Two numbers do most of the work. Girls before 8, boys before 9 = precocious. One cutoff, one decision tree, every board question.
first screen drill
Age, Axis, Action
Do the whole puberty workup in three moves: age cutoff, which endocrine axis is active, then the next clinical action. Tap a case and make the call before the long walkthrough.
tap a case
The page now opens with the clinical move.
Pick a scenario. The answer appears here as a chain: cutoff, axis, action.
A nearly 9-year-old girl is brought in for evaluation of a growth spurt. Parents say she's showing signs of puberty earlier than her siblings. She's at the 96th percentile for height and 98th percentile for weight. Physical exam: Tanner stage 1 pubic hair, Tanner stage 2 breast development. Sparse, soft axillary hair. The core driver is:
THE RULE
One Cutoff Decides Everything
Before you touch labs, imaging, or differentials, ask one question: how old is the kid? The age decides whether you have a problem or a normal child.
🔑Girls: puberty before age 8 = precocious. Age 8 to 12 = normal. Boys: puberty before age 9 = precocious. Age 9 to 14 = normal.🔑8 for girls, 9 for boys. Girls start a year earlier, just like in real life.
From the Attending
"Average puberty in America is 10 for girls, 11 for boys. Standard deviation, 1 year. Two SDs early: 8 for girls, 9 for boys. Before 8, before 9, that's precocious. Know your cutoffs."
The chain: signs of puberty → check age → above cutoff = normal variation → reassure, no workup. Below cutoff = precocious → start the algorithm.
The girl in the opener is almost 9. She's inside the 8 to 12 window. Her sequence is normal (breast first, then hair). She's just earlier than her siblings. That's variation, not pathology.
The Trap: "Earlier Than Siblings" Is a Red Herring
Board stems love "earlier than siblings" or "earlier than expected." Ignore it. The number is the only thing that matters. Same physical findings at age 9 = normal. Same findings at age 6 = full workup. Don't compare to family. Compare to the cutoff.
THE STAGES
Tanner Staging
Match the description to the number. Not the age. The description.
From the Attending
"How would you describe Tanner 3? What does it LOOK like? I don't care about the age. Tanner is a physical exam scale, not a calendar."
Trap word: "coarse." Coarse hair is Tanner 4, not Tanner 3. Tanner 3 is darker and curling. Tanner 4 is full adult texture, just not yet on the thighs. Every time.
Stage 1 · Prepubertal
Breast
Flat. No glandular tissue, no areolar elevation.
Pubic Hair
None. Just fine vellus hair, same as the abdomen.
Factory settings. Kid mode. Nothing has started.
Stage 2 · The First Sign
Breast
Breast buds. Small elevation. Areola starts to widen.
Pubic Hair
Sparse, soft hair along the labia or base of the penis. "One here, one here, one here."
Breast buds = FIRST sign in girls. Don't get fooled: in boys, the first sign is testicular enlargement (>4 mL or >2.5 cm), NOT pubic hair.
Girls' growth spurt starts here (Tanner 2, age 11 to 12). Boys are still catching up.
Stage 3 · The Patch
Breast
Breast and areola enlarge together. Single smooth contour, no separation yet.
Pubic Hair
Darker, curling, spreading. You can see a PATCH across the mons.
From the Attending
"Tanner 1: nothing. Tanner 2: sparse, one here, one here. Tanner 3: there's a PATCH. See a patch, that's a 3. Don't overthink it."
Boys' growth spurt starts here (Tanner 3 to 4, age 13 to 14). Two years behind the girls.
Stage 4 · Almost Adult
Breast
Areola and nipple project as a secondary mound above the breast surface. Bump within a bump.
Pubic Hair
Adult texture, full coverage of the mons or base of penis. Hasn't crossed onto the thighs yet.
Menarche lives at Tanner 4 (average age 12.5). The secondary mound is the hallmark finding. If the stem says "first period," picture Tanner 4 breasts.
Stage 5 · Adult
Breast
Mature. The Stage 4 secondary mound flattens back into the breast contour. Only the nipple projects.
Pubic Hair
Adult distribution. Spreads to the medial thighs or up onto the lower abdomen.
From the Attending
"Tanner 4 covers the base. Tanner 5 reaches the thigh or climbs onto the pelvis. That's the whole system. Description to number. Every time."
BOYS' GENITAL STAGING
Same five stages. Testes and penis instead of breasts. Volume by orchidometer is the key metric.
Stage 1 · Prepubertal
Genital
Testicular volume <4 mL. Long axis <2.5 cm. Prepubertal penis and scrotum.
Pubic Hair
None. Fine vellus hair only.
Nothing has started. Same as girls' Stage 1.
Stage 2 · The First Sign
Genital
Testicular volume 4 to 8 mL. Long axis 2.5 to 3.3 cm. Scrotum enlarges, thins, and may redden. Little or no penile change yet.
Pubic Hair
Sparse, downy hair at the base of the penis.
Testicular enlargement ≥4 mL = FIRST sign in boys. FSH stimulates Sertoli cells and seminiferous tubules first. The engine turns over before the wheels move.
Stage 3 · Growth Begins
Genital
Testicular volume 9 to 12 mL. Long axis 3.4 to 4.0 cm. Penis enlarges, mainly in length.
Pubic Hair
Darker, coarser, more curled. Spreads over the pubic junction.
Peak height velocity starts here (Tanner 3 to 4, age 13 to 14). Two years behind the girls.
Stage 4 · Nearly Adult
Genital
Testicular volume 15 to 20 mL. Long axis 4.1 to 4.5 cm. Penis increases in length AND breadth. Glans develops. Scrotal skin darkens.
Pubic Hair
Adult-type hair over the pubic region but not yet to medial thighs.
Spermarche lives here (Tanner genital 4). First sperm production. Also when pubertal gynecomastia typically peaks (Tanner 3 to 4).
Stage 5 · Adult
Genital
Adult genitalia. Testicular volume >20 mL. Long axis >4.5 cm.
Pubic Hair
Adult escutcheon. Spreads to medial thighs.
Orchidometer pearl: small, firm testes in a tall teen = think Klinefelter. Large testes (>30 mL) post-puberty + intellectual disability = think Fragile X. Size AND texture matter.
THE SEQUENCE
Normal Order of Puberty
Puberty plays in a fixed order. Out-of-order = pathology, even if the age is normal. Hair before breasts in a girl? That's not late thelarche. That's an androgen source (adrenal tumor, CAH) until proven otherwise.
📋Girls: Thelarche (breast buds) → Growth spurt → Pubarche (pubic hair) → Menarche (first period)🔑Thelarche first, Menarche last. Estrogen drives the show, hair just tags along.
📋Boys: Testicular enlargement (>4 mL) → Scrotal changes → Penile growth (length first) → Pubic hair → Growth spurt (Tanner 3 to 4) → Voice deepening, facial hair → Spermarche (Tanner 4)🔑Testes first. Voice and facial hair are LATE. Spermarche at Tanner 4, same stage as menarche in girls.
📋Girl pearl: Physiologic leukorrhea (white vaginal discharge) appears 6 to 12 months before menarche. Rising estrogen stimulates cervical mucus. Normal finding, not an infection. If the stem describes a pubertal girl with non-foul white discharge, reassure.
From the Attending
"First sign in a girl: breast bud. First sign in a boy: balls get bigger. Not pubic hair. The clinical medicine will try to fool you with hair, every time. Don't fall for it. Hair is adrenal. The first real puberty sign is gonadal."
BARS SHOW TYPICAL AGE RANGE
WHEN IT'S TOO EARLY
Precocious Puberty
Puberty before 8 (girls) or 9 (boys). One question runs the whole workup: is the brain driving this, or is something else making hormones on its own?
The chain: too-early signs → LH/FSH → GnRH stim test. The stim test answers the central vs peripheral question with one injection.
From the Attending
"See precocious puberty, the next question is always the same: central or peripheral? Brain's switch flipped early, or is something out there making the hormone on its own? That fork drives the whole differential."
Central (GnRH-Dependent)
Peripheral (GnRH-Independent)
Where
HPG axis flipped on early. Brain is driving it.
Hormones come from outside the axis. Tumor, adrenal, exogenous.
LH/FSH
High (pituitary fully active)
Suppressed (axis shut down by hormone flood)
GnRH stim
LH surges
LH stays flat
Sequence
Normal order, just early
Off-sequence (isolated breast or isolated hair)
#1 cause
Idiopathic (girls). CNS lesion / hamartoma (boys, until proven otherwise).
Leuprolide. Continuous GnRH agonist desensitizes the pituitary.
Treat the source. Remove tumor, stop exposure, block enzyme.
From the Attending
"One injection tells you everything. GnRH only talks to the pituitary. It can't reach a tumor in the ovary or the adrenal. So if the shot makes LH jump, the pituitary is awake and primed. Central. If the shot does nothing, the pituitary is asleep because something else is doing the work. Peripheral. Find the source."
The GnRH Test, Translated
LH rises after GnRH → pituitary is primed → Central PP → MRI brain, then leuprolide. LH stays flat after GnRH → pituitary is suppressed → Peripheral PP → DHEAS, 17-OHP, hCG, ovarian/adrenal imaging. Treat the source.
Sex-Specific Default
Girl with central PP: 90% idiopathic. MRI usually clean. Boy with central PP: assume CNS lesion (hypothalamic hamartoma is classic) until MRI proves otherwise. Boys with early puberty get their brain imaged.
🧠Brain MRI indications (know these cold): 1. ALL boys with central precocious puberty. 2. Girls younger than 6 with precocious puberty. 3. Any child with neurologic symptoms (headache, vision change, vomiting).🔑Boys always get MRI. Girls only if <6 or neuro symptoms. Girls 6 to 8 with idiopathic CPP usually skip MRI.
The Van Wyk-Grumbach Exception
Severe longstanding hypothyroidism can mimic precocious puberty. Massive TSH cross-reacts with the FSH receptor → ovarian stimulation, breast development, vaginal bleeding, ovarian cysts. The unique board pearl: bone age is DELAYED, not advanced. Every other cause of PP advances bone age. Van Wyk-Grumbach is the one exception. TSH is sky-high, T4 is in the gutter. Thyroid replacement reverses everything.
INTERACTIVE
GnRH Stimulation Test Simulator
Same shot, two patients. Watch what the LH curve tells you.
Before the shot: which patient should make a big LH surge?
Exactly. Central precocious puberty means the brain-pituitary axis is already awake, so one GnRH pulse triggers LH release. Peripheral precocious puberty keeps LH flat because sex hormone feedback has shut the pituitary down.
Central PP
Brain is driving puberty. Pituitary primed and answering.
💡One shot, one answer. LH surge >5 to 8 IU/L = pituitary is awake = central. Flat LH = pituitary is suppressed by a hormone source it doesn't control = peripheral. The pituitary only answers if it's been talking to GnRH already.
CHALLENGE
Sort: Central or Peripheral?
Tap a card, then tap the bin where it belongs.
Central PP
Peripheral PP
THE LINEUP
Puberty Disorders
Tap to expand.
🧠
Central Precocious Puberty
GnRH-dependent
Clue: Girl <8 or boy <9 with normal sequence (just early).
Mechanism: Brain flipped the switch ahead of schedule. Hypothalamus → GnRH → LH/FSH → gonads.
Labs: LH and FSH pubertal. LH surges after GnRH stim.
#1 cause: Girls = idiopathic. Boys = CNS lesion (hypothalamic hamartoma) until MRI says otherwise.
Rx: Leuprolide. Continuous GnRH agonist desensitizes the pituitary → LH/FSH drop → puberty pauses until age-appropriate.
🏈
Peripheral Precocious Puberty
GnRH-independent
Clue: Off-sequence puberty (isolated breast or isolated hair, virilization in a girl, etc.).
Mechanism: Sex hormones from outside the HPG axis → flood → pituitary shuts off in negative feedback.
Bonus: May also see hyperthyroidism, Cushing's, GH excess, hyperphosphatemia. Any Gs-driven gland is fair game.
Board pearl: Fracture + early puberty + jagged cafe au lait = McCune-Albright.
⏰
Constitutional Delay
#1 cause of delayed puberty
Clue: No signs by 13 (girls) or 14 (boys), short for age, plus a parent who was a "late bloomer."
Mechanism: Normal variant. HPG axis is fine, just clocking late.
Bone age: Delayed. Matches the kid's developmental stage, not the birthday.
Labs: LH, FSH, testosterone all low, but appropriate for the bone age.
Discriminator:Smell is normal. That rules out Kallmann.
Rx: Reassure. Short course of testosterone or estrogen if psychosocial distress.
👃
Kallmann Syndrome
Can't smell, can't puberty
Clue: Teen with no puberty AND anosmia (can't smell coffee, gasoline, mint).
Mechanism: GnRH neurons share an embryonic origin with olfactory neurons. They fail to migrate from the nose to the hypothalamus together → no GnRH AND no smell.
Labs: Low LH, low FSH, low sex steroids (hypogonadotropic hypogonadism).
MRI: Hypoplastic or absent olfactory bulbs.
Board pearl: Always ask about smell in delayed puberty. Anosmia + no puberty = Kallmann. Every time.
🔪
Turner Syndrome
45,XO
Karyotype: 45,XO (one X missing).
Body: Short, webbed neck, shield chest with wide-spaced nipples, cubitus valgus, lymphedema of hands and feet at birth.
Gonads: Streak ovaries → primary amenorrhea → no estrogen → no puberty.
Cardiac: Bicuspid aortic valve, coarctation of the aorta.
Renal: Horseshoe kidney.
Labs:High FSH/LH (hypergonadotropic). Pituitary screaming at gonads that never answer.
Rx: GH for height. Estrogen + progesterone for puberty.
👀
Klinefelter Syndrome
47,XXY
Karyotype: 47,XXY (one extra X).
Body: Tall, long limbs, gynecomastia, sparse facial/body hair, small FIRM testes.
Mechanism: Extra X scars the seminiferous tubules → tubules fibrose → testes feel firm AND can't make sperm. Leydig cells fail too → low testosterone.
Labs: Low testosterone, high FSH/LH (hypergonadotropic), azoospermia.
Board pearl: Tall teen with gynecomastia and small firm testes → karyotype. Don't biopsy first.
Rx: Testosterone replacement. Fertility is very limited.
🌞
Premature Thelarche
Just the breasts, nothing else
Clue: Girl <8 with isolated breast development. Tanner 1 hair. Normal growth velocity.
Mechanism: Brief, low-grade estrogen pulse. Often bilateral, sometimes asymmetric. Benign variant.
Bone age: Normal (this is the test that rules in benign).
Rx: Reassure. Re-check every 6 months. If hair, growth spurt, or rapid progression appear → restart the precocious puberty workup.
Pearl: One sign = benign. Two signs = investigate.
🪝
Premature Adrenarche
Just the hair, nothing else
Clue: Pubic or axillary hair, body odor, mild acne before 8 (girls) or 9 (boys). No breast, no testicular growth.
Mechanism: Adrenal zona reticularis turns on early → DHEAS rises → hair follicles activate. Gonadal axis stays quiet.
Bone age: Normal or just slightly advanced.
Rule out: Non-classic CAH. Check 17-OHP.
Rx: Reassure once CAH is excluded. Benign, but flag obesity and insulin resistance risk later.
🙏
Androgen Insensitivity
46,XY + breasts + no hair
Karyotype: 46,XY. Phenotypically female.
Mechanism: Androgen receptor is broken. Testes make testosterone, but the body can't hear it. Testosterone aromatizes to estrogen → breast development. No androgen action → scant pubic/axillary hair.
Anatomy: Testes present (inguinal or intra-abdominal). No uterus (AMH destroyed Mullerian ducts). Blind-ending vaginal pouch.
Presentation: Primary amenorrhea in a girl with breasts but no body hair. Inguinal masses on exam.
Rx: Let endogenous estrogen finish puberty. Gonadectomy AFTER puberty (2 to 3% gonadoblastoma risk). Lifelong estrogen replacement.
🔬
5-Alpha-Reductase Deficiency
Virilizes at puberty
Karyotype: 46,XY. Undervirilized external genitalia at birth (often raised female).
Mechanism: Cannot convert testosterone to DHT. DHT drives external male genitalia in utero. At puberty, rising testosterone (which doesn't need 5-AR for muscle, voice, phallus growth) causes virilization.
Clue: "Girl" who virilizes at puberty. Phallic enlargement, voice deepening, muscle growth. Testes descend.
Internal structures: Normal. AMH is intact, so Mullerian ducts regressed. Wolffian ducts developed (testosterone works for those).
Board pearl: Phenotypic female at birth who masculinizes at puberty = 5-AR deficiency until proven otherwise.
💜
Mullerian Agenesis
MRKH: breasts + no uterus + normal hair
Karyotype: 46,XX. Normal ovaries. Normal secondary sexual characteristics.
Problem: Mullerian ducts failed to develop → absent uterus, absent upper vagina. Ovaries are NOT Mullerian, so they work fine.
Presentation: Primary amenorrhea in an otherwise normal girl with breasts AND normal pubic hair.
Discriminator: Normal pubic hair separates MRKH from AIS. AIS has scant hair (broken androgen receptor). MRKH has normal hair (working androgens, just no uterus).
Clue: Adolescent girl with normal puberty, cyclic pelvic pain, no visible menses. Bulging bluish membrane at introitus.
Mechanism: Menstrual blood accumulates behind the imperforate membrane → hematocolpos (blood filling the vagina), then hematometra (filling the uterus).
Imaging: Pelvic US shows fluid-filled vagina and uterus.
When: Tanner genital stages 3 to 4. Up to 65% of boys get transient breast tissue during normal puberty.
Mechanism: Transient estrogen/androgen imbalance as the HPG axis ramps up. Testosterone aromatizes to estrogen before full androgen levels stabilize.
Resolves: Usually within 6 to 18 months. Self-limited.
Red flags: Persists >24 months, progressive, painful, or occurs WITHOUT other pubertal progression. Evaluate: Klinefelter, prolactinoma, estrogen-secreting tumor, drug effect (spironolactone, marijuana).
Board pearl: Bilateral, non-tender, Tanner 3 to 4 = reassure. Unilateral, firm, fixed = image it.
🧬
Fragile X
Macroorchidism after puberty
Clue: Post-pubertal male with intellectual disability + large testes (macroorchidism) + long face + prominent ears.
Mechanism: FMR1 gene CGG repeat expansion on the X chromosome. Silences FMRP protein needed for synaptic development.
Testes: Enlarged AFTER puberty (>30 mL), unlike Klinefelter which has SMALL testes. That's the discriminator.
Carrier effect: Female premutation carriers are at risk for primary ovarian insufficiency (premature menopause <40).
Board pearl: Big testes + intellectual disability = Fragile X. Small firm testes + tall + gynecomastia = Klinefelter. Size and texture of the testes split them.
ALGORITHM
Decision Tree: Evaluating Early Puberty
Tap through the steps.
Signs of puberty before age 8 (girls) or age 9 (boys)?
Normal development. Reassure. Check Tanner stage for sequence.
Get bone age. Is it advanced?
GnRH stimulation test: does LH rise?
Central PP. MRI brain. Treat with leuprolide.
Peripheral PP. Check DHEAS, 17-OHP, hCG. Treat the source.
Check FSH and LH levels
Constitutional delay OR hypogonadotropic (Kallmann, tumor, chronic illness). Family history: constitutional. Anosmia: Kallmann.
Primary gonadal failure (hypergonadotropic). Turner 45X in girls, Klinefelter 47XXY in boys. Get karyotype.
GROWTH MECHANICS
Hormones, Bone Age & Growth Plates
VOCABULARY
Adrenarche · adrenal androgens (DHEA/DHEAS) turn on → pubic/axillary hair, body odor, acne. Runs on its own track. Brain not required.
Gonadarche · pituitary FSH/LH wake up the gonads. This is the real start of puberty.
Thelarche · first breast development. First gonadarche sign in girls. Tanner 2.
Pubarche · first pubic hair. Adrenal product. Can run ahead of or behind gonadarche.
Menarche · first period. Tanner 4, average age 12.5. Late event, never the first sign.
Spermarche · first sperm production/ejaculation. Tanner genital stage 4 in boys. Equivalent milestone to menarche in girls.
Mini-puberty · brief HPG axis activation in infancy (first 6 months). Transient breast tissue in girls, penile/testicular changes in boys. Exam trap: this is NOT pathologic precocious puberty. Self-resolves by age 1 to 2.
Physiologic leukorrhea · white, non-foul vaginal discharge that appears 6 to 12 months before menarche. Rising estrogen stimulates cervical mucus. Normal. Not an infection.
From the Attending
"Two engines, two tracks. The brain-gonad axis makes thelarche, menarche, testes. The adrenal axis makes hair, odor, acne. They normally run together, but they can run apart. Isolated hair? Think adrenal. Isolated breast? Think gonadal or estrogen exposure. Know which engine you're looking at."
PEAK HEIGHT VELOCITY BY TANNER STAGE
Group
Peak velocity
Tanner
Age
Girls
8 to 9 cm/yr
Tanner 2 to 3
11 to 12
Boys
9 to 10 cm/yr
Tanner 3 to 4
13 to 14
Why men end up taller: the spurt is only slightly bigger, but it starts ~2 years later. Those 2 extra years of pre-spurt growth before the plates close are the entire difference.
GROWTH PLATE FUSION
Long bones grow at the epiphyseal plate (cartilage disc between metaphysis and epiphysis). Sex hormones close that plate by killing the chondrocytes and replacing cartilage with bone.
Estrogen closes plates. In BOTH sexes. Testosterone matters mostly because aromatase converts it to estrogen at the plate. Aromatase-deficient men keep growing into their 20s → tall stature, eunuchoid proportions. That's the proof.
Most long-bone plates close: girls 15 to 16, boys 17 to 18.
Hand & wrist (read for bone age): fused by 16 (girls) / 18 (boys).
Clavicle, iliac crest: last to fuse (mid-20s).
Board stem trap: precocious puberty kid looks tall today. Without leuprolide, plates close early → short adult. Treating them protects adult height.
BONE AGE VS CHRONOLOGICAL AGE
Bone age = left-hand-and-wrist X-ray, compared to the Greulich-Pyle atlas. It tells you how mature the skeleton is, not how many birthdays the kid has had.
Why it matters: bone age tracks hormone exposure. Hormone signal advances the skeleton. So bone age vs chronological age is a direct readout of "how much sex steroid has this kid been seeing?"
From the Attending
"Bone age two standard deviations above chronologic age. What does that tell you? Those bones are being driven. He's too young to have that much hormone on board. Something is making sex steroids that shouldn't be there yet. The X-ray caught it."
Bone age > chronological age: too much hormone, too early. Precocious puberty, CAH, McCune-Albright, exogenous exposure.
Bone age < chronological age: not enough hormone. Constitutional delay, hypogonadism, GH deficiency, chronic disease, malnutrition.
Bone age = chronological age: on schedule. Isolated premature thelarche / adrenarche live here.
VISUAL REFERENCE
Clinical Images & Cafe Au Lait Discriminator
McCune-Albright: irregular cafe au lait ("coast of Maine")
Turner syndrome: webbed neck (pterygium colli)
Human chromosomes XXY: Klinefelter 47,XXY karyotype
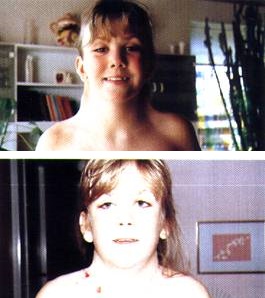
Gynaecomastia: pubertal and Klinefelter comparison clue
Polyostotic fibrous dysplasia: McCune-Albright bone lesion
DISCRIMINATOR
Coast of Maine vs Coast of California
Same color spot. Border shape splits two completely different diseases.
Coast of Maine
Jagged, irregular borders. Few large lesions. Rocky Maine coastline.
McCune-Albright
Coast of California
Smooth, rounded borders. Often many lesions (≥6, each >5 mm prepubertal). Sandy California coast.
Neurofibromatosis 1
From the Attending
"Big hyperpigmented patches with jagged borders, plus fractures, plus early puberty? McCune-Albright. Six or more smooth-bordered spots, plus axillary freckling, plus a Lisch nodule on slit lamp? That's NF1. Same color, different border, different disease. Know your clues."
WHEN IT'S TOO LATE
Delayed Puberty
The mirror image of precocious puberty. The HPG axis should have fired by now. It hasn't. One question runs the whole workup: is the clock just running slow, or is something actually broken?
🔑Girls: no breast development by age 13 = delayed. Boys: no testicular enlargement (≥4 mL) by age 14 = delayed. Girls: no menarche by 15, or >3 years after thelarche = evaluate.🔑Precocious: 8 girls, 9 boys. Delayed: 13 girls, 14 boys. Both sets are one year apart.
From the Attending
"Precocious puberty: before 8, before 9. Delayed puberty: no breast by 13, no testes by 14. Two sets of numbers. Know them cold. The most common cause of delayed puberty? Constitutional delay. More common in boys. Dad was a late bloomer. That's your #1 answer."
Constitutional Delay
Hypogonadotropic
Hypergonadotropic
Where
Normal variant. Clock is slow, all parts work.
Brain/pituitary not sending the signal.
Gonads not responding to the signal.
LH/FSH
Low, but appropriate for bone age.
Low (brain is quiet).
High (pituitary screaming at dead gonads).
Bone age
Delayed (matches developmental stage).
Delayed or normal.
Normal or delayed.
Smell
Normal.
Absent in Kallmann.
Normal.
Examples
Late-bloomer dad. Short today, normal adult height.
Reassure. Short testosterone/estrogen course if psych distress.
Treat cause. Replace sex steroids.
Replace sex steroids. GH for Turner.
Red Flags Against Constitutional Delay
Constitutional delay is #1, but clinical medicine love to test the exceptions. Flags that push you to investigate further: anosmia (Kallmann), dysmorphic features (Turner/Klinefelter), chronic disease symptoms, weight loss or low BMI, growth failure off the familial curve, prior CNS radiation or tumor, neurologic symptoms. If any red flag is present, don't stop at "late bloomer."
💡The gonadotropin direction tells you everything. Low LH/FSH = brain problem (constitutional, Kallmann, pituitary). High LH/FSH = gonad problem (Turner, Klinefelter, gonadal injury). Read the direction first, then narrow.🔑Low gonadotropins = brain isn't asking. High gonadotropins = brain is asking, gonads aren't answering.
From the Attending
"Think of FSH and LH as the pituitary yelling at the gonads. If the gonads are dead (Turner, Klinefelter), the pituitary yells LOUDER. FSH and LH go sky-high. If the brain never sent the signal (Kallmann, constitutional), the pituitary is quiet. FSH and LH stay low. Direction of the gonadotropins. Every time."
THE WORKUP
Primary Amenorrhea
No period by 15. Or no period >3 years after thelarche. Or no pubertal development by 13.
Step zero: pregnancy test. Always. Then the algorithm branches on one question: are secondary sexual characteristics present?
Primary amenorrhea: are secondary sexual characteristics present?
"Primary amenorrhea algorithm: breasts or no breasts. No breasts? High FSH means dead ovaries, low FSH means the brain never asked. Breasts present? Check for a uterus. No uterus plus no hair equals AIS. No uterus plus hair equals Mullerian agenesis. Uterus plus pain equals outflow obstruction. Three branches. That's the whole tree."
AIS vs Mullerian Agenesis: The Hair Splits It
Both have breasts. Both have no uterus. Both present as primary amenorrhea. The discriminator: pubic hair. AIS (46,XY) has scant or absent pubic hair because the androgen receptor is broken. Mullerian agenesis (46,XX) has normal pubic hair because androgens work fine. Same presentation, one detail separates them.
medical education
Clinical Walkthrough
34 clinical vignettes. One at a time. Tap each teaching beat to reveal the chain.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.
 McCune-Albright: irregular cafe au lait ("coast of Maine")
McCune-Albright: irregular cafe au lait ("coast of Maine")
 Turner syndrome: webbed neck (pterygium colli)
Turner syndrome: webbed neck (pterygium colli)
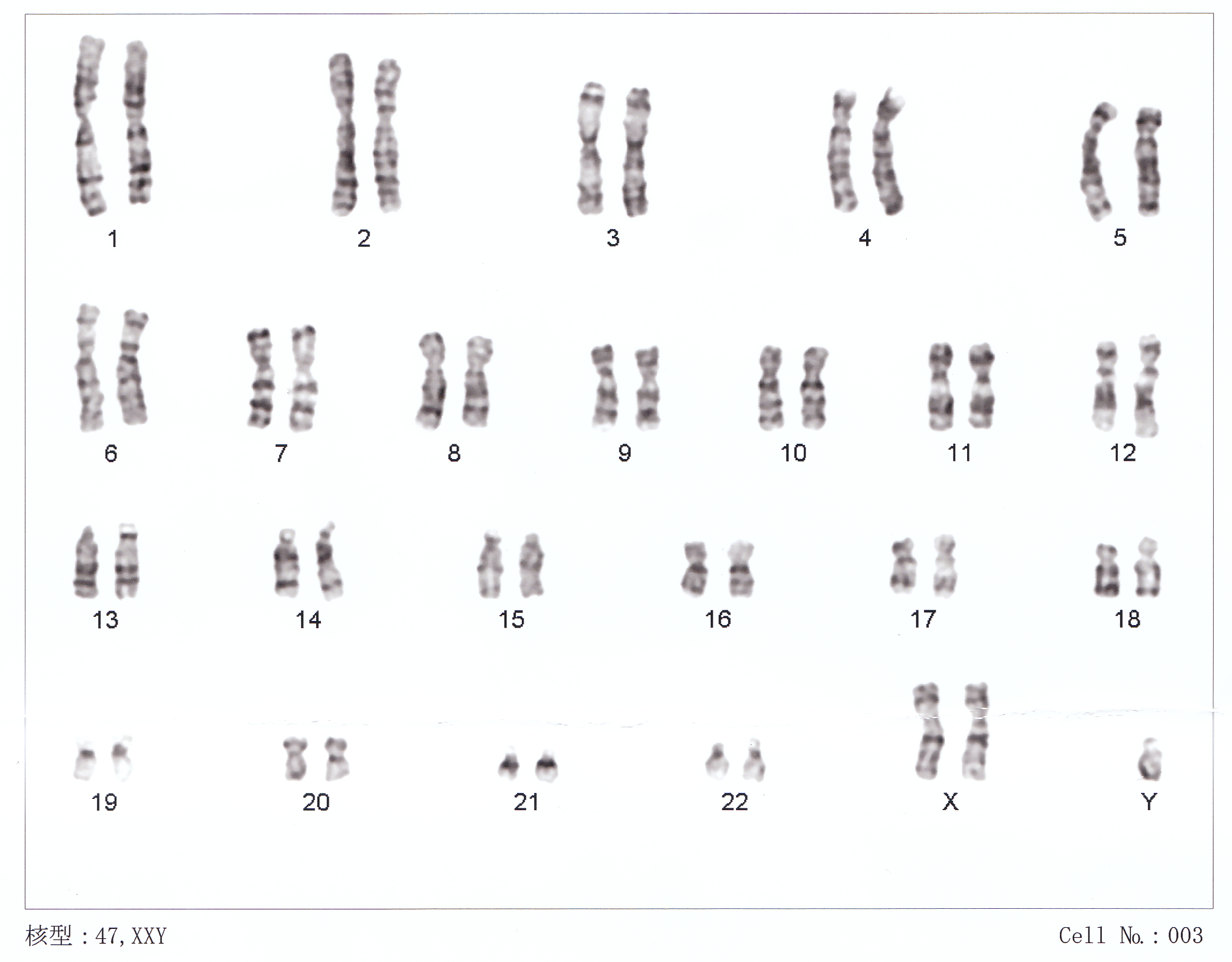 Human chromosomes XXY: Klinefelter 47,XXY karyotype
Human chromosomes XXY: Klinefelter 47,XXY karyotype
 Gynaecomastia: pubertal and Klinefelter comparison clue
Gynaecomastia: pubertal and Klinefelter comparison clue
 Polyostotic fibrous dysplasia: McCune-Albright bone lesion
Polyostotic fibrous dysplasia: McCune-Albright bone lesion