A toddler shows up with one tender, red, swollen node under the jaw. Five answer choices, and four of them are correct, for a different patient. Learn to read the stem's fingerprints so the same neck lump never fools you twice.
Section 1 of 4 · Pattern Lock
The Hot Node vs Its Lookalikes
Acute unilateral cervical lymphadenitis is a young child with one tender, warm, red, swollen node that blew up over hours to a couple of days. The bug is almost always Staph aureus or group A strep. Everything else that looks like a neck node moves on a different clock. Read the clock first.
A 3-year-old has a single tender, warm, red node under the right jaw that appeared two days ago. He is febrile but otherwise well. There is no fluctuant soft center, no recurrent-abscess history, no penicillin allergy, and no kitten at home.
Before you pick a drug, what does the tempo tell you the bug is?
Bilateral viral reactive nodes
Pyogenic bacteria: staph or strep
Cat-scratch (Bartonella)
Atypical mycobacteria
Route
Skin or oropharynx seeds a draining node; the node inflames and swells fast.
Pattern
Hours to days = pyogenic. Weeks and non-tender = Bartonella or atypical mycobacteria. Bilateral with a cold = viral.
Pearl
Tempo is the fingerprint. The faster and hotter the node, the more it screams staph and strep, and the more an antibiotic has to cover both.
Clinical Images
📷 Enlarged cervical node · tap to expand
📷 Staph aureus, Gram stain · tap to expand
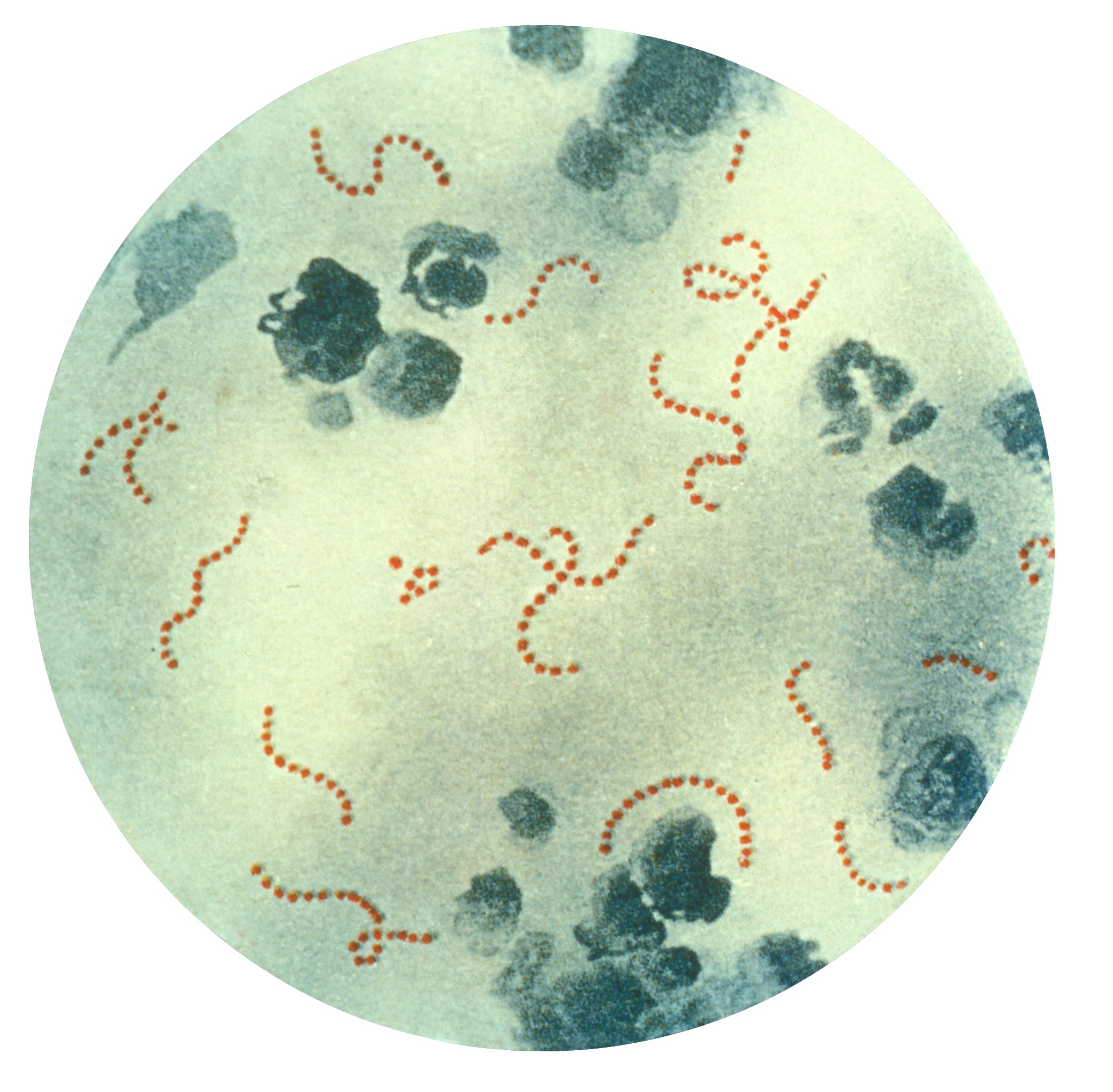
📷 Group A strep chains · tap to expand
Section 2 of 4 · The Coverage Map
Does Your Drug Cover What the Stem Forces You To?
Every drug covers a set of bugs. Every stem forces you to cover a set of bugs. The right answer is the drug whose coverage contains the stem's demand. Tap a drug to light its coverage, then answer the case.
Coverage
MSSA
MRSA
S. pyogenes
Oral anaerobes
Bartonella
Atypical myco
Fungal
Case check
The stem: acute hot node in a child with two prior MRSA abscesses and a penicillin allergy. This stem forces you to cover MRSA + group A strep. Pick a drug above, then ask the grid:
The grid is the whole game
You are not asked "is this a good antibiotic." You are asked "does its column light up where the stem demands." A great drug with a dark cell in the demanded column is a wrong answer.
Section 3 of 4 · The Head-to-Head
Clindamycin vs Amoxicillin-Clavulanate
Same syndrome. Same neck. The answer swings on one clue the stem plants. Tap the flags in the stem and watch the recommendation flip live.
Flags tapped: 0
A young child with an acute unilateral hot node. Tap what you see:
recurrent MRSA abscesses,
visible pus and fluctuance,
penicillin allergy,
high local MRSA rates,
dental caries and poor dentition.
Amoxicillin-clavulanate
No MRSA flag lit. A well child with an acute node, no resistance clues, is the amox-clav lane: MSSA (beta-lactamase covered), group A strep, and oral anaerobes in one drug.
Clindamycin = the MRSA and allergy key
Any MRSA flag OR a penicillin allergy, and you reach for clindamycin: it covers MRSA, group A strep, and anaerobes. Amox-clav does not touch MRSA, full stop.
Amox-clav = the mouth key
Dental or oropharyngeal source with no MRSA flag, and amoxicillin-clavulanate is the clean fit: it adds oral-anaerobe coverage on top of MSSA and strep, and the clavulanate handles beta-lactamase producers.
The question is never "good drug"
It is "which problem did the stem plant, resistance or source?" MRSA/allergy problem picks clindamycin. Mouth-source problem picks amox-clav.
Why the losers lose
Cefdinir
Covers group A strep and some MSSA, but staph coverage is unreliable and it hits zero MRSA. Boards use it as the plausible oral cephalosporin that quietly ignores the staph problem in a syndrome you cannot tell staph from strep clinically.
Azithromycin
Its node is the cat node: subacute, non-tender, kitten in the stem. Macrolide resistance in staph and strep makes it a poor pick for the acute hot node.
Its real lane: Bartonella / cat-scratch
Itraconazole
A fungal answer hunting a fungal stem: river-valley exposure, pulmonary or mediastinal disease, hepatosplenomegaly, chronic tempo. None of that is an acute tender neck node.
Its real lane: endemic fungal disease
Supportive care
Fits a small, minimally tender node in a well, afebrile child. It loses against a febrile child with a large, hot, painful node at risk of turning into pus.
Its real lane: the well, quiet node
Section 4 of 4 · Sort & Escalate
Sort the Mimics, Then Know When to Drain
Drag each mini-case into its tempo lane. Get all five right and the lane pattern locks. Then walk the drainage gate: pus does not answer to antibiotics.
Acute (hours to days)
Subacute (weeks)
Chronic (weeks+)
Decision tree · Node 1
The hot node now has a soft, fluctuant, pointing center. Child is febrile.
You started an oral antibiotic yesterday. On exam today your finger presses a spot that gives, like a grape under the skin.
Yes. Fluctuance means a walled-off pocket of pus. Antibiotics cannot penetrate a mature abscess reliably, so you drain it and keep the antibiotic. Fluctuant equals drain it; the abscess does not read the prescription.
Decision tree · Node 2
Different child: a chronic violaceous, minimally tender node over several weeks, child under 5, afebrile, overlying skin thinning.
You already gave a beta-lactam a week ago and nothing changed. The node has a dusky purple color the parents say has been there "forever."
Right. Chronic, violaceous, non-tender, in a child under 5, with skin thinning is the atypical (nontuberculous) mycobacterial picture. It does not answer to pyogenic antibiotics; the move is excision, not another beta-lactam. Violaceous and chronic means you left the pyogenic lane entirely.
The age-under-5 trap
Age under 5 alone does not turn an acute hot febrile node into atypical mycobacteria. The mycobacterial node is chronic and violaceous. Tempo and color override age.
The one-line summary
Acute hot tender node, cover staph + strep. MRSA flag or penicillin allergy, clindamycin. Dental source, no MRSA flag, amox-clav. Fluctuant, drain it. Slow, non-tender, exposure-driven, or chronic violaceous, you are in a different lane, so stop reaching for the pyogenic antibiotic.