The reversible one vs the one that gave up trying
A 55-year-old with 30 pack-years presents with chronic dyspnea and wheezing. PFTs show FEV1/FVC < 0.7. After albuterol, FEV1 improves by 8%.
Asthma or COPD?
These two diseases both cause airflow obstruction and wheezing. That's where the similarity ends. Flip between tabs · notice how different the stories are.
Young. Often childhood onset. Atopic history · eczema, allergic rhinitis, food allergies. Family history of asthma. The kid who couldn't run the mile in gym class.
Eosinophilic inflammation → bronchial hyperreactivity → airway smooth muscle spasm → reversible obstruction. The airways are twitchy, not destroyed.
REVERSIBLE. Give albuterol → FEV1 jumps ≥12% AND ≥200mL. The airways open back up because the walls are still intact. They're just spasming.
Inhaled corticosteroids (ICS) are the controller. SABA for rescue. Step up with LABA + ICS combo. The goal is no symptoms · and that's actually achievable.
Older smoker. Usually 40+ with significant smoking history. The guy who smoked a pack a day for 30 years and now can't climb stairs.
Neutrophilic inflammation → protease-antiprotease imbalance → alveolar wall destruction (emphysema) + mucus gland hypertrophy (chronic bronchitis). The architecture is permanently damaged.
IRREVERSIBLE. Give albuterol → FEV1 improves <12% or <200mL. The obstruction is structural. You can't relax a wall that's been demolished.
LAMA (tiotropium) is the first-line controller. Add LABA. ICS only added for frequent exacerbations (≥2/year). Smoking cessation is the ONLY thing proven to slow decline. O2 if PaO2 ≤55.
One screen. All the differences. Lead with what's DIFFERENT, not what's shared.
Three airway disorders. Each one presents differently and demands a different fight. Tap a card to flip it.
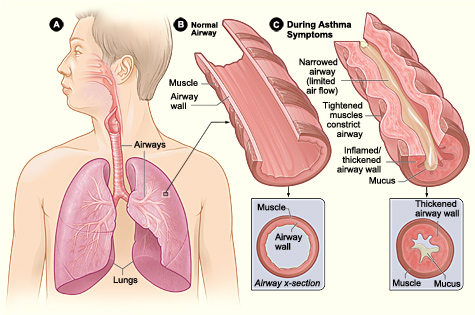 Asthma Airway
Asthma Airway
 Emphysema
Emphysema
 Barrel Chest
Barrel Chest
 Spirometry
Spirometry
Who: Young, atopic. Eczema, allergies, family history.
Cell: Eosinophils. IgE-driven Th2 inflammation. Mast cells fire, IL-5 summons eos.
Key: REVERSIBLE. FEV1 improves ≥12% AND ≥200mL post-albuterol.
Triggers: Allergens, cold air, exercise, NSAIDs, viral URI.
Rx: ICS (controller) + SABA (rescue). Step therapy up to ICS/LABA combo.
PFTs: Normal between attacks. FEV1/FVC normalizes post-bronchodilator.
Who: Smoker, >40. Pack-years do the damage. A1AT deficiency = young non-smoker.
Cell: Neutrophils. Protease-antiprotease imbalance → alveolar destruction.
Key: IRREVERSIBLE. FEV1/FVC <0.7 always. Bronchodilator response <12%.
Subtypes: Pink puffer (emphysema, low BMI, hyperinflated) vs Blue bloater (chronic bronchitis, hypercapnic, edematous).
Rx: LAMA first. Add LABA. ICS only if ≥2 exacerbations/year. O2 if PaO2 ≤55. Smoking cessation = only proven mortality benefit.
Who: Older patient with asthma history who smoked, OR young smoker with partially reversible obstruction.
Spirometry: FEV1/FVC <0.7 (like COPD) but also shows ≥12% reversibility (like asthma). Both criteria met.
Inflammation: Mixed eosinophilic + neutrophilic. The two diseases collide.
Board trap: clinical medicine test clean patterns. Only call ACOS when they explicitly give BOTH disease features. If it looks like COPD, call COPD. If it looks like asthma, call asthma.
Rx: ICS + LABA (treat both components). More exacerbations, worse outcomes than either alone.
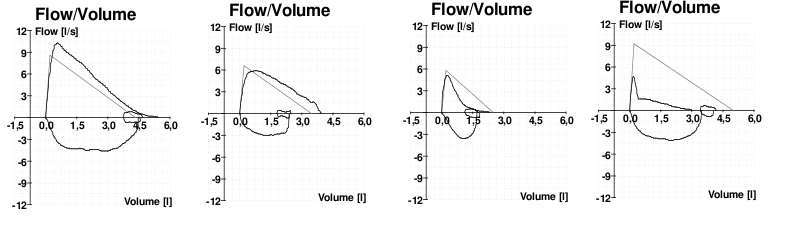
The shape of the expiratory limb tells you the diagnosis. Click a pattern to examine it.
clinical medicine shortcut: scooped = obstructive. Small = restrictive. Normal = neither. Click each button for the full breakdown.
The reference shape. Airways open fully, peak flow is high, exhalation is unrestricted. Memorize this first. Everything else is a deviation from it.
The concave scoop = small airways collapsing mid-exhalation, cutting off flow before the lungs are empty. FEF 25 to 75% is the most sensitive marker. In asthma, the curve normalizes with bronchodilator. In COPD, it does not.
Stiff lungs cannot expand, so TLC and FVC are both reduced. But once you start exhaling, airway patency is intact: FEV1/FVC stays normal or elevated. TLC below 80% predicted is the gold standard diagnostic criterion.
Board vignette drops. Patient is wheezing. Walk through it.
Five patients walk in wheezing. Don't give them the wrong inhaler.
Read every explanation, not just the correct answer.
Original clinical vignettes. Shuffled, never-repeat, full explanations for every choice.