EF patient stacks more mortality protection. Watch the bar fill as you assemble the guideline-directed regimen.
✓
ARNI (sacubitril/valsartan)
Preferred over ACEi/ARB. Block neprilysin, boost natriuretic peptides, drop afterload. If unavailable, an ACEi or ARB still counts as this pillar. Never stack all three.
✓
Beta-blocker
Carvedilol, metoprolol succinate, or bisoprolol only. Blunts the sympathetic overdrive that remodels the ventricle. Start low, go slow.
✓
MRA (spironolactone or eplerenone)
Blocks aldosterone-driven fibrosis. Watch potassium 5.0 mEq/L (3.5 to 5.0) and creatinine, since these patients also sit on RAAS blockade.
✓
SGLT2 inhibitor (dapagliflozin/empagliflozin)
The newest pillar. Cuts hospitalizations and cardiovascular death even without diabetes. The choice most often missed on current exams.
0 of 4 pillars · start building.
Additional Therapies (not pillars, but testable)
Symptom Relief
Loop diuretics (furosemide, bumetanide) · for congestion
No mortality benefit. Pure symptom relief. "Dry" the patient out when they're volume-overloaded. Adjust dose to euvolemia.
Hydralazine + Nitrate
Hydralazine + isosorbide dinitrate
Mortality benefit specifically in Black patients with NYHA III-IV already on standard GDMT (A-HeFT trial). Also used when patient can't tolerate ACEi/ARB (renal failure, hyperkalemia).
Ivabradine
Ivabradine (Corlanor)
For patients on max beta-blocker who still have HR ≥ 70 in sinus rhythm. Blocks the funny (If) current in the SA node. Only works in sinus · useless in a-fib.
Devices
ICD if EF ≤ 35% on 3+ months of optimal GDMT. CRT if EF ≤ 35% + LBBB + QRS ≥ 150ms.
ICD prevents sudden cardiac death. CRT resynchronizes a dyssynchronous squeeze · actual mortality benefit when indicated.
End-Stage (NYHA IV)
LVAD (bridge or destination), heart transplant, inotropes (milrinone, dobutamine)
When drugs and devices aren't enough. Inotropes improve symptoms but may worsen mortality · they're for comfort or bridge to transplant.
Board Trap
Beta-blockers are contraindicated in acute decompensated HF. Don't start or uptitrate during an acute exacerbation · the patient needs their sympathetic drive right now. Start or resume once they're stable and euvolemic. Board question: patient admitted with acute HF, already on metoprolol → hold, don't increase.
Board Trap
Metoprolol succinate (extended-release) has HF mortality data. Metoprolol tartrate (immediate-release) does NOT. Same drug, different formulation, different evidence. clinical medicine will specify. If they say "metoprolol" without specifying, the context matters.
6
HFpEF · The One With Fewer Answers
HFpEF is frustrating because most HFrEF drugs don't work here. The ventricle squeezes fine · it just can't relax. Different problem, different approach.
Strategy
Details
SGLT2 inhibitor
The ONE drug class with clear benefit in HFpEF (EMPEROR-Preserved). Empagliflozin reduced HF hospitalizations. This is the answer on modern clinical practice.
Diuretics
For volume management. These patients are preload-sensitive · too much diuresis drops their filling and they crash.
BP control
Most HFpEF is from long-standing HTN → LVH → diastolic dysfunction. Controlling the cause prevents progression.
Rate control
A-fib is extremely common in HFpEF. Fast rates shorten diastole → less filling time → worse symptoms.
Weight loss
Obesity is a major driver. Even modest weight loss improves symptoms and functional capacity.
💡The simplest board answer for HFpEF: SGLT2i + treat the underlying cause + diuretics for symptoms. If they give you an HFpEF patient and ask "what medication?", SGLT2i is the answer (unless there's a contraindication).
7
Acute Decompensated HF · The ER Scenario
Patient arrives to the ED with severe dyspnea, bilateral crackles, SpO2 88%, BNP 1200. They're "wet and cold" or "wet and warm." This is the acute management question.
What's the FIRST thing you give this patient?
IV loop diuretics are first-line for acute decompensated HF. The patient is drowning in their own fluid · dry them out FIRST. Decongestion is the immediate priority. GDMT optimization happens later, when they're stable.
This patient is acutely decompensated · they need decongestion NOW. IV furosemide is first-line. The GDMT drugs (ARNI, beta-blocker) are for chronic management after stabilization. Beta-blockers can actually make acute decompensation WORSE. Get the fluid off first.
The Warm/Cold × Wet/Dry Matrix
This is how you triage acute HF. Two questions: Is the patient congested (wet)? Is the patient perfusing (warm)?
💡Warm & Wet is the bread-and-butter HF admission. IV furosemide, supplemental O2, monitor I/Os, optimize GDMT once stable. Cold & Wet is the scary one · you need something to squeeze the heart harder (dobutamine, milrinone) while also decongesting.
Board Trap
Nesiritide (IV BNP) used to be given for acute HF. It fell out of favor · no mortality benefit and possible renal harm. If clinical medicine offers it as an answer, it's almost always the wrong choice. IV diuretics are first-line.
8
Decision Tree · What Do I Do?
clinical medicine gives you an HF patient. Work through this algorithm to get the answer.
Answer each node before the next branch unlocks.
A 64-year-old man arrives at the emergency department with crushing dyspnea, SpO2 84% on room air, bibasilar crackles to the scapulae, JVP to the jaw, and a third heart sound. Blood pressure is 148/92 mmHg, extremities warm. What is the first move?
He is decongested and euvolemic three days later. Echo confirms EF 28% with a dilated, thin-walled left ventricle. Resting heart rate is 62/min in sinus, QRS 96 ms (normal less than 120). What now anchors his long-term therapy?
Step 1: Is this acute or chronic?
Acute HF · Is the patient congested (wet)?
Wet patient · Is perfusion adequate (warm vs cold)?
Dry but symptomatic · What's the likely issue?
Reassess the diagnosis. If truly dry + warm → adjust oral meds, this may not need admission. If dry + cold → consider cardiogenic shock with intravascular depletion. Gentle volume challenge + consider inotropes. Get a right heart cath if diagnosis is unclear.
Chronic HF · What's the EF?
HFrEF · Start all four pillars of GDMT:
1. ARNI (or ACEi → ARB if intolerant) 2. Beta-blocker (carvedilol, metoprolol succinate, or bisoprolol) 3. MRA (spironolactone or eplerenone) · watch K+ 4. SGLT2i (dapagliflozin or empagliflozin) + Loop diuretic PRN for congestion (no mortality benefit)
If still EF ≤35% after 3+ months GDMT → ICD.
If LBBB + QRS ≥150ms → CRT.
If Black + NYHA III-IV → add hydralazine/nitrate.
If sinus + HR ≥70 on max BB → add ivabradine.
HFpEF · Fewer proven therapies:
1. SGLT2i (empagliflozin · EMPEROR-Preserved) 2. Diuretics for volume (careful · these patients are preload-sensitive) 3. BP control (target <130/80) 4. Rate control if A-fib 5. Weight loss if obese
The big four GDMT pillars (ARNI, BB, MRA) have NOT shown mortality benefit in pure HFpEF. SGLT2i is the breakthrough here.
9
Elimination Game · Name That Failure
Four patients walk in. Each clue eliminates one diagnosis. Click the one that DOESN'T fit each clue.
HFrEF
Weak pump, EF 25%
HFpEF
Stiff wall, EF 60%
Cor Pulmonale
RV failure from lung disease
Tamponade
Fluid compressing the heart
Loading clue...
Round 2 · Four more diagnoses. Same drill.
Dilated CMP
Big floppy ventricle
HCM
Thick septum, obstruction
Restrictive CMP
Stiff walls, can't fill
Takotsubo
Stress-induced, apical ballooning
Loading clue...
10
Quiz · Don't Kill Them
Six patients just showed up to your cardiology clinic. Let's see if you were paying attention.
clinical Walkthrough
clinical Walkthrough
Original clinical vignettes. Shuffled, never-repeat until the bank exhausts. Right-click or long-press to cross out. Double-click or double-tap to highlight. Answer to make the clues glow.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 12, 2026 at 11:55 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.