Virchow's triad, the Wells score, and the workup algorithm that decides who gets a scan, who gets thrombolytics, and who walks out alive.
Opening Challenge
A 45-year-old woman is 3 days out from a total hip replacement when she develops sudden pleuritic chest pain and dyspnea. HR 115 (60 to 100), RR 24 (12 to 20), BP 124/78, SpO2 92% on room air. Right calf is asymmetrically swollen and tender. ECG shows sinus tachycardia. Adding the swollen leg, the recent surgery, and PE as the leading diagnosis, her Wells PE score lands at 7 (high probability).
What is the single best next step?
A) Send a serum D-dimer first
B) CT pulmonary angiography (CTA-PE)
C) V/Q scan immediately
D) Lower extremity duplex ultrasound
Her Wells score is 7. What does a high pre-test probability do to the value of a D-dimer? D-dimer is roughly 97% sensitive but only 40 to 50% specific, so it earns its keep only as a rule-out tool when probability is low. If you order it here and it comes back negative, do you believe it? You cannot: the residual risk after a high pre-test probability plus a "negative" D-dimer is still high enough to kill her. So you skip the screening test and go to the test that locates clot. V/Q is the fallback only when contrast is contraindicated (renal failure, contrast allergy) or in pregnancy; duplex finds the leg clot, not the lung clot. When pre-test probability is high, skip the D-dimer and go straight to CTA-PE.
01 · The Foundation
Virchow's Triad
Three conditions that tilt the balance toward clot formation. DVT always starts in the deep veins of the proximal leg, in the valve pockets where flow is slowest.
01 · Stasis
Stasis
Sluggish blood flow allows coagulation factors to accumulate and clot formation to begin.
Key anatomic fact: DVT starts in the valve pockets of deep veins ⓘProximal clot (femoral, iliac) embolizes to the lung far more than distal calf clot. Calf clots matter mostly when they propagate proximally.. Proximal DVT (femoral, iliac) carries higher PE risk than distal (calf). Calf DVTs that propagate proximally are the main PE source.
Increased clotting tendency, either inherited or acquired.
Inherited: Factor V Leiden (most common inherited thrombophilia, causes activated protein C resistance) 🔑Very Popular: Factor V Leiden is the #1 inherited clot risk. APC cannot cut the mutant factor Va., Prothrombin G20210A mutation, Protein C/S deficiency, Antithrombin III deficiency.
Acquired: Antiphospholipid syndrome (APS) with lupus anticoagulant. Paradox: aPTT is prolonged IN THE LAB (in vitro), but causes thrombosis in the body (in vivo). OCP use (estrogen elevates clotting factors, depresses protein S). Malignancy: Trousseau syndrome = migratory thrombophlebitis from cancer-released procoagulants.
Factor V Leiden #1Protein C/S deficiencyAPS paradoxOCP + Factor V LeidenTrousseau syndrome
03 · Endothelial Injury
Endothelial Injury
Damaged vessel wall exposes subendothelial collagen and tissue factor, triggering the coagulation cascade directly.
Causes: surgery (especially orthopedic, abdominal, pelvic), trauma, central venous catheter placement, atherosclerotic plaque disruption, vasculitis.
Why hip/knee replacement carries the highest DVT risk: mechanical trauma to the deep femoral veins during surgery + stasis from positioning + post-op immobility = all three arms of the triad hit simultaneously.
Surgery / traumaCentral linesAtherosclerosisVasculitis
From the AttendingFactor V Leiden + OCP: Factor V Leiden (activated protein C resistance) is the most common inherited thrombophilia. Oral contraceptives containing estrogen further increase clotting factor levels and reduce protein S. Combining both = very high VTE risk. Always screen for thrombophilia before starting OCPs in patients with a personal or family history of clots. 🔑Estrogen + Leiden = stacked risk. Estrogen raises clotting factors and lowers protein S on top of the inherited defect.
From the AttendingAPS paradox explained: Antiphospholipid antibodies bind phospholipids used in the aPTT assay, prolonging it in vitro. But in the body, these antibodies activate endothelium and platelets, causing arterial and venous thrombosis, plus recurrent pregnancy loss (antiphospholipid antibodies interfere with placental vasculature).
02 · Risk Stratification
Wells Score + Workup Algorithm
Pre-test probability drives everything. Score first, then choose your test. Never go straight to imaging without a clinical probability estimate.
Wells PE Score
DVT Wells Score
Points Added
Clinical signs and symptoms of DVT (swelling, tenderness along deep veins)+3
PE is the #1 diagnosis, or equally likely as an alternative+3
Heart rate > 100 bpm+1.5
Immobilization > 3 days OR surgery in the past 4 weeks+1.5
Prior DVT or PE+1.5
Hemoptysis+1
Malignancy on treatment, or palliated in past 6 months+1
PE Workup Algorithm
Calculate Wells PE Score
↓
Score 0-1 · LOW
D-dimer first
↓
Negative
PE ruled out. Stop.
Positive
CT-PA
Score 2-6 · MODERATE
D-dimer first
↓
Negative
Consider stopping
Positive
CT-PA
Score >4 (>6 simplified) · HIGH
Skip D-dimer entirely
↓
CT-PA directly
From the AttendingWhy skip D-dimer when probability is high: D-dimer has high sensitivity (~97%) but terrible specificity. Any condition causing fibrinolysis (surgery, infection, malignancy, old age, pregnancy) elevates D-dimer. In a high-probability patient, a negative D-dimer is dangerous. The pre-test probability plus a negative D-dimer still leaves too much residual risk. Go directly to CT-PA.
Points
Active cancer (on treatment or within 6 months)+1
Paralysis, paresis, or recent plaster immobilization of lower extremity+1
Recently bedridden > 3 days or major surgery within 4 weeks+1
Localized tenderness along distribution of the deep venous system+1
Entire leg swollen+1
Calf swelling > 3 cm compared with asymptomatic leg+1
Pitting edema confined to symptomatic leg+1
Collateral superficial veins (non-varicose)+1
Alternative diagnosis as likely or more likely than DVT-2
DVT Workup Algorithm
Calculate DVT Wells Score
↓
Score 0 · LOW
D-dimer
↓
Negative = DVT excluded
Score 1-2 · MODERATE
D-dimer OR duplex US
↓
Negative D-dimer = stop. Positive = duplex US.
Score ≥2 · HIGH
Duplex US directly
↓
No D-dimer needed
From the AttendingDuplex ultrasound: The imaging test of choice for DVT. Non-invasive, no radiation, no contrast. Compressibility of the vein is the key finding. A normal vein compresses under probe pressure. A DVT does not compress. High sensitivity for proximal DVT (femoral, popliteal). Lower sensitivity for distal (calf) DVT.
03 · Diagnostic Tools
Diagnosis Tools
Tap each card to reveal the details. Know what each test does well, and where it fails.
Mechanism in Motion · From Valve Pocket to Lung
Watch a clot detach from a leg-vein valve pocket, ride the venous return, and lodge in a pulmonary artery. The downstream lung loses perfusion while ventilation continues: a V/Q mismatch, and the right ventricle meets a sudden wall.
Lung perfused · V matches Q
Clinical Imaging
What It Looks Like
Tap any image for the full read.
CTA-PE · Filling defect
CTA · Massive occlusion
ECG · S1Q3T3
Duplex · Femoral DVT
Clinical · Swollen DVT leg
RevealBeat · The Wells-then-Test Logic
Tap each beat. Answer in your head before you reveal.
Why score before you scan? tap
Pre-test probability changes what a test result means. A "negative" D-dimer is reassuring only when probability was already low. Skipping the Wells step makes every downstream result uninterpretable.
High Wells: what do you order? tap
Go straight to CTA-PE. A negative D-dimer cannot lower a high pre-test probability below the threshold where you would stop, so the screening test wastes time and risks a fatal false reassurance.
When does V/Q replace CTA-PE? tap
When iodinated contrast is the problem: severe renal impairment, contrast anaphylaxis, or pregnancy. V/Q maps perfusion without contrast; read a mismatch as PE.
PERC: what does an all-negative rule buy you? tap
In a patient already judged low probability, eight negative PERC criteria drop the post-test risk below the testing threshold. You stop: no D-dimer, no imaging.
D-dimer▼
High sensitivity, low specificity. Elevated whenever fibrinolysis is happening anywhere in the body.
Sensitivity ~97%. Specificity only ~40-50%. That means a positive D-dimer tells you almost nothing on its own.
Use: Rule OUT PE when pre-test probability is LOW or MODERATE. A negative D-dimer in a low-probability patient essentially excludes PE (NPV ~99%).
Not useful when: Pre-test probability is high. Post-op state, active infection, cancer, pregnancy, and age >50 all elevate D-dimer independently.
Age-adjusted D-dimer: For patients over 50, the threshold is age x 10 ug/L instead of a fixed 500 ug/L. This reduces false positives in elderly patients.
High sensitivity (rule-out tool)Low specificity (many false positives)Only for low/moderate probability
CT-PA (CT Pulmonary Angiography)▼
Gold standard for PE diagnosis. Sensitivity ~95%, specificity ~98%. Can confirm and locate clot.
Shows filling defect in the pulmonary arteries where contrast is blocked by thrombus. Can see saddle emboli at the main pulmonary artery bifurcation, or peripheral segmental/subsegmental clots.
Also assesses severity: RV to LV diameter ratio on axial cuts. RV:LV >0.9 indicates right heart strain (massive/submassive PE). This determines treatment escalation.
Contraindications: Severe renal impairment (contrast nephropathy risk), known contrast allergy, pregnancy (radiation to fetus). In these cases, use V/Q scan instead.
Gold standardSensitivity ~95%, Spec ~98%Contrast requiredRV:LV ratio for severity
V/Q Scan▼
Ventilation-Perfusion scan. Inhaled radiotracer (ventilation) vs. injected radiotracer (perfusion). Compare the maps.
V/Q mismatch: Areas with normal ventilation but absent perfusion. This is the classic PE pattern. Blood can't get there because a clot is blocking the artery, but air still goes in.
Use when CT-PA is contraindicated: renal failure (no contrast), contrast allergy, or pregnancy (V/Q exposes fetus to lower radiation than CT-PA, and uses no iodinated contrast).
Interpretation: Normal V/Q essentially rules out PE. High-probability V/Q in the right clinical context confirms PE. Indeterminate V/Q requires CT-PA or other imaging.
No iodinated contrastSafe in renal failurePreferred in pregnancyIndeterminate results common
Echo + Troponin▼
Not for diagnosis. For severity stratification. Used after PE is confirmed to guide treatment intensity.
Echo findings in PE: RV dilation and hypokinesis. McConnell sign = RV free wall hypokinesis with preserved apical motion (fairly specific for acute PE). D-sign on parasternal short axis = interventricular septum bowing left from elevated RV pressure.
Troponin: Elevated troponin (I or T) in PE = RV myocardial injury from pressure overload. Elevated troponin + echo RV strain = submassive PE category. These patients need escalation beyond just anticoagulation alone.
BNP/NT-proBNP: Elevated BNP also indicates RV strain. Used alongside troponin to assess right heart stress.
Not for diagnosisSeverity stratification onlyMcConnell sign: RV free wall hypokinesisTroponin up = RV injury
From the AttendingOrder of operations: Wells score first. If low/moderate probability, D-dimer. If D-dimer negative, stop. If D-dimer positive or high probability, CT-PA. Add echo + troponin after confirming PE to stratify severity and determine if thrombolytics are needed.
04 · Treatment Algorithm
Treatment by Severity
Three categories. Treatment escalates from anticoagulation alone all the way to emergency embolectomy.
Subsegmental / Low-Risk
Submassive
Massive
Subsegmental PE · Provoked DVT · Low-Risk PE
Anticoagulation Alone
First-line: Direct Oral Anticoagulants (DOACs)
Rivaroxaban (factor Xa inhibitor) or Apixaban (factor Xa inhibitor) are preferred for most patients
Dabigatran (direct thrombin inhibitor) or Edoxaban are alternatives
DOACs have replaced warfarin for most non-cancer, non-APS patients
Duration:
Provoked (surgery, immobility, clear reversible cause): 3 months, then stop
Unprovoked (no identifiable trigger): 3-6 months minimum, then reassess. Consider indefinite if recurrence risk is high
Cancer-related VTE: LMWH (enoxaparin) preferred traditionally, but rivaroxaban and edoxaban are now evidence-based alternatives for cancer patients
Pregnant patients: DOACs are teratogenic. Use LMWH (enoxaparin) throughout pregnancy. Warfarin is teratogenic in first trimester; avoid.
From the AttendingWhy DOACs over warfarin: Fixed dosing (no regular INR monitoring), fewer drug and food interactions, lower intracranial bleeding risk, faster onset. The only situations where warfarin is still preferred: antiphospholipid syndrome (APS requires warfarin for INR target 2-3), mechanical heart valves, and patients who cannot afford DOACs.
Submassive PE · RV Strain · Hemodynamically Stable
Anticoagulation + Consider Escalation
Definition: PE with RV dysfunction (echo evidence of RV strain, RV:LV >0.9, McConnell sign) AND/OR biomarker elevation (troponin, BNP), but blood pressure is maintained (systolic >90 mmHg).
Standard: Anticoagulation (IV heparin initially)
Start IV unfractionated heparin (UFH) for immediate anticoagulation and flexibility if escalation is needed
Consider escalation if worsening:
Systemic thrombolytics (alteplase/tPA) at lower dose
Catheter-directed thrombolysis (CDT): delivers tPA directly into the pulmonary artery at lower systemic dose, reducing bleeding risk vs. systemic tPA
Decision is individualized based on bleeding risk vs. hemodynamic trajectory
From the AttendingSubmassive is the hardest decision: Patient is stable NOW but may deteriorate. The question is whether the benefit of thrombolysis outweighs the bleeding risk (especially intracranial hemorrhage, ~2-3% with systemic tPA). Catheter-directed thrombolysis is increasingly used because it reduces systemic tPA dose.
Massive PE · Hemodynamic Instability
Systemic Thrombolytics + Supportive Care
Definition: PE causing hemodynamic instability. Systolic BP <90 mmHg for >15 minutes, or requiring pressors, or cardiac arrest.
Step 1: Systemic thrombolytics (tPA / alteplase)
100 mg IV over 2 hours (standard adult dose)
This is a life-saving intervention when the patient is crashing
Check absolute contraindications: prior intracranial hemorrhage, recent (<3 months) ischemic stroke, intracranial neoplasm, active internal bleeding, recent (<3 months) major head trauma/surgery
Step 2: If tPA is absolutely contraindicated:
Surgical embolectomy (cardiothoracic surgery): direct extraction of clot
Catheter-based thrombectomy: mechanical disruption and aspiration via catheter
Supportive care:
Vasopressors (norepinephrine preferred) for hemodynamic support
IV fluids cautiously. Do NOT fluid overload. The RV is already stressed. Excess fluid further distends the RV, pushes septum left (D-sign), and reduces LV preload
Avoid high PEEP in intubated patients (increases RV afterload)
From the AttendingtPA in massive PE overrides most hesitation: A patient in PE-induced cardiac arrest or with BP <90 mmHg is going to die without reperfusion. The bleeding risk of tPA is acceptable vs. certain death. The only absolute bar is active intracranial pathology. Recent surgery is a RELATIVE contraindication, not absolute, in a dying patient.
Warfarin bridge rule: When initiating warfarin, you MUST overlap with heparin (UFH or LMWH) until INR is therapeutic (≥2.0) for at least 24 hours AND the patient has received warfarin for a minimum of 5 days. Warfarin initially drops Protein C and S (natural anticoagulants) before it drops the procoagulant factors II, IX, X. Without bridging, you create a temporary hypercoagulable window.
05 · Clinical Reasoning
Elimination Game
Use the clues to eliminate wrong answers one by one until only the diagnosis remains.
A 35-year-old woman presents after her third DVT in 5 years. She has had two spontaneous abortions in the past two years with no identified cause. Labs show a prolonged aPTT that does NOT correct with a 1:1 mixing study. ANA is weakly positive. She is not currently pregnant and has never been on OCPs.
Factor V Leiden
Antiphospholipid Syndrome
Protein C Deficiency
Prothrombin G20210A Mutation
Clue 1: "Prolonged aPTT that does NOT correct with a 1:1 mixing study (mixing study adds normal plasma to the patient's sample)."
Correction = patient lacks a clotting FACTOR, and normal plasma supplies the missing one. No correction = patient has an INHIBITOR (an antibody) blocking the phospholipid surface used in the aPTT assay. Factor V Leiden does not affect aPTT at all. Protein C deficiency does not prolong aPTT. Prothrombin G20210A gives elevated prothrombin levels, not a prolonged aPTT with inhibitor pattern.
Eliminating: Factor V Leiden, Protein C Deficiency, Prothrombin G20210A Mutation
Clue 2: "Third DVT + two spontaneous abortions + positive ANA + inhibitor on mixing study."
This is the classic triad of antiphospholipid syndrome: recurrent thrombosis (venous or arterial), recurrent pregnancy loss (antiphospholipid antibodies impair placental circulation, causing miscarriage), and laboratory confirmation (lupus anticoagulant = phospholipid-dependent aPTT prolongation with inhibitor pattern, OR anticardiolipin or anti-beta2-glycoprotein I antibodies). ANA positivity suggests an underlying autoimmune milieu, and APS is commonly associated with SLE.
Confirmed: Antiphospholipid Syndrome
Antiphospholipid Syndrome (APS)
The Sapporo criteria require two things: (1) clinical criterion (arterial or venous thrombosis, or pregnancy morbidity) AND (2) lab criterion (lupus anticoagulant, anticardiolipin IgG/IgM, or anti-beta2-glycoprotein I IgG/IgM on two occasions at least 12 weeks apart).
Treatment: Long-term anticoagulation with warfarin (INR 2-3). DOACs are NOT recommended for APS with positive lupus anticoagulant (higher recurrence rate vs. warfarin in trials). If she becomes pregnant: switch to LMWH + low-dose aspirin.
06 · clinical Walkthrough
clinical Walkthrough
Original clinical vignettes drawn one at a time. Shuffled, never-repeat, with a worked reasoning chain for every choice. Right-click or long-press an option to cross it out; double-tap to highlight.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 1, 2026 at 10:03 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.
 CTA-PE · Filling defect
CTA-PE · Filling defect
 CTA · Massive occlusion
CTA · Massive occlusion
 ECG · S1Q3T3
ECG · S1Q3T3
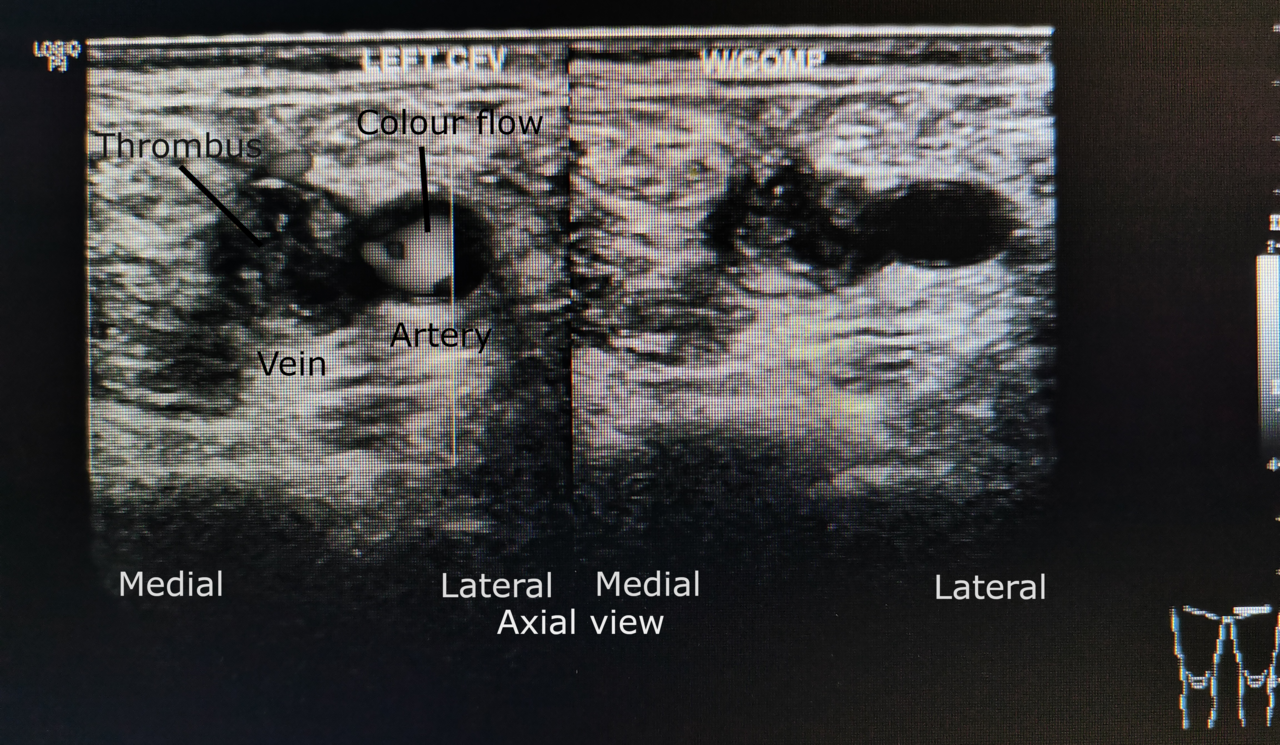 Duplex · Femoral DVT
Duplex · Femoral DVT
 Clinical · Swollen DVT leg
Clinical · Swollen DVT leg