Three structural heart diseases that look different, fail differently, and kill differently
A 22-year-old athlete collapses during a basketball game. Echocardiogram shows asymmetric septal hypertrophy (3.0 cm), systolic anterior motion (SAM) of the mitral valve, and dynamic LVOT obstruction. Which of the following makes his obstruction WORSE?
Same organ. Completely different structural problems. Know the pattern before memorizing the details.
Tap any card to open it in place. The SVG shows why EF differs across the three types.
Asymmetric septal hypertrophy · LV is too thick · can't relax · diastolic dysfunction · EF normal or HIGH
Beta-myosin heavy chain (MYH7) or MYBPC3 · autosomal dominant · screen first-degree relatives
Harsh LLSB murmur · LOUDER with Valsalva/standing (decreased preload) · softer with squat/leg raise · young athlete SCD
Metoprolol or verapamil (slow HR, improve filling) · ICD (SCD prevention) · avoid vasodilators
Valsalva louder = HCM. Only murmur that does this.
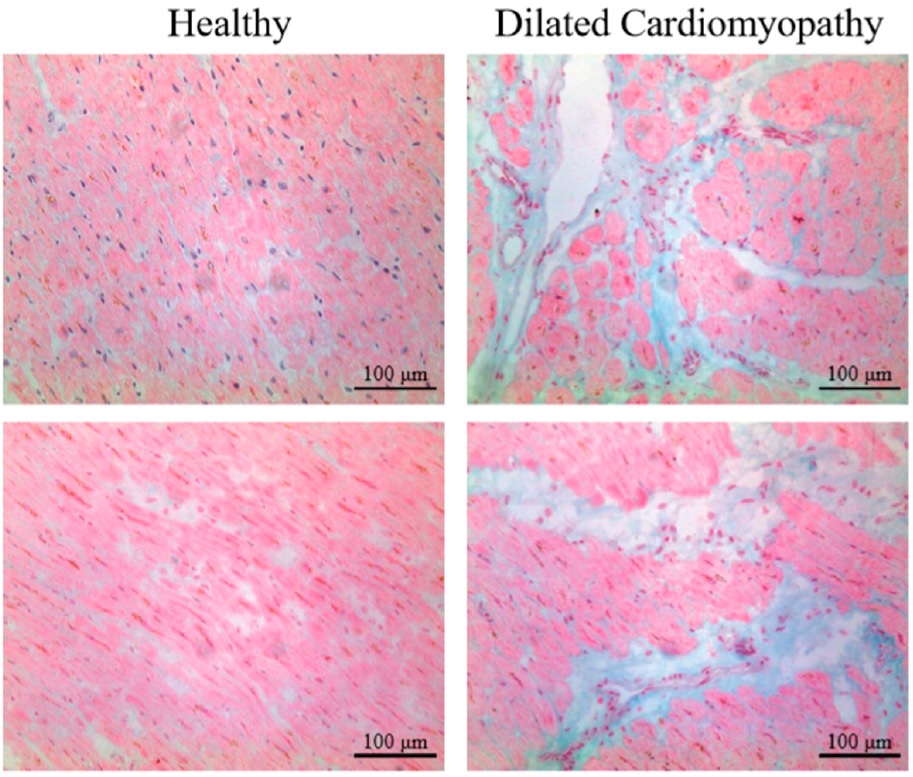
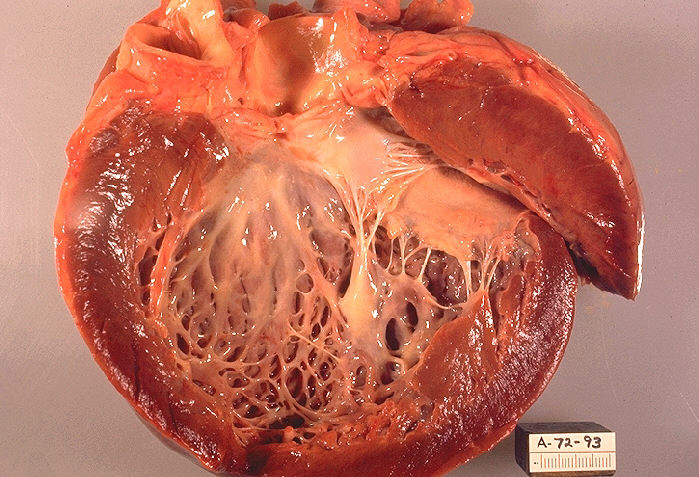
All 4 chambers dilated · thin walls · can't squeeze · systolic dysfunction · EF LOW (<40%)
ACEi + beta-blocker + diuretic · ICD if EF <35% · CRT if QRS >150ms + LBBB
S3 gallop + dilated chambers + low EF = DCM
Stiff walls · can't fill · diastolic dysfunction · EF normal · elevated filling pressures in both ventricles
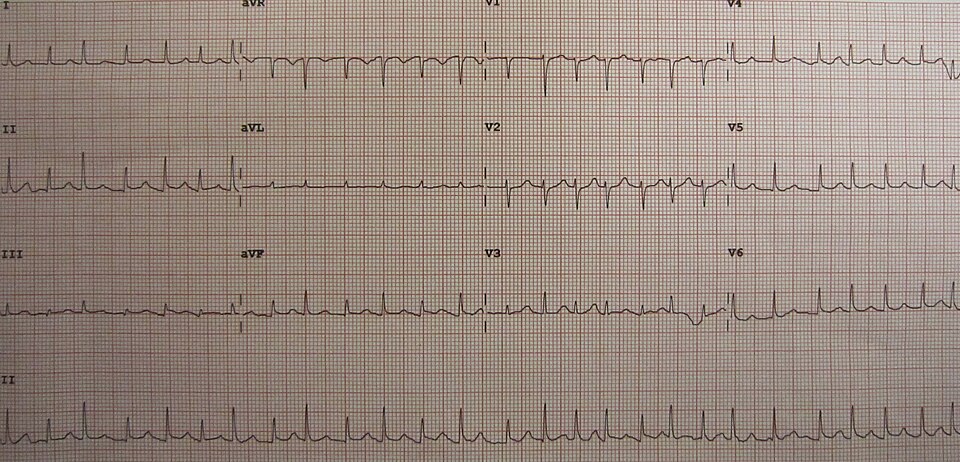
Kussmaul sign · low voltage on ECG but thick walls on echo · pericardial knock absent (not constrictive)
Low ECG voltage + thick echo walls = amyloid RCM
Rule: Smaller LV = worse obstruction = louder murmur. Bigger LV = less obstruction = softer.
Aortic stenosis does the OPPOSITE of HCM on maneuvers.
Both are harsh systolic murmurs. The maneuvers are how you tell them apart on the clinical medicine.
| Feature | HCM | Aortic Stenosis |
|---|---|---|
| Location | LLSB | RUSB |
| Radiation | Apex (not carotids) | Carotids |
| Valsalva / Standing | LOUDER (decreased preload, smaller LV) | Softer |
| Squatting / Leg Raise | Softer (increased preload, larger LV) | Louder |
| S4 gallop | Present | Present |
| EF | Normal or High | Normal early, low late |
| Pulse quality | Bisferiens pulse (spike-and-dome) | Pulsus parvus et tardus (weak, delayed) |
| Obstruction type | Dynamic (varies with preload) | Fixed (valve orifice) |
Stop memorizing maneuver lists. Ask one question: did the LV cavity get smaller or bigger? Smaller cavity (Valsalva, standing, dehydration) drives the septum into the SAM leaflet and the dynamic murmur screams. Bigger cavity (squat, leg raise, handgrip, fluids, phenylephrine) pulls them apart and it quiets down. HOCM is the one murmur that gets louder when you make the heart smaller.
clinical medicine rarely say the diagnosis. They hand you one phrase and expect you to land the type. Tap a clue, then name it before the answer drops. Color follows the disease the clue points to.
Tap each card to reveal the detail. Know the cause, know the test, know the stain.
Autosomal dominant, 50% de novo mutations. Two most tested loci:
1. MYH7 (beta-myosin heavy chain): Motor protein of the thick filament. Mutations increase cross-bridge cycling, causing hypercontractility and compensatory hypertrophy. Generally presents earlier and more severely.
2. MYBPC3 (myosin-binding protein C): Regulatory protein that modulates cross-bridge kinetics. More common overall, but often later onset and milder phenotype. Both are sarcomere genes, reinforcing that HCM is a disease of the contractile apparatus.
Family screening protocol: Echo + genetic testing in all first-degree relatives. Echo every 12-18 months in at-risk adolescents during growth spurts (HCM can develop or worsen during rapid growth).
A: Alcohol. Toxic dilated CMP. Dose-dependent. Abstinence can partially reverse it.
B: Beri-beri (thiamine/B1 deficiency). Wet beriberi = high-output heart failure. Causes peripheral vasodilation leading to high cardiac output, which eventually leads to dilated, high-output cardiomyopathy. Give thiamine first before glucose in any alcoholic presenting with HF.
C: Coxsackie B myocarditis. Viral infection directly damages myocytes. DCM can develop weeks to months after an acute viral illness. Associated with chest pain, troponin elevation, and new dilated LV.
D: Doxorubicin (Adriamycin). Cumulative dose-dependent cardiotoxicity. Causes free radical damage to cardiomyocytes. Lifetime dose limit. Dexrazoxane used for cardioprotection in certain cases.
E: Everything else. Idiopathic (most common, 50%). Peripartum (last month of pregnancy to 5 months postpartum, treat with standard HF therapy, may recover). Chagas disease (T. cruzi, apical aneurysm on echo is classic). Genetic/familial (titin/TTN mutations most common).
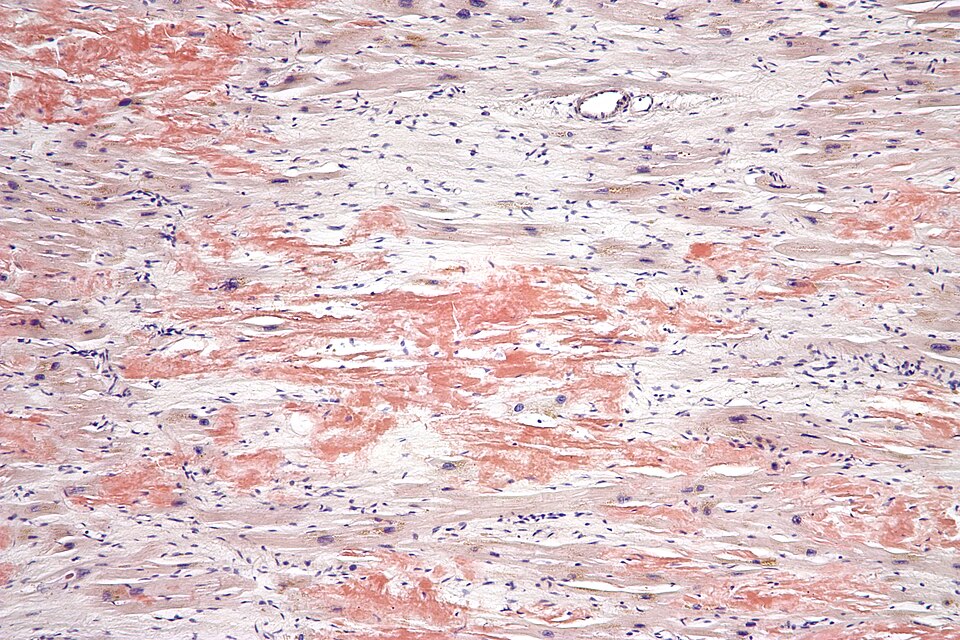
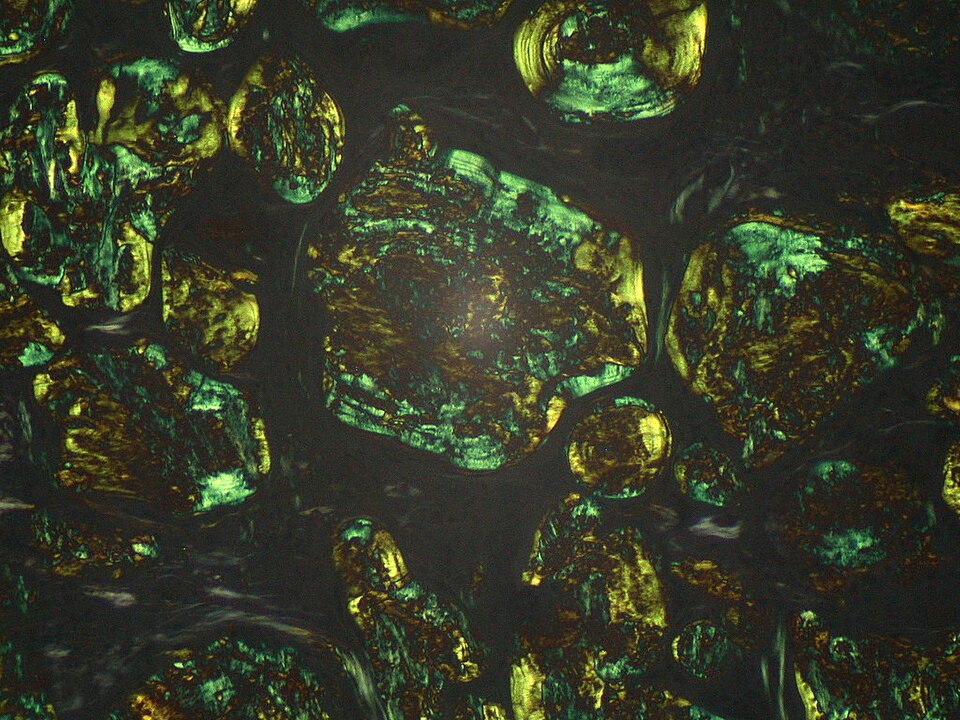
Amyloidosis (most common cause): AL type (from plasma cell dyscrasia, think multiple myeloma) or AA type (from chronic inflammation). Diagnosis: Congo red stain shows apple-green birefringence under polarized light. Send serum/urine SPEP to look for monoclonal light chains in AL amyloid. Cardiac biopsy shows amyloid fibrils in the myocardium. Echo: granular sparkling appearance of the myocardium.
Sarcoidosis: Noncaseating granulomas infiltrate the myocardium. Can cause arrhythmias and conduction disease (heart block) in addition to restrictive physiology. Diagnosis: biopsy of accessible tissue (lung, lymph node, skin). Treat with steroids.
Hemochromatosis: Iron deposits throughout the body. Classic triad: bronze diabetes (iron in pancreas and skin), cirrhosis, cardiomyopathy (can be dilated or restrictive). Elevated transferrin saturation and serum ferritin. Prussian blue stain shows iron deposits. Treatment: therapeutic phlebotomy or deferoxamine.
Apply the clues in order. Eliminate wrong answers. One correct diagnosis survives.
Original clinical vignettes. Shuffled, never-repeat, full Chicago explanations.
