Breast and Axilla Masses Read the Lump, Not the Panic
Anatomy and Pathology · Where Breast Lumps Hide
Breast and Axilla Masses Read the Lump, Not the Panic
Most breast and axilla lumps are benign. The board points hide in three forks: a mass that follows the milk line, discharge that names the duct, and a node at the apex that chokes a vein. Learn the map, and the differential reads itself.
Medically reviewed by Fatima Ali, DO and Kaitlyn Cocuzzo, MD
Before you scroll
A 28-year-old woman at 32 weeks of her first pregnancy comes to the office because of a new, soft, lumpy, sponge-like mass in the right axilla that was not there before she became pregnant. It is mildly tender, with no redness and no recent injury. On examination the fullness is doughy and poorly bordered, and a tiny extra nipple sits just below it. Ultrasound shows tissue that looks just like her normal breast. Which of the following is the most likely diagnosis?
Why is a node the tempting wrong answer?
A lump in the axilla makes everyone reach for lymph node first. But nodes are discrete, firm, and rounded, and a reactive node needs a reason (an infection or injury). She has none, and the mass is doughy and poorly bordered, not a marble you can roll.
What do the spongy feel and the extra nipple tell you?
Tissue that feels like breast, sits on a line below an accessory nipple, and looks like breast on ultrasound IS breast. The milk line runs from axilla to groin, and leftover breast tissue is most common in the axilla.
So why now, in pregnancy?
Accessory breast tissue carries the same hormone receptors as normal breast, so it swells when pregnancy and lactation hormones rise. That is why it appeared this trimester and not before. A new spongy axillary mass that grows in pregnancy, on the milk line with an extra nipple, is accessory breast tissue, not a node.
Scroll ↓ tap the anatomy map next
The Signature Game · Tap the Spot, Learn the Lump
The Milk Line and Axilla Map
One picture holds the whole topic. Tap the breast, the milk line, the axilla, or the apex under the clavicle. Each tap names what lives there and why it matters. This is the map behind every breast-and-axilla question.
Tap a glowing point
Start with the axilla: it holds the answer to the opener and to the venous trap further down.
Four points · tap each to build the whole map
From the Attending
One picture, three traps. A lump on the milk line that feels like breast is breast, not a node. A node at the apex sits on the vein, so it swells the arm. A mass in the breast is the differential you sort by feel and imaging. Learn where each one lives, and you stop guessing. Know your clues.
Pin 1 · The Lump That Follows a Line
Accessory Breast Tissue and the Milk Line
Why a brand-new axillary lump in pregnancy is breast tissue, not a node, and how the embryologic milk line gives it away.
The structure
The milk line runs from the axilla to the groin
In the embryo, a ridge of ectoderm (the mammary ridge, or milk line) runs down each side of the body from the armpit to the inner thigh. Normally one breast forms on each side and the rest of the ridge melts away.
When part of the ridge persists, you get an accessory nipple (polythelia) or accessory breast tissue (polymastia), and it can sit anywhere along that line. The most common spot is the axilla.
Straight line below the nipple. An extra nipple always sits in a vertical line under the normal one, never off to the side. That line IS the milk line.
Why it shows up in pregnancy
It carries hormone receptors, so it swells with the breast
Accessory breast tissue is real glandular breast tissue. It answers to estrogen, progesterone, and prolactin just like the normal breast.
That is why it can be silent for years, then enlarge, ache, or even leak milk during pregnancy and lactation. A new, soft, spongy axillary fullness in a pregnant patient that was absent before is the classic story.
An accessory nipple (polythelia) sitting along the milk line. The same milk line carries accessory breast tissue, most often in the axilla.
From the Attending
Do not confuse the lump that feels like breast with a node. A node is a firm marble with a reason behind it. Accessory tissue is a doughy field that matches the breast on ultrasound and sits on the milk line with an extra nipple. When a new spongy axillary mass grows in pregnancy, find the milk line. Every time.
Pin 3 · Five Groups, One Choke Point
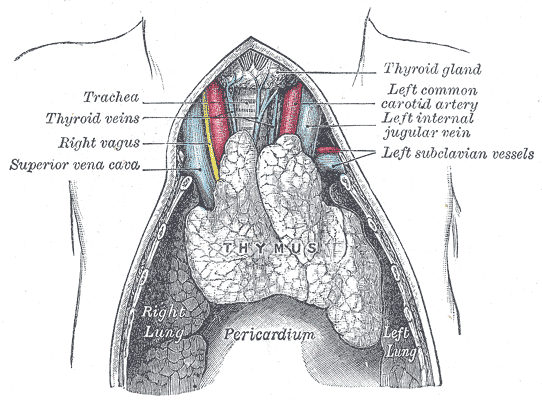
The Five Axillary Node Groups
Tap each group to see what it drains and where it sits. One of them rests on the axillary vein, so when it enlarges the whole arm swells. Find that one.
Lymphatics of the breast draining into the axillary node groups along the axillary vessels (anterior view).
🦴
Anterior (pectoral)
Anterior axillary wall
▼
Sits
Along the lateral thoracic vessels, deep to pectoralis major, on the anterior wall of the axilla.
Drains
The anterior chest wall and most of the breast.
Pearl
The first station for most breast cancer spread. Important for staging, but it is not the venous choke point.
🦴
Posterior (subscapular)
Posterior axillary wall
▼
Sits
Along the subscapular vessels on the posterior wall of the axilla.
Drains
The posterior chest wall and the scapular region.
Pearl
Back wall, back drainage. Far from the vein at the apex.
🦴
Lateral (humeral)
Along the vein, distal
▼
Sits
On the medial side of the axillary vein, lower down toward the arm.
Drains
Most of the upper limb.
Pearl
It drains the arm, but the whole-limb venous choke is higher up, at the apex, not here on the lateral wall.
🧭
Central
Axillary fat, the hub
▼
Sits
Embedded in the fat at the center of the axilla.
Drains
Receives from the anterior, posterior, and lateral groups, then forwards to the apex.
Pearl
The hub, and the group most often felt on exam. It is upstream of the choke, not the choke itself.
🔹
Apical (infraclavicular)
On the vein, under the clavicle
▼
Sits
At the apex of the axilla, pressed against the axillary vein where it dives under the clavicle to become the subclavian vein.
Drains
Receives from all the other groups, then empties into the subclavian lymphatic trunk.
Pearl
This is the choke. Because it sits on the vein at the outlet, bulky apical nodes compress upper-limb venous return, so the whole arm swells, worst just below the clavicle.
From the Attending
Five groups, but only one sits on the vein. The apical group is at the apex, right where the axillary vein passes under the clavicle to become the subclavian. So when a patient with breast cancer turns up with a swollen, heavy arm and distended veins, do not blame the heart first. Find the apical nodes squeezing the vein at the outlet. That distinction drives everything.
Pin 2 · The Stain With No Lump
Bloody Nipple Discharge
One duct, blood, no mass, no pain. Name it before you name cancer.
The number-one cause
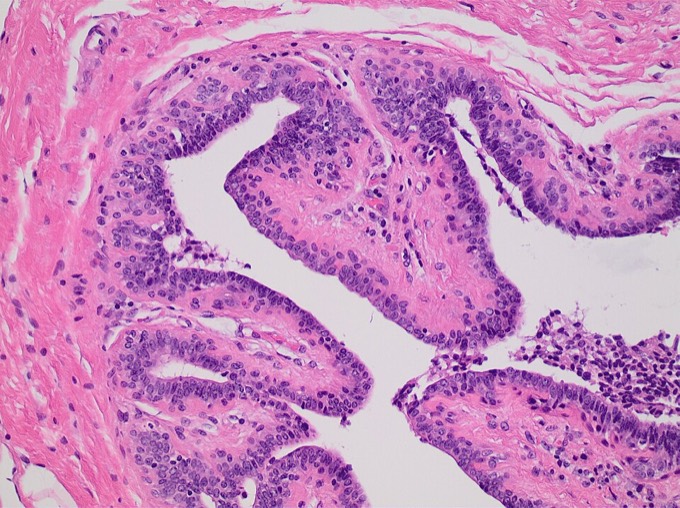
Intraductal papilloma
A benign papillary growth inside a single lactiferous duct. It is the most common cause of bloody nipple discharge, classically in a woman in her 30s to 50s.
The story: spontaneous, bloody or serosanguineous discharge from one duct, usually with no palpable mass and no pain. Imaging shows a small lesion inside a dilated duct.
One duct, no lump, benign. Single-duct bloody discharge with no mass is papilloma until proven otherwise.
Do not confuse it with
Intraductal carcinoma (ductal carcinoma in situ)
DCIS can also cause bloody discharge, but it leans older, and it tends to bring a mass or suspicious calcifications on mammography.
Because the two overlap, every bloody single-duct discharge is still worked up (imaging plus duct excision) to be sure. Papilloma is the most likely answer; ruling out cancer is the safe move.
Intraductal papilloma: benign fronds with fibrovascular cores filling a dilated duct. Fragile vessels in the fronds bleed, which is why the discharge is bloody.
From the Attending
A patient drips blood from one duct and there is no lump. Your gut yells cancer. Slow down. The most common cause is a benign papilloma, and the fragile little vessels in its fronds are what bleed. You still image and excise to be safe, but the name on the board is papilloma. Find the source, then prove it.
The Differential · Five Lumps, One Feel Each
The Breast Mass Lineup
Tap a tab. Each mass has one signature feel, one signature patient, and one imaging clue. Learn the pattern, not the paragraph.
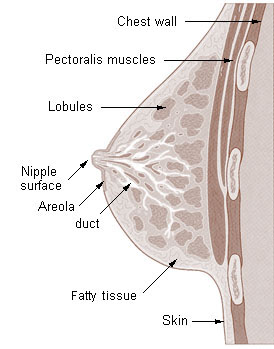
Normal breast: lobules and ducts in a fat and stromal bed. Each benign mass arises from one of these parts.
Benign · most common in the young
Fibroadenoma
Patient
Woman under 35
Feel
Smooth, rubbery, freely mobile
Imaging
Well-defined oval, hypoechoic, wider-than-tall
Behavior
Hormone-responsive, often stable
The classic breast mouse: it slips under your fingers because it is well-encapsulated. Mobile and rubbery in a young woman equals fibroadenoma.
Fibroadenoma: a well-circumscribed, rubbery, lobulated mass that shells out cleanly. The smooth border is why it feels mobile.
Benign · fluid-filled
Simple cyst
Patient
Often 35 to 50, perimenopausal
Feel
Smooth, mobile, sometimes tender
Imaging
Anechoic on ultrasound (pure fluid)
Move
Aspirate if symptomatic; clear fluid and the mass resolves
Anechoic is the word. Pure fluid lets the ultrasound beam pass straight through. If aspiration gives clear fluid and the lump disappears, it was a simple cyst.
Benign · most common change overall
Fibrocystic change
Patient
Reproductive age
Feel
Bilateral, lumpy, rope-like
Timing
Cyclic tenderness, worst premenstrually
Imaging
Mixed cysts and dense tissue
Both breasts, every month. Bilateral lumpiness that hurts before the period and eases after is fibrocystic change, not a discrete mass.
Benign · the great mimic
Fat necrosis
History
Trauma, surgery, or radiation
Feel
Firm, irregular, can dimple the skin
Imaging
Oil cyst with rim calcification
Biopsy
Lipid-laden macrophages, no cancer
It looks like cancer: firm, irregular, skin dimpling. The trauma history and an oil cyst point to fat necrosis, and biopsy settles it.
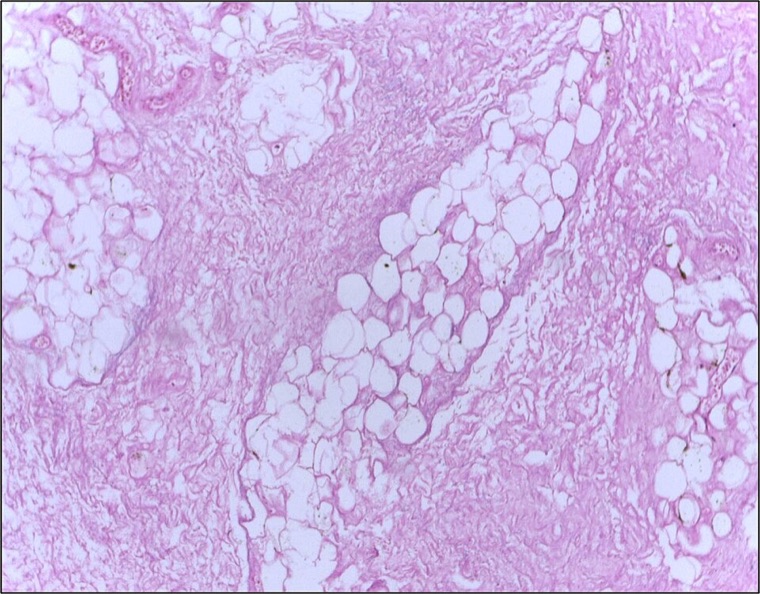
Fat necrosis: foamy lipid-laden macrophages cleaning up damaged fat, with no malignant cells. Benign, but it mimics cancer clinically.
Malignant · the red flags
Carcinoma
Patient
Usually older; risk rises with age
Feel
Fixed, hard, irregular
Skin and nipple
Dimpling, peau d orange, nipple retraction
Imaging
Spiculated mass, pleomorphic microcalcifications
Nodes
Firm, fixed axillary lymph nodes
Fixed, hard, retracting, with nodes. Any of these flips a lump from reassuring to refer. Diagnostic mammogram and ultrasound, then core-needle biopsy.
The Decision Tool · Sort the Finding
Benign or Red Flag?
Tap a finding, then tap the bin it belongs in. Reassuring features go left, red flags go right. Get it right and it locks with the reason.
Reassuring
Benign features. Watch or simple workup.
Red flag
Refer and image. Exclude cancer.
Tap a finding above, then tap a bin.
The Answer Key, Row by Row
Predict each feature, then tap the row to reveal the benign and the malignant version.
Feature
Benign
Malignant
Shape
Round, well bordered
Irregular, spiculated
Mobility
Freely mobile
Fixed to skin or wall
Consistency
Soft to rubbery
Hard
Skin
Normal
Dimpling, peau d orange
Nipple
Normal
Retraction, bloody plus mass
Nodes
None
Firm, fixed axillary nodes
Ultrasound
Wider-than-tall, smooth
Taller-than-wide, irregular
Tap any row to check your prediction
Build the Plan
Work Up a New Breast Mass
One patient, one decision at a time. Guess each branch before it opens. This is the reasoning behind every most-appropriate-next-step question.
From the Attending
Do not let pain steer you. Most breast cancers are painless, and plenty of benign lumps hurt. Sort by the features that predict biology: is it fixed, hard, irregular, retracting the skin or nipple, with nodes? If yes, image and biopsy. If it is a soft mobile mass in a young woman, ultrasound leads. The feel and the imaging decide, not how much it aches.
Don't Miss the Lump
Five Quick Calls
Five rapid questions pulled from a bigger pool, reshuffled every visit. Cross out (right-click or long-press) and highlight (select text) as you read.
Clinical Practice
Walk the Cases
Full clinical vignettes, one at a time, in a shuffled order. Progress saves to your account on this device. Cross out (right-click or long-press) and highlight (select text) as you go.
Your attending drops a chart in front of you on rounds.
Attending
"Pregnant patient, new soft lump in the armpit. Resident already wrote enlarged lymph node. Sign off?"
You
"A lump in the axilla... a node seems reasonable?"
Attending
"It is spongy, it grew with the pregnancy, there is an extra nipple under it, and the ultrasound looks exactly like her breast. That is not a node. That is breast tissue on the milk line."
Attending
"Read every one of these the same way. Match the feel and the story to the structure before you name it."
A new spongy axillary mass that grows in pregnancy, on the milk line with an extra nipple, is accessory breast tissue, not a node. Find the milk line.
Tip: kill the wrong choices first, then read the explanation chain for every option.
Gray's Anatomy. The mammary ridge (milk line), breast structure, and the five groups of axillary lymph nodes with their drainage and relation to the axillary vein.
Moore, Clinically Oriented Anatomy. Axillary contents, lymphatic drainage of the breast, and the apical (infraclavicular) nodes at the venous outlet.
Kumar, Abbas, Aster, Robbins and Cotran Pathologic Basis of Disease. Fibroadenoma, intraductal papilloma, fibrocystic change, fat necrosis, and invasive carcinoma of the breast.
Townsend, Sabiston Textbook of Surgery. Evaluation of a breast mass and nipple discharge, benign versus malignant features, and the role of imaging and core-needle biopsy.
Vignettes are original clinical teaching cases. Demographics, values, and answer order are written for practice. Always confirm management against current guidance at the point of care.
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.