Seizure, aspiration, anaerobes, cavity. The chain that clinical medicine love to test.
PROVE YOURSELF
One patient. One shot. What's the diagnosis?
ASPIRATION CASCADE
It's a 4-step disaster, and every step is testable.
Step 1: Loss of consciousness. Something knocks out the protective reflexes · the cough reflexYour airway's bouncer. Cough and epiglottic closure normally prevent anything from sliding past the vocal cords into the lungs. and epiglottic closure. In this case, it's a seizure. The patient loses consciousness, the airway goes unguarded, and whatever's sitting in the back of the throat has a free pass down.
Step 2: Aspiration. Oral flora · bacteria that normally live in the mouth and gums · slides into the lower airways. These aren't exotic bugs. They're the same anaerobes that cause gum disease and dental abscesses: PeptostreptococcusAnaerobic gram-positive cocci. Normal oral flora. Thrives in low-oxygen environments like deep gum pockets and, now, necrotic lung tissue., PrevotellaAnaerobic gram-negative rod. Common in the mouth, especially in periodontal disease. Major player in aspiration pneumonia and lung abscess., FusobacteriumAnaerobic gram-negative rod. Famous for Lemierre syndrome (septic jugular thrombophlebitis). Also a key player in aspiration lung abscesses., and BacteroidesAnaerobic gram-negative rod. B. fragilis is the GI star (below the diaphragm), but oral Bacteroides species are part of the aspiration abscess crew above the diaphragm..
Step 3: Infection festers. The aspirated bacteria land in gravity-dependent lung segments (more on that below) and set up shop. The immune system walls off the infection, tissue dies, and liquefactive necrosisThe tissue literally melts. Unlike caseating necrosis (cheesy, TB), liquefactive necrosis produces runny, pus-filled material. Lungs are especially prone because they're soft and air-filled. creates a pus-filled cavity.
Step 4: Cavity forms. The dead tissue breaks down, some drains into a bronchus (that's the productive cough), and air enters the cavity. Now you have the classic CXR finding: a cavitary lesion with an air-fluid level. Air on top, pus on the bottom. Like a half-empty bottle of chunky swamp water.
WHO ASPIRATES?
Tap each card to see WHY it causes aspiration.
The common thread: anything that compromises airway protection. The protective reflexes are the bouncer at the door of your lungs. When the bouncer passes out (seizure, alcohol, sedation) or is physically propped open (intubation), the mouth bacteria walk right in.
ANATOMY
Gravity picks the landing zone.
THE BUGS
These are mouth bacteria. That's the whole point.
Lung abscesses from aspiration are polymicrobial. You'll see a mix of anaerobes that normally live in your gingival crevices and tonsillar crypts. They're not exotic. They're not hospital-acquired. They're just oral flora that ended up where they shouldn't be.
| Organism | Gram Stain | Key Fact |
|---|---|---|
| Peptostreptococcus | Gram + cocci | Anaerobic version of strep. Common in dental, brain, lung abscesses |
| Prevotella | Gram − rod | Replaced Bacteroides as the #1 name for oral anaerobic GNR |
| Fusobacterium | Gram − rod | The Lemierre's bug. Spindle-shaped. Loves causing abscesses |
| Bacteroides (oral spp.) | Gram − rod | Not B. fragilis (that's GI). Oral species live above the diaphragm |
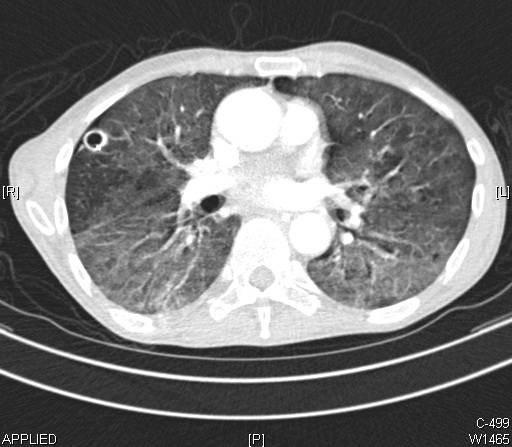
IMAGING
One image, three clues.
1. Cavitary lesion · a round, thick-walled area of destroyed lung tissue. The wall is irregular (unlike the thin-walled cysts of pneumatoceles). Think of it like a room-sized hole eaten through a building.
2. Air-fluid level · a perfectly flat horizontal line inside the cavity. Air floats on top, pus pools at the bottom. You know how if you half-fill a water bottle and hold it still, there's that clean horizontal line? Same physics. This requires an upright film to see.
3. Right lower lobe location · confirms the aspiration route. If you see a cavitary lesion in the upper lobe, your differential shifts hard toward TB or cancer.
DIFFERENTIAL
Four suspects. Only one fits. Eliminate them one by one.
TREATMENT
Cover anaerobes first. Drain only when the cavity refuses to empty.
KNOW THE DIFFERENCE
Same CXR finding, completely different diseases.
| Diagnosis | Location | Key Clue | Patient |
|---|---|---|---|
| Aspiration abscess | Right lower lobe | Foul sputum, air-fluid level | Seizures, alcoholism, stroke |
| TB | Upper lobes (apical) | Night sweats, weight loss, AFB+ | Immigration, HIV, prison, shelter |
| Lung cancer | Variable (often hilar) | Solitary mass, weight loss, hemoptysis | Older, heavy smoker (30+ pack-years) |
| Klebsiella pneumonia | Upper lobes | Currant-jelly sputum, bulging fissure | Alcoholic, diabetic |
| Aspergillus | Pre-existing cavity | Fungus ball (mycetoma), air-crescent sign | Immunocompromised, prior TB cavity |
VILLAINS
Tap each card. Know the mechanism, the patient, and the exact clue.
DECISION TREE
Step through the clues. Arrive at the diagnosis.
MEMORY HOOKS
Tap the key icon to unlock each mnemonic. clinical medicine anchors only.
Foul-smelling sputum means anaerobes. Aerobic bacteria do not produce volatile sulfur compounds. 🔑Foul = Fusobacterium and friends from the mouth. If the sputum reeks, the answer is anaerobes. If the sputum is just purulent, keep the differential open. The smell IS the culture.
The right main bronchus is wider, shorter, and more vertical than the left. Aspirated material goes right. 🔑Right = Receives aspirate. Think of the trachea as a highway that forks. The right exit is wider, closer, and goes almost straight down. Gravity sends everything right almost every time.
Supine aspiration hits the posterior segment of the RUL or superior segment of the RLL. 🔑Posterior = patient was on their Back. When lying flat, the posterior segments become gravity-dependent. A posterior RUL cavity = the patient aspirated while supine (after seizure, during surgery, in bed).
Metronidazole alone fails for lung abscess. It misses microaerophilic streptococci. 🔑Metronidazole = Missing strep. It kills strict anaerobes beautifully but microaerophilic strep (tolerate small O2) slip through. Clindamycin covers both groups. Metronidazole monotherapy = guaranteed treatment failure.
Klebsiella hits upper lobes in alcoholics and diabetics. Currant jelly sputum. 🔑Klebsiella = Kill the alcoholic with currant jelly. Upper lobe, bloody mucoid sputum (not foul), bulging fissure sign on CXR. Diabetics and alcoholics. The aggressive necrotizing bug that destroys the upper lobe rapidly.
Aspergilloma is an air crescent sign, not an air-fluid level. 🔑Aspergilloma = Air crescent around a round ball. Fungus colonizes a pre-existing cavity (old TB, old sarcoid). The ball (mycetoma) moves when the patient changes position. Air crescent wraps around the top. Air-fluid level is a flat line. Completely different shape.
The clinical timeline distinguishes abscess from cancer. Abscess: 1-3 weeks, fever, foul sputum. Cancer: 3+ months, weight loss, no fever, no foul odor. 🔑Infection: fast onset, fever, smells, responds to antibiotics. Cancer: slow onset, weight loss, no smell, does not respond to antibiotics. When the "abscess" does not improve after 2-3 weeks of antibiotics, get bronchoscopy. You may be treating a malignancy.
Lung abscess from aspiration during a dental procedure = polymicrobial oral anaerobes. NOT a single organism like Strep pneumo. 🔑Aspiration abscess cultures grow "mixed oral flora." This confuses students who expect a single named organism. The whole point is that the flora from dental plaque, gum disease, and tonsillar crypts all land together. It is always polymicrobial.
PCP is bilateral and does not cavitate. It is ground-glass, not holes. 🔑PCP = Pervasive haze, not holes. Bilateral diffuse ground-glass on CXR (frosted glass appearance). No cavity. If you see a cavity in an HIV patient, think TB or cryptococcus or aspergillus, not PCP. LDH is elevated (nonspecific marker of injury).
Prolonged antibiotic therapy means 4-6 weeks. Clinical improvement within 1-2 weeks means you have the right drug. 🔑Lung abscess demands patience. The cavity fills with pus, the walls need time to heal, the anaerobes are entrenched. But you should see fever breaking and sputum improving in the first 1-2 weeks. No improvement at 2 weeks = wrong antibiotic or wrong diagnosis (cancer, resistant organism).
The right lower lobe basal segments are the landing zone when aspiration happens upright. The superior segment of the RLL is the landing zone when supine. 🔑Upright: basal segments = gravity pulls material straight down into dependent segments. Supine: superior RLL or posterior RUL = those segments face downward (become gravity-dependent) when lying flat. Gravity always picks the landing zone. The right bronchus always wins.
A parapneumonic effusion or empyema can complicate lung abscess. Empyema is pus in the pleural space, NOT in the lung. 🔑Abscess is inside the lung parenchyma. Empyema is between the lung and the chest wall (pleural space). They look different on imaging: abscess has a round cavity inside the lung, empyema has fluid following the pleural contour. Empyema requires chest tube drainage, not antibiotics alone.
CLINICAL IMAGES
Real pathology. Tap any image to expand.


PROVE IT
5 patients just walked in smelling terrible. Don't let them down.