The granuloma that touches everything → lungs, skin, eyes, heart. How one mechanism creates a whole-body disease.

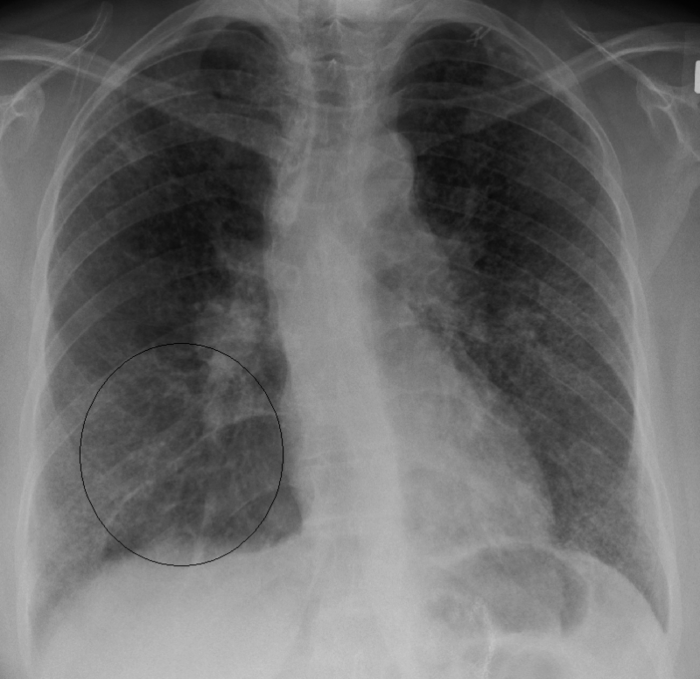
A 29-year-old African-American woman presents with 4 months of fever, progressive shortness of breath, and a dry cough. She's lost 5 kg. She visited Kenya 2 months ago. Exam: fine crackles and wheezing bilaterally. Labs: calcium 11.8 mg/dL (normal: 8.4-10.2). CXR: reticular opacities + bilateral hilar lymphadenopathy.
What's the underlying mechanism?
THE CASE
Patient walks in. Three clues hit you immediately. What do you make of them?
THE SMOKING GUN
Lab + imaging. These two together lock the diagnosis.
THE MECHANISM
One immune reaction, systemic consequences
Sarcoidosis is a Type IV hypersensitivityDelayed-type hypersensitivity. T-cells (not antibodies) drive the reaction. Same category as TB skin test reactions, contact dermatitis, and transplant rejection. Takes 24-72 hours to develop, which is why sarcoidosis is chronic, not acute. reaction to an unknown antigen. Nobody knows what triggers it. The immune system just... decides to fight something, and can't stop.
Here's the chain:
The granuloma macrophages also secrete ACE (angiotensin-converting enzyme) → which is why elevated serum ACE is a lab marker for sarcoidosis.🔑Sarcoidosis → Serum ACE ↑ (the granulomas are little ACE factories)
THE CALCIUM QUESTION
Same lab value, completely different mechanisms
| Sarcoidosis | Malignancy (SCC Lung) | |
|---|---|---|
| Trace It | Granuloma macrophages make 1-alpha hydroxylase → excess active vitamin D → ↑ gut Ca²⁺ absorption | Tumor secretes PTHrP → mimics PTH → ↑ bone resorption |
| Vitamin D | ↑ 1,25-(OH)₂D (calcitriol HIGH) | Normal or low |
| PTH | Suppressed (calcium is high, so PTH shuts down) | Suppressed (PTHrP, not PTH, is driving it) |
| PTHrP | Normal | Elevated |
| CXR | Bilateral hilar LAD, reticular opacities | Solitary mass or nodule |
| Demographics | Young (20-40), often African American | Older (50+), smoker |
| Treatment | Steroids (suppress the granulomas) | Treat the cancer + IV fluids + bisphosphonates |
MULTI-SYSTEM
Tap each organ to see what happens when granulomas show up there
CLINICAL
What to order and what to give
Diagnosis:
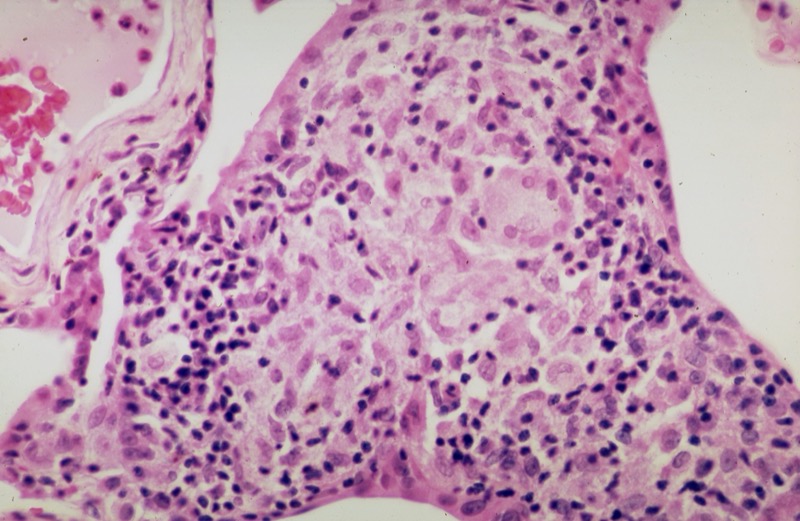
Gold standard is biopsy showing non-caseating granulomas. Transbronchial biopsy is most common approach. You'll also see:
| Test | Finding | Why |
|---|---|---|
| CXR | Bilateral hilar LAD | Granulomas in hilar lymph nodes |
| Serum ACE | ↑ Elevated | Granuloma macrophages produce ACE |
| Calcium | ↑ Hypercalcemia | 1-alpha hydroxylase → excess calcitriol |
| 1,25-(OH)₂D | ↑ Elevated | Same mechanism → granulomas make active vit D |
| Biopsy | Non-caseating granulomas | Confirms diagnosis, rules out TB/fungal |
| CD4:CD8 ratio (BAL) | ↑ Elevated | Th1-predominant response in alveoli |
Treatment:
Corticosteroids → suppress the granulomatous inflammation. Not everyone needs treatment though → many patients with Stage I disease self-resolve. Treat when there's: organ damage, hypercalcemia, eye involvement, cardiac or neuro involvement, or progressive lung disease.
Steroid-sparing agents for refractory cases: methotrexate, azathioprine, infliximab.
Histology buzzwords:
| Finding | What It Is |
|---|---|
| Non-caseating granulomas | Tight clusters of epithelioid macrophages, NO central necrosis |
| Schaumann bodies | Calcified, laminated concretions inside giant cells (calcium + protein deposits) |
| Asteroid bodies | Star-shaped inclusions inside giant cells (cytoskeletal remnants) |
| Multinucleated giant cells | Fused macrophages → Langhans-type (nuclei arranged in horseshoe pattern) |
GAME TIME
Four mechanisms. One matches sarcoidosis. Watch the clues knock them out.
PROVE IT
5 patients just showed up. Don't let the granulomas fool you.
Original clinical vignettes. Shuffled, never-repeat, full explanations for every choice.