Born with a broken circuit. Left-to-right shunts cause volume overload. Right-to-left cause cyanosis. The physiology drives everything.
Opening Challenge
A 2-day-old infant has cyanosis that does NOT improve with supplemental oxygen.
The nurse places a pulse oximeter on both hands: right hand reads 98%, left hand reads 88%.
Chest X-ray reveals an "egg on a string" cardiac silhouette.
What is the most likely diagnosis?
Answer: B · TGA
The "egg on a string" (narrow mediastinum because the aorta sits directly anterior to the pulmonary artery, not side by side) is pathognomonic for TGA.
Differential cyanosis (right hand higher sat than feet/left hand) can occur when a PDA provides mixing, but the egg silhouette clinches TGA.
TOF has a boot-shaped heart.
No response to O2 means a structural shunt, not a pulmonary cause: oxygenated blood from the lungs cannot reach the systemic circulation in parallel circuit anatomy.
Defect Visual Anchors
Common defect overview
Parallel circuits in TGA
Ductus-dependent mixing
The Shunt Divide
Every congenital heart defect falls into one of two categories. The direction of the shunt determines your first move in any vignette.
L-to-R shunt forms (VSD, ASD, PDA, AVSD). Oxygenated blood re-enters the right side and floods the lungs.
Increased pulmonary blood flow causes endothelial remodeling and arterial wall thickening over years.
RV hypertrophy: right ventricle remodels against the elevated resistance.
Eisenmenger syndrome: pulmonary pressure exceeds systemic. Shunt reverses to R-to-L.
Late cyanosis + digital clubbing + polycythemia. Surgical repair now CONTRAINDICATED.
L-to-R Shunts
Acyanotic at birth. Cyanosis only if Eisenmenger develops later.
VSD (most common CHD overall): left lower sternal border, holosystolic murmur
ASD: fixed split S2, systolic ejection murmur at pulmonic area
PDA: continuous "machinery" murmur, left infraclavicular; wide pulse pressure
AVSD: ASD + VSD + common AV valve; strongly associated with Down syndrome
Left oxygenated blood spills into the right side. Lungs get extra volume. The baby is pink at birth. The murmur is what brings them in.
R-to-L Shunts
Cyanotic from birth. Deoxygenated blood bypasses the lungs.
TTTTTThe 5 T's
Tetralogy of Fallot: most common CYANOTIC CHD. Boot-shaped heart. Tet spells.
TGA: parallel circuits. Egg on a string. Day 1-2 of life.
Truncus arteriosus: single great vessel. Associated with 22q11 deletion.
Tricuspid atresia: no tricuspid valve; hypoplastic RV; left axis deviation on ECG.
TAPVR (Total anomalous pulmonary venous return): pulmonary veins drain to right side.
Hypoplastic left heart: duct-dependent systemic circulation. PGE1 is life.
Eisenmenger Syndrome
The point of no return.
Any large, unrepaired L-to-R shunt can trigger irreversible pulmonary vascular remodeling
Most common culprits: large VSD, large ASD, PDA
Once pulmonary pressure exceeds systemic: shunt reverses to R-to-L, cyanosis appears
Clubbing and polycythemia follow (polycythemia is compensatory, not to be treated aggressively)
Surgical repair CONTRAINDICATED: removing the shunt leaves the RV facing fixed high resistance it cannot overcome
Management: pulmonary vasodilators, lung transplant in select cases
🧪
The Hyperoxia Test: Give 100% O2. If cyanosis corrects, the cause is pulmonary (V/Q mismatch, pneumonia, RDS). If cyanosis persists, the cause is structural cardiac because the shunt routes deoxygenated blood directly into the systemic circulation, bypassing the alveoli entirely. This is your first move when a cyanotic neonate arrives.
L-to-R Shunts
Tap each card to flip and reveal the full clinical picture. Know the murmur, the associations, and the treatment approach for each.
Most Common CHD Overall
Ventricular Septal Defect (VSD)
Tap to reveal →
L-to-R
Murmur: Harsh holosystolic at left lower sternal border (3rd-4th ICS). Thrill may be palpable.
80% close spontaneously (especially small muscular VSDs). Large VSDs cause CHF, failure to thrive, recurrent pneumonias.
Location: Membranous VSD = 80% of cases. Muscular = remainder.
Eisenmenger risk if large and unrepaired.
Fixed Split S2
Atrial Septal Defect (ASD)
Tap to reveal →
L-to-R
Secundum ASD (fossa ovalis area) = most common type.
Fixed split S2: RA filling is equalized across respiration by the shunt, removing the normal respiratory variation.
Systolic ejection murmur at pulmonic area (high pulmonary flow, not across the defect itself).
Often asymptomatic until adulthood, then: fatigue, palpitations, paradoxical embolism/stroke.
Primum ASD = near AV valves, Down syndrome association.
Machinery Murmur
Patent Ductus Arteriosus (PDA)
Tap to reveal →
L-to-R
Ductus arteriosus = fetal shunt connecting aorta to pulmonary artery. Closes at birth as O2 rises and prostaglandins fall.
Murmur: Continuous "machinery" murmur, left infraclavicular. Present in both systole AND diastole.
Wide pulse pressure (blood runs back into pulmonary artery in diastole).
Treatment: Indomethacin (NSAID inhibits prostaglandins, closes duct). Common in preterm infants.
Keep open with PGE1 in duct-dependent lesions.
Down Syndrome Association
AV Septal Defect (AVSD)
Tap to reveal →
L-to-R
Anatomy: Primum ASD + VSD + single common AV valve (instead of separate mitral and tricuspid).
Strongly associated with Trisomy 21 (Down syndrome). If the vignette says Down syndrome + CHD, think AVSD first.
Complete AVSD presents with early CHF and failure to thrive; requires surgical repair by 3-6 months of age.
Partial AVSD may be asymptomatic longer.
R-to-L Shunts
These are the cyanotic lesions. Deoxygenated blood bypasses the lungs and reaches the systemic circulation directly. Tap each to expand the full breakdown.
Tetralogy of Fallot (TOF)
Most common CYANOTIC CHD
⌄
Four defects remembered with PROVe: Pulmonary stenosis (RVOT obstruction) + RVH + Overriding aorta + VSD.
Boot-shaped heart on CXR: RVH lifts and rotates the cardiac apex upward and to the left, with a concave pulmonary segment.
Tet spells (hypercyanotic episodes): dynamic RVOT obstruction worsens suddenly, more deoxygenated blood exits via overriding aorta. Triggered by crying, feeding, exertion, or agitation.
Squatting reflex: child instinctively squats to compress femoral arteries, increasing SVR, which pushes more blood through the stenotic RVOT into the lungs. Classic board clue.
Tet spell management: knee-chest position + morphine + IV fluids + propranolol (if persistent). Goal: increase SVR and reduce RVOT spasm.
Surgical repair required, typically before 6 months of age.
Transposition of the Great Arteries (TGA)
Day 1-2 of life, incompatible with life without mixing
⌄
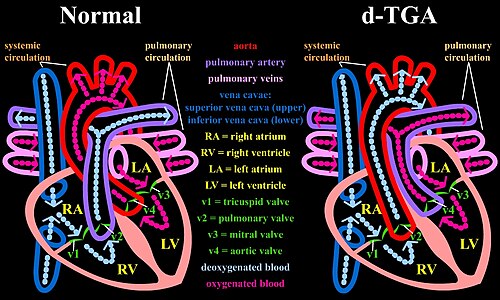
The aorta arises from the right ventricle; the pulmonary artery arises from the left ventricle. Two parallel, non-communicating circuits. Incompatible with life unless there is mixing via ASD, VSD, or PDA.
Egg on a string on CXR: aorta sits directly anterior to the pulmonary artery (not side-by-side), creating a narrow superior mediastinum that looks like an egg balanced on a string.
Cyanosis appears on Day 1-2, does NOT respond to O2.
Immediate treatment: PGE1 to keep PDA open + balloon atrial septostomy (Rashkind) for immediate mixing.
Definitive repair: Arterial switch operation (Jatene procedure) in the first 2 weeks of life. Aorta reconnected to LV, pulmonary artery to RV, coronary arteries reimplanted.
Truncus Arteriosus
Single great vessel from both ventricles
⌄
A single common arterial trunk arises from both ventricles instead of a separate aorta and pulmonary artery. The truncal valve overrides a large VSD.
Presents with early cyanosis AND early heart failure (because pulmonary blood flow is actually increased from the single trunk).
Associated with 22q11 deletion (DiGeorge/velocardiofacial syndrome).
Requires surgical repair: VSD closure, conduit from RV to pulmonary arteries.
Check calcium in any vignette mentioning DiGeorge: hypocalcemia from absent parathyroid glands causes tetany/seizures.
Tricuspid Atresia
Left axis deviation on ECG (rare for a cyanotic lesion)
⌄
Complete absence of the tricuspid valve. Blood from the RA cannot enter the RV. Survival requires an ASD (for RA emptying) and either VSD or PDA (for some pulmonary blood flow).
Hypoplastic RV: the right ventricle never develops normally because it receives no input from the RA.
Left axis deviation on ECG: this is the distinguishing feature. Most right-sided cyanotic lesions show right axis deviation from RV strain. Tricuspid atresia has a dominant LV, so the axis swings left.
Palliative surgery: Fontan procedure (connects systemic veins directly to pulmonary arteries, bypassing the heart entirely).
The Big Rules
These are the clinical rules that separate a correct answer from a trap. Know them cold.
⛔
Duct-Dependent Lesions: Give PGE1 Immediately.
Any CHD where the only path to perfuse the lungs (or the body) is through a PDA: prostaglandin E1 keeps the duct open. Do NOT let it close. Examples: pulmonary atresia, critical coarctation of the aorta, hypoplastic left heart syndrome, TGA. Closing the duct = death.
🧬
Down Syndrome (Trisomy 21) + CHD:
AVSD (most specific) > VSD > ASD. If the vignette has Trisomy 21 and a cardiac defect, go to AVSD first. Primum ASD (a component of AVSD) is also a common Down syndrome association.
⚡
22q11 Deletion (DiGeorge / Velocardiofacial Syndrome):
Truncus arteriosus and TOF are the two most common CHDs. The triad is: hypocalcemia (no parathyroid), T-cell deficiency (thymic aplasia), cleft palate, and conotruncal cardiac defects. Mnemonic: CATCH-22 (Cardiac, Abnormal facies, Thymic aplasia, Cleft palate, Hypocalcemia, chromosome 22).
Coarctation of the Aorta
Type
Location
Presentation
Initial Treatment
Infantile (Preductal)
Proximal to ductus arteriosus
Severe HF in first days of life. Duct-dependent lower body perfusion. Critical
PGE1 to maintain ductal flow, urgent surgical repair
Coarctation High-Yield Associations:
Bicuspid aortic valve (50% of coarctation cases) and Turner syndrome (45,X) are the two key associations. Radio-femoral delay on exam (radial pulse arrives before femoral pulse). Turner
⏹
Eisenmenger Timing Rule:
Once Eisenmenger syndrome is established, surgical repair is CONTRAINDICATED. Removing the shunt eliminates the RV's only "escape valve"; the RV suddenly faces the full fixed pulmonary vascular resistance with no way to decompress. Acute RV failure follows.
The Elimination Game
Use the clues to narrow down four candidates to one. Click each clue in order.
Clinical Vignette
A 3-month-old girl is found to have a continuous "washing machine" murmur heard best under the left clavicle. She was born at 28 weeks gestation. Physical exam reveals a wide pulse pressure. Echocardiogram confirms persistent communication between the aorta and pulmonary artery.
Which defect explains this presentation?
VSD
ASD
PDA
Coarctation
A continuous murmur persists across the entire cardiac cycle. VSD produces a holosystolic (systolic only) murmur because the pressure gradient reverses in diastole. ASD produces a systolic ejection murmur from increased pulmonary flow, not a shunt murmur across the defect itself. Coarctation produces a systolic murmur or is silent.
Eliminated: VSD, ASD, Coarctation
Prostaglandins keep the ductus arteriosus open in the fetus. In premature infants, the duct is especially likely to remain patent because prostaglandin synthesis is still active and the duct is less responsive to the postnatal oxygen signal. Indomethacin (an NSAID) inhibits prostaglandin synthesis, causing the duct to constrict and close. Murmur disappears because the structural communication is gone.
Confirmed: PDA
Verdict: Patent Ductus Arteriosus (PDA)
Continuous machinery murmur + premature infant + wide pulse pressure + aorta-to-pulmonary artery communication + indomethacin closure = PDA. The ductus arteriosus connects the descending aorta to the pulmonary trunk just distal to the left subclavian artery, explaining why the murmur is loudest at the left infraclavicular region. The pressure gradient exists in both systole and diastole (aortic pressure always exceeds pulmonary artery pressure in a normal PDA), hence the continuous character.
clinical Quiz
Four original clinical questions. Full explanations included.
Question 1 of 8
A 4-year-old boy is brought to the ER for a "blue spell." His mother reports he turned deeply blue during a tantrum, then squatted down and the color improved. He has had prior similar episodes. Physical exam reveals a harsh systolic ejection murmur at the left upper sternal border. Chest X-ray shows a boot-shaped cardiac silhouette.
Which of the following correctly describes the four anatomical defects responsible for this presentation?
Tempting to pick TGA since both cause cyanosis in newborns and both are cyanotic CHDs. But the squatting response and boot-shaped heart are TOF-specific clues that TGA cannot explain. Think of RVOT obstruction as a kinked garden hose: squatting compresses the femoral arteries, raising systemic resistance, and the increased back-pressure forces more blood to find the alternate route through the kinked hose into the lungs. TGA has parallel circuits with no kink to force blood through.
Correct: A. Tetralogy of Fallot.
Tet spells are hypercyanotic episodes where the dynamic RVOT obstruction worsens acutely, shunting more deoxygenated blood through the overriding aorta into the systemic circulation. Squatting increases SVR by compressing the femoral arteries, which pushes more blood through the stenotic RVOT into the lungs, improving oxygenation. The boot-shaped heart is caused by RVH lifting and rotating the apex.
The four components (PROVe): Pulmonary stenosis + RVH + Overriding aorta + VSD.
Why the others are wrong:
B: Fabricated combination, no CHD matches this pattern.
C: Tricuspid atresia has left axis deviation on ECG (dominant LV), not a boot-shaped heart; RVOT murmur and squatting response are absent.
D: TGA presents day 1-2 with severe cyanosis and an egg-on-a-string CXR; no boot-shaped heart and no relief with squatting.
Break it down: TOF = PROVe (Pulmonary stenosis + RVH + Overriding aorta + VSD); boot-shaped heart from RVH; squatting raises SVR forcing more flow through RVOT; tet spells = acute RVOT obstruction worsening.
A 36-year-old woman presents to a cardiologist with progressive shortness of breath on exertion and two episodes of stroke-like symptoms. She has no history of hypertension or smoking. Physical exam reveals a fixed split S2 and a systolic ejection murmur at the left upper sternal border. Echocardiogram shows a 2 cm defect in the mid-interatrial septum.
Which additional cardiac finding is MOST likely to explain her stroke-like episodes?
Tempting to pick endocarditis since cardiac shunts and IE seem naturally linked. But ASD is a large-bore, low-velocity connection, not the high-velocity jet that damages endothelium and creates the nidus for endocarditis. Think of paradoxical embolism as a tunnel bypass under a quality control station: a venous clot that would normally be filtered in the pulmonary capillaries finds the ASD tunnel, skips the filter entirely, and arrives in the systemic arterial system. Young patient with stroke and no traditional risk factors = look for the tunnel.
Correct: B. Paradoxical embolism through the atrial defect.
An ASD allows venous thrombi from the right heart to bypass the pulmonary circulation entirely and enter the systemic arterial circulation directly. This paradoxical embolism explains cryptogenic stroke in young patients with ASD or patent foramen ovale. The fixed split S2 (RA filling equalized by the shunt, removing respiratory variation) is pathognomonic for ASD.
Why the others are wrong:
A: Endocarditis is more common with VSD (high-velocity jet) or with valvular abnormalities. ASD is a low-velocity, large-orifice shunt with low endocarditis risk.
C: Pulmonary vein thrombosis is a rare complication of pulmonary fibrosis or post-ablation, not ASD. LA pressure is actually normal or low in ASD due to the decompressing shunt.
D: Coronary artery dissection is not a complication of increased cardiac output from shunts; it occurs in peripartum women and athletes, and is unrelated to ASD.
Break it down: ASD = paradoxical embolism (DVT bypasses lungs via defect, reaches systemic circulation); fixed split S2 = pathognomonic for ASD; low-pressure large-orifice shunt = low IE risk; cryptogenic stroke in young patient = look for ASD/PFO.
A newborn is noted to have cyanosis immediately after birth. Supplemental oxygen does not improve saturation. Prostaglandin E1 is administered. Chest X-ray shows an "egg on a string" cardiac silhouette. Echocardiogram confirms the aorta arising from the right ventricle and the pulmonary artery arising from the left ventricle.
What is the definitive surgical repair for this condition?
Tempting to pick the BT shunt since it is the most commonly tested palliative cardiac surgery for cyanotic CHD. But BT shunt only increases pulmonary blood flow, it does not fix the anatomical problem in TGA. Think of TGA as two train lines running in parallel on the wrong tracks: the BT shunt adds more trains to one line, but they are still on the wrong track. The arterial switch operation physically moves both lines to their correct tracks and re-connects all the switches.
Correct: C. Arterial switch operation (Jatene procedure).
TGA requires the arterial switch operation performed in the first 2 weeks of life. The aorta and pulmonary artery are transected and re-anastomosed to their correct ventricles (aorta to LV, pulmonary artery to RV), and the coronary arteries are reimplanted. PGE1 bridges the infant to surgery by maintaining ductal patency for mixing.
Why the others are wrong:
A: BT shunt (subclavian artery to pulmonary artery) is palliative for TOF and other lesions with reduced pulmonary blood flow. It increases pulmonary flow but does not correct the great vessel transposition.
B: Fontan procedure connects systemic veins directly to pulmonary arteries, bypassing the right heart entirely. Used for single-ventricle lesions such as tricuspid atresia and hypoplastic left heart syndrome, not TGA.
D: Ross procedure replaces a diseased aortic valve with the patient's own pulmonic valve. Unrelated to TGA.
Break it down: TGA = arterial switch operation (Jatene) in first 2 weeks of life; PGE1 bridges to surgery by maintaining ductal mixing; BT shunt = palliative for TOF (reduced pulmonary flow), not TGA; arterial switch physically re-anastomoses aorta and pulmonary artery to correct ventricles.
A 17-year-old male is found to have blood pressure of 180/40 mmHg in his right arm. His left arm reads 130/80 mmHg. Femoral pulses are weak and delayed compared to radial pulses. Chest X-ray shows bilateral rib notching. Echocardiogram reveals a bicuspid aortic valve.
Which chromosomal syndrome is most commonly associated with this condition?
Tempting to pick DiGeorge syndrome since both affect the aortic arch development and both are genetic conditions with cardiac defects. But DiGeorge produces conotruncal defects (TOF, truncus arteriosus) from neural crest migration failure, not coarctation. Think of each chromosome syndrome as having its own cardiac fingerprint stamped into the developmental blueprint: Turner (45,X) always stamps coarctation, Down stamps AVSD, DiGeorge stamps conotruncal defects. The combination of unequal arm BPs plus radio-femoral delay plus rib notching in an adolescent girl is the Turner coarctation signature.
Correct: C. Turner syndrome (45,X).
This is postductal coarctation of the aorta. The combination of unequal arm blood pressures (right > left when the coarctation involves or is near the left subclavian origin), radio-femoral delay, rib notching (inferior rib surfaces eroded by enlarged intercostal collateral arteries), and bicuspid aortic valve is classic. Coarctation is the most common CHD in Turner syndrome, affecting 10-15% of patients with 45,X.
Why the others are wrong:
A: Down syndrome (Trisomy 21) is associated with AVSD and VSD, not coarctation.
B: DiGeorge syndrome (22q11 deletion) is associated with Truncus arteriosus and TOF, not coarctation. These are conotruncal defects from abnormal neural crest migration.
D: Trisomy 18 (Edwards syndrome) is associated with VSD and other defects, but patients with Trisomy 18 rarely survive to adolescence (median survival less than 2 weeks); the age presentation rules this out.
Break it down: coarctation = Turner syndrome (45,X) cardiac fingerprint; rib notching = intercostal collateral arteries eroding inferior rib surfaces; AVSD = Down syndrome; TOF or truncus = DiGeorge (22q11); each chromosome syndrome has its own cardiac fingerprint.
A 2-day-old boy born at 28 weeks gestation is noted to have bounding peripheral pulses and a continuous machinery-like murmur at the left infraclavicular region. Chest X-ray shows cardiomegaly and pulmonary vascular congestion. Echocardiogram confirms a large communication between the aorta and pulmonary artery.
Which pharmacologic agent is first-line to close this defect in a premature infant?
Tempting to pick PGE1 since prostaglandins are directly involved in PDA and PGE1 is the board-tested drug for neonatal cardiac emergencies. But PGE1 does the opposite: it keeps the ductus open. Think of PGE1 as a chemical doorstop and indomethacin as the person who kicks the doorstop away. PGE1 holds the door open for ductal-dependent cyanotic lesions. Indomethacin removes the signal that was propping the door open so the ductus can finally close.
Correct: B. Indomethacin.
This is a patent ductus arteriosus (PDA). The ductus arteriosus stays open in the fetus because prostaglandins keep it dilated. After birth, rising oxygen levels and falling prostaglandins cause it to close. In premature infants, prostaglandin synthesis persists longer and the duct is less responsive to oxygen, so it remains patent. Indomethacin is a COX inhibitor that blocks prostaglandin synthesis, removing the "stay open" signal and allowing the duct to constrict. Think of prostaglandins as a finger in a dam; indomethacin pulls the finger out.
Why the others are wrong:
A and C: PGE1 (prostaglandin E1, alprostadil) is used to KEEP the ductus open in ductal-dependent lesions (TGA, critical coarctation, pulmonary atresia). Giving it here would worsen the PDA.
D: Digoxin does not close structural defects; it is used for rate control and heart failure, not to eliminate shunts.
Break it down: close PDA = indomethacin (COX inhibitor removes prostaglandin signal); PGE1 = OPENS ductus for ductal-dependent cyanotic lesions; opposite actions, same prostaglandin pathway; premature infants = persistent prostaglandin synthesis keeps ductus patent.
A 6-year-old girl with a known large ventricular septal defect that was not repaired in infancy now presents with worsening cyanosis and exercise intolerance. Examination reveals clubbing and central cyanosis. Echocardiogram shows right-to-left shunting through the VSD with severe right ventricular hypertrophy and estimated pulmonary artery pressure exceeding systemic pressure.
What physiological process best explains the reversal of shunt direction?
Tempting to pick LV failure since that would lower the left-to-right pressure gradient and seem to reduce the shunt. But LV failure reduces the gradient without reversing it, and does not cause cyanosis, clubbing, and polycythemia. Think of Eisenmenger as a one-way street that runs for decades before flipping to two-way: the pulmonary arterioles gradually remodel and thicken under the chronic flood of blood, raising the resistance on the right side until it matches and then exceeds the left. Once the sign flips, cyanosed blood flows backward. The shunt that once caused no symptoms now causes end-stage disease.
Correct: D. Eisenmenger physiology.
A large, unrepaired left-to-right shunt (VSD, ASD, PDA) chronically floods the pulmonary vasculature with excess blood. Over years, the pulmonary arterioles remodel: their walls thicken and their lumens narrow, driving pulmonary vascular resistance (PVR) progressively higher. When PVR finally exceeds systemic vascular resistance (SVR), the pressure in the right ventricle exceeds that on the left, and shunting reverses: now deoxygenated blood flows from right to left, bypassing the lungs and reaching the aorta. Cyanosis, clubbing, and polycythemia follow. This is Eisenmenger syndrome, the irreversible endpoint of untreated large left-to-right shunts.
Why the others are wrong:
A: Elevated LVEDP from LV failure would reduce the left-to-right gradient but would not reverse it unless PVR exceeded SVR.
B: Tricuspid regurgitation affects RA pressure, not RV pressure, and does not directly cause reversal of a ventricular-level shunt.
C: Aortic stenosis increases LV afterload, which tends to maintain or increase systemic pressure; the opposite of what would be needed to reverse the shunt.
Break it down: Eisenmenger = PVR exceeds SVR causing right-to-left shunt reversal; untreated large left-to-right shunt (VSD, ASD, PDA) causes irreversible pulmonary arteriole remodeling; cyanosis, clubbing, polycythemia = clinical triad; surgical repair is contraindicated once Eisenmenger develops.
A newborn girl is cyanotic at birth. Oxygen supplementation does not raise her saturation above 75%. Prostaglandin E1 is started. Echocardiogram shows total anomalous pulmonary venous return (TAPVR) with obstruction at the site where the pulmonary veins drain into a systemic vein below the diaphragm.
Why does prostaglandin E1 NOT provide adequate palliation in obstructed TAPVR, unlike in TGA?
Tempting to give PGE1 since it is the first-line drug for cyanotic newborns awaiting surgery, and both TGA and TAPVR are cyanotic CHDs requiring surgery. But the anatomy is different. Think of TAPVR with obstruction as a flooded basement with a blocked drain: PGE1 opens a window on the ground floor (the ductus), but the basement water cannot escape because the drain is blocked. The ground floor window does nothing for the basement. The surgical team needs to clear the drain directly.
Correct: A.
In TGA, PGE1 buys time by keeping the ductus arteriosus open so some mixing can occur between the parallel circulations. In TAPVR, the problem is different: all four pulmonary veins drain anomalously into systemic veins instead of the left atrium, so oxygenated blood never reaches the left heart directly. When the drainage pathway is obstructed (most often in the infracardiac type, where veins pass through the diaphragm), blood cannot leave the lungs adequately; pulmonary venous hypertension, pulmonary edema, and severe hypoxia follow. Keeping the ductus open with PGE1 allows some flow across it, but it cannot decompress the obstructed pulmonary veins upstream. Obstructed TAPVR is a surgical emergency requiring immediate repair.
Why the others are wrong:
B: PGE1 is not absolutely contraindicated; it may still be given pending surgery. The issue is efficacy, not contraindication.
C: PGE1 is a vasodilator, not a vasoconstrictor. It dilates the ductus and can mildly dilate pulmonary vasculature.
D: Most TAPVR cases have an atrial communication (ASD or PFO) that allows some mixing. The obstruction is in the pulmonary venous return pathway, not at the atrial level.
Break it down: obstructed TAPVR = surgical emergency requiring immediate repair; PGE1 cannot decompress obstructed pulmonary veins upstream; TGA = PGE1 helps (allows mixing through ductus); TAPVR obstruction = infracardiac type (veins pass through diaphragm) is most commonly obstructed.
A 3-year-old girl with Down syndrome is evaluated for a cardiac murmur. Echocardiogram shows a primum atrial septal defect combined with a cleft mitral valve and a large inlet ventricular septal defect, with a single common atrioventricular valve.
Which cardiac defect is most specifically associated with trisomy 21?
Tempting to pick VSD since it is the most common CHD overall and Down syndrome patients clearly have cardiac defects. But Down syndrome has a specific developmental mechanism that targets the AV junction, not a random increased risk of all defects. Think of the endocardial cushion development as the central plug-in point for the heart's internal wall construction: trisomy 21 disrupts the plug-in process, leaving a gap in the lower atrial septum, upper ventricular septum, and AV valves simultaneously. VSD alone would be a different plug-in point failing.
Correct: C. Atrioventricular septal defect (AVSD), also called endocardial cushion defect.
Down syndrome (trisomy 21) is the classic association with AVSD, occurring in approximately 40-50% of patients with AVSD who have a chromosomal abnormality. The endocardial cushions form the central fibrous skeleton of the heart including the lower atrial septum, upper ventricular septum, and AV valve leaflets. In trisomy 21, endocardial cushion development is disrupted, resulting in the spectrum from partial AVSD (primum ASD + cleft mitral valve) to complete AVSD (common AV valve + both ASD and VSD).
Why the others are wrong:
A: TOF is associated with 22q11 deletion (DiGeorge) and Noonan syndrome, not Down syndrome.
B: Coarctation of the aorta is specifically associated with Turner syndrome (45,X).
D: TGA is more commonly sporadic or associated with maternal diabetes, not trisomy 21.
Break it down: Down syndrome (trisomy 21) = AVSD (endocardial cushion defect); Turner (45,X) = coarctation; DiGeorge (22q11) = TOF or truncus arteriosus; each chromosome syndrome has its own cardiac fingerprint stamped into developmental biology.
0/8
Loading...
25-Question Walkthrough
Original clinical vignettes. Shuffled, never-repeat, full cause-to-effect explanations.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 1, 2026 at 10:03 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.