A 67-year-old man with hypertension and type 2 diabetes is brought in by ambulance. He says his chest has felt "like someone's sitting on it" for the past 90 minutes. His BP is 88/60 and he's diaphoretic and pale. EKG shows ST elevations in leads II, III, and aVF with ST depression in I and aVL. What is the most likely culprit artery?
Tap any segment to learn what it means
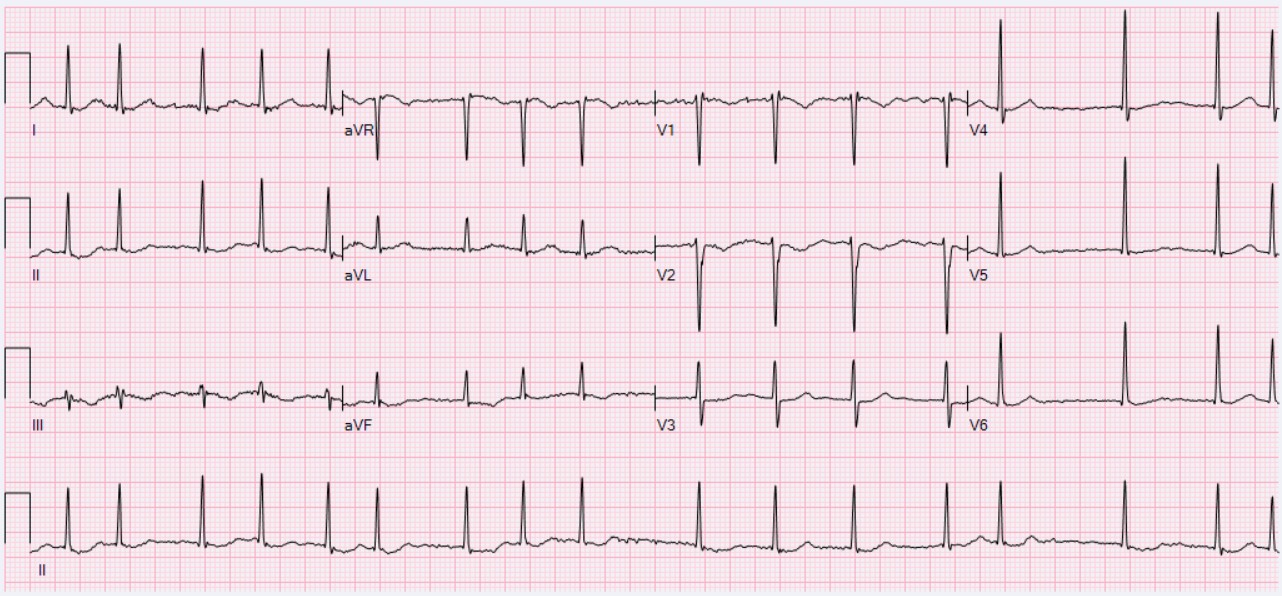
📷 NORMAL SINUS RHYTHM · open image
Tap a segment above
Select a waveform segment
Each segment of the EKG tells a specific electrical story. Tap the P wave, QRS, ST segment, T wave, or intervals to see what is normal and what goes wrong.
How to Read Paper Speed
📏
Standard paper runs at 25 mm/sec. Each small box = 0.04s. Each large box (5 small) = 0.2s. One full EKG strip = 10 seconds. This math is on every single interval question.
🔋
Voltage: Each small box = 0.1 mV vertically. Each large box = 0.5 mV. A QRS that is 10 small boxes tall = 1 mV. LVH and RVH criteria use this.
Lead Geography; What Each Lead Sees
Territory
Leads
Culprit Artery
Inferior
II, III, aVF
RCA (80%), LCx (20%)
Anterior
V1-V4
LAD
Lateral
I, aVL, V5-V6
LCx / LAD diagonal
Posterior
V1-V2 (reciprocal)
RCA / LCx
Septal
V1-V2
LAD (septal perforators)
Memory: I, II, III point like a clock face. II sits at the bottom. The inferior leads look UP from the feet of the patient; they see the bottom of the heart.
Calculating Rate; The 300 Method
Find an R wave on a thick line. Count the thick lines to the next R wave: 300, 150, 100, 75, 60, 50. That is your rate. If the rhythm is irregular, count all QRS complexes in 10 seconds and multiply by 6.
💡
Mnemonic: "300 Mexicans Ate Hot Burritos Sadly" = 300, 150, 100, 75, 60, 50. Yes it is weird. No you will not forget it.
Systematic Rhythm Assessment
1️⃣
Regular or irregular? March out the R waves. Regular = NSR candidate. Irregular = think AFib, MAT, or PACs.
2️⃣
P waves present? No P waves = AFib or junctional. P before every QRS = organized atrial activity.
3️⃣
P-QRS relationship? Is there a P for every QRS and a QRS for every P? If not, think AV block.
4️⃣
QRS narrow or wide? Less than 3 small boxes (0.12s) = narrow = supraventricular. Greater than 3 = wide = bundle branch, aberrant, or ventricular.
The Major Rhythms at a Glance
📷 ATRIAL FIBRILLATION · open image
Rhythm
Rate
P waves
QRS
NSR
60-100
Upright in II
Narrow
AFib
Usually fast
None (fibrillatory baseline)
Narrow, irregular
AFlutter
150 (2:1 block)
Sawtooth at 300
Narrow
VTach
100-250
Dissociated
Wide, regular
VFib
Chaotic
None
Chaotic
SVT
150-250
Buried in T wave
Narrow, regular
Junctional
40-60
Retrograde/absent
Narrow
Board Trap
Atrial flutter almost always presents at heart rate 150. Why? The atria fire at 300 bpm and the AV node blocks every other beat (2:1 block). If you see a narrow complex tachycardia at exactly 150, look hard for sawtooth flutter waves; they can hide in the QRS or T wave. Cardiovert it like AFib.
Rhythm Battle Cards
SUPRAVENTRICULAR
🌞
Atrial Fibrillation
Irregularly irregular
RateVariable (usually fast)
P wavesNone; fibrillatory baseline
QRSNarrow, chaotically irregular
No two RR intervals are the same
core cue
AFib: Core Cues
Trace It
Multiple chaotic reentry circuits in atria. No organized atrial contraction. AV node fires when it wants.
Atrial clots form in the LAA. Stroke risk. CHADS-VASC score drives anticoagulation decision.
Treatment
Rate control (beta-blocker, CCB) vs. rhythm control (cardioversion). Anticoag if >48h or unknown onset.
SUPRAVENTRICULAR
🐇
Atrial Flutter
Regularly irregular
RateAtria 300, ventricles 150 (2:1)
P wavesSawtooth at 300 bpm in II, III, aVF
QRSNarrow, regular (or regularly irregular)
HR exactly 150 = flutter until proven otherwise
core cue
AFlutter: Core Cues
Trace It
Single large reentry circuit in RA (cavotricuspid isthmus). Organized but too fast. AV node protects by blocking in ratio (2:1, 3:1, 4:1).
The Trap
Flutter waves hide in QRS or T wave. Carotid sinus massage slows AV conduction temporarily and uncovers them.
Treatment
Same anticoag rules as AFib. Rate control. Ablation is curative (95% success at isthmus).
VENTRICULAR
⚡
Ventricular Tachycardia
Wide complex emergency
Rate100-250 bpm
P wavesAV dissociation (cannon A waves)
QRSWide (>0.12s), monomorphic or poly
Wide complex + fast + hemodynamic instability = VTach until proven otherwise
core cue
VTach: Core Cues
Trace It
Reentry circuit in ventricular scar (post-MI most common). Both ventricles not contracting in sync; cardiac output tanks.
Brugada Criteria
RS absent in precordial leads, RS interval >100ms, AV dissociation, morphology criteria. Any one = VTach.
Treatment
Unstable: synchronized cardioversion immediately. Stable: amiodarone or procainamide. Verapamil can worsen hypotension in VTach.
SUPRAVENTRICULAR
🔥
SVT (AVNRT)
Paroxysmal narrow complex
Rate150-250 bpm
P wavesBuried in T wave or retrograde
QRSNarrow, regular, abrupt onset/offset
Abrupt "flip switch" start/stop in a young healthy person
core cue
SVT: Core Cues
Trace It
Dual pathway reentry in the AV node (AVNRT). Fast and slow pathways create a loop. Triggered by a PAC hitting the fast path when it's refractory.
Termination
Vagal maneuvers (Valsalva, carotid sinus massage) first. Adenosine 6mg IV if vagal fails; briefly blocks AV node and breaks the circuit.
Long-term
Ablation of slow pathway curative. Beta-blockers or CCBs for prevention if recurrent.
Axis; Which Direction Is the Heart Pointing?
The cardiac axis tells you the average direction of ventricular depolarization. Normal is between -30 and +90 degrees. Use Lead I and aVF together as a two-lead shortcut.
Two-Lead Shortcut
✅
Normal: Lead I positive + aVF positive = normal axis (roughly -30 to +90)
⬆
LAD: Lead I positive + aVF negative = left axis deviation. Think: LVH, LBBB, inferior MI, LAFB
➡
RAD: Lead I negative + aVF positive = right axis deviation. Think: RVH, RBBB, lateral MI, LPFB, tall thin people, dextrocardia
⚡
Extreme axis (NW axis): Both Lead I and aVF negative. Think: VTach, severe RVH, lead reversal
Cause
Axis
See It
LBBB
LAD
Wide QRS + LAD together
RBBB
Normal or RAD
rSR' in V1, wide S in I
LAFB
LAD
Narrow QRS, LAD alone
Inferior STEMI
LAD
Loss of inferior forces
RVH / PE
RAD
S1Q3T3 pattern in PE
Axis Identifier; Pick Your Leads
Tap Lead I then aVF to identify the axis.
LEAD I
aVF
Normal Intervals; Know These Cold
Interval
Normal Range
Measured How
PR interval
0.12 to 0.20s (3-5 small boxes)
Start of P to start of QRS
QRS duration
Under 0.12s (less than 3 boxes)
Start to end of QRS
QTc
Under 0.44s men, 0.46s women
QT corrected for rate
AV Blocks; The Three Flavors
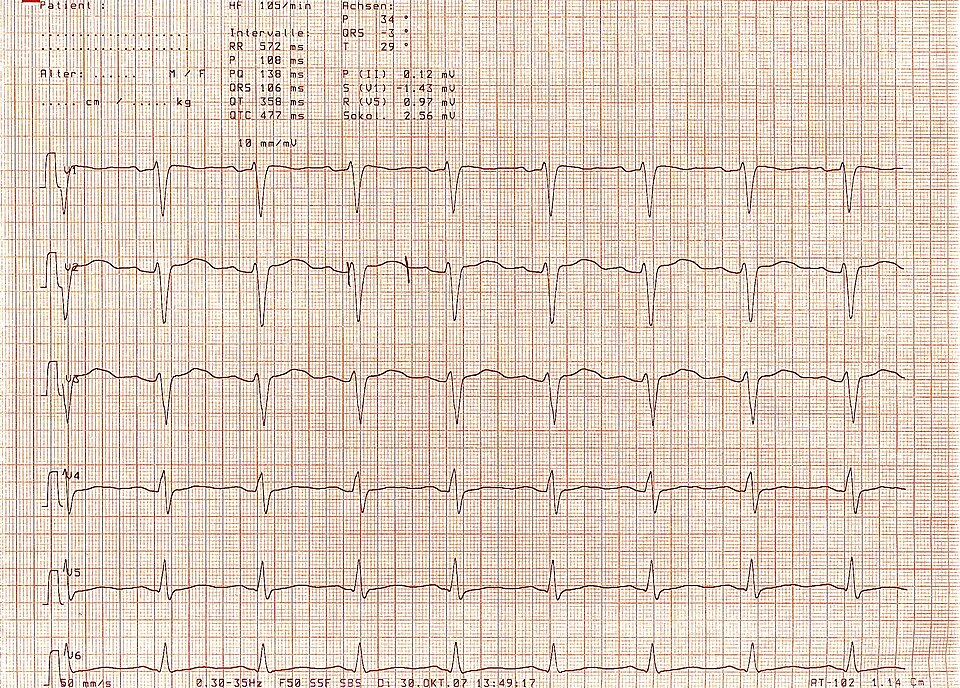
ECG: LONG QT · open image
1
First-degree: PR greater than 0.20s. Every P conducts. No treatment needed. "The bouncer is slow but everyone gets in."
2
Mobitz I (Wenckebach): PR progressively lengthens until a QRS is dropped. Then resets. Regularly irregular. Usually benign; observe. Inferior MI, athletic hearts, increased vagal tone.
2B
Mobitz II: Constant PR but sudden QRS drops without warning. Dangerous; can progress to complete block. Needs pacemaker. Associated with anterior MI and His-Purkinje disease.
3
Third-degree (complete): P waves and QRS march at completely different rates with no relationship. Escape rhythm keeps the patient alive. Pacemaker now.
Board Trap
Mobitz I vs Mobitz II matters enormously: Wenckebach (I) = observation. Mobitz II = pacemaker. The clinical medicine will try to make you confuse them. Key: in Mobitz I, the P-R interval GETS LONGER before the dropped beat. In Mobitz II, all conducted PR intervals are IDENTICAL; the drop comes out of nowhere.
Bundle Branch Blocks
⬅
LBBB: Wide QRS + broad notched R in I, aVL, V5-V6 ("William") + deep S in V1. Causes LAD. Invalidates STEMI criteria; any new LBBB with chest pain = cath lab.
➡
RBBB: Wide QRS + rSR' in V1 ("rabbit ears") + wide S in I, aVL, V5-V6 ("Marrow"). Can be normal variant. Does NOT invalidate STEMI.
🧠
WiLLiaM MaRRoW: LBBB = W in V1, M in V6. RBBB = M in V1, W in V6.
QT Prolongation; Drugs That Kill
Long QT is dangerous because it can degenerate into Torsades de Pointes (TdP); a polymorphic VTach that can become VFib. QTc greater than 500ms is a medical emergency.
Drug Class
Examples
Antiarrhythmics
Sotalol, amiodarone, quinidine, procainamide
Antibiotics
Azithromycin, fluoroquinolones
Antipsychotics
Haloperidol, quetiapine, ziprasidone
Antiemetics
Ondansetron, metoclopramide
Antifungals
Fluconazole
💊
TdP treatment: IV magnesium sulfate first. Then overdrive pacing or isoproterenol if needed. Stop the offending drug.
ST Elevation; STEMI vs Benign
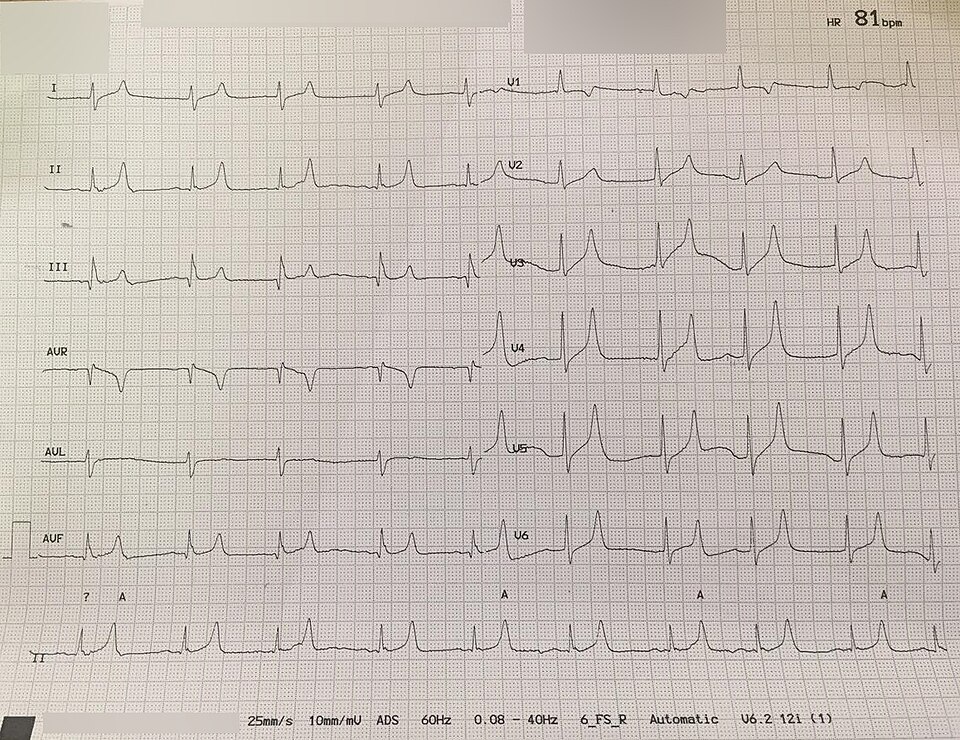
ECG: HYPERKALEMIA · peaked T waves · open image
Pattern
Shape
Key Clue
STEMI
Convex ("tombstone") or flat elevation
Reciprocal depression in opposite leads
Pericarditis
Concave ("saddle-shaped"), diffuse
PR depression, no reciprocal changes
Early repolarization
Concave, notch at J point
Young athletic person, V2-V5, benign
Brugada
Coved STE in V1-V2
Young man, syncope, especially at rest
LVH strain
Downsloping ST in V5-V6
Deep S in V1, tall R in V5-V6
STEMI Territories
❤
Inferior STEMI (II, III, aVF): RCA in 80%. Check right-sided leads (V4R) for RV involvement; if present, do NOT give nitrates or diuretics (preload-dependent).
⬆
Anterior STEMI (V1-V4): LAD. Worst prognosis. Can cause cardiogenic shock, new LBBB, papillary muscle rupture.
↙
Posterior STEMI: ST depression + tall R in V1-V2 + upright T. The posterior wall has no direct leads; you see it as a mirror image. Add V7-V9 (posterior leads) to confirm.
Board Trap
Wellens Syndrome: A patient with unstable angina and biphasic or deeply inverted T waves in V2-V3 when they are PAIN FREE. This means the LAD is critically stenosed and the patient is about to have a massive anterior STEMI. Do NOT stress test. Send urgently to cath lab.
T Wave Changes
🔺
Hyperacute T waves: Tall, peaked, symmetric T waves are the EARLIEST sign of STEMI; before ST elevation. Often missed.
🔻
T wave inversions: Ischemia, PE (V1-V4), Wellens, Takotsubo, increased ICP (deep symmetric inversions).
⚡
Peaked T waves with wide QRS: Think hyperkalemia first. Sine wave pattern = extreme hyperkalemia = cardiac arrest risk.
Prove It
Clinical Vignettes
Five questions. One shot each. Let's see what stuck.
out of 5
clinical Walkthrough
clinical Walkthrough
Original clinical vignettes. Shuffled, never-repeat, full explanations for every choice.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 13, 2026 at 12:48 AM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.