Brachial Plexus and Upper Extremity Nerve Injuries
From roots to terminal branches. Erb's, Klumpke's, the three peripheral nerve palsies, TOS, carpal tunnel, and radial head OMM - one page, every angle.
Opening Challenge
A 24-year-old man is involved in a motorcycle accident. His left arm hangs at the side, adducted and internally rotated, with the forearm pronated. He cannot abduct the shoulder or flex the elbow. Grip strength is intact. On physical exam the biceps reflex is absent on the left but the grasp reflex is preserved.
Which roots are most likely injured?
Correct: A, C5 and C6 (upper trunk - Erb's). The "waiter's tip" posture - arm adducted, internally rotated, forearm pronated - is the hallmark of Erb-Duchenne palsy. The deltoid (abduction), biceps (flexion and supination), and brachioradialis are all innervated by C5-C6. With those roots out, unopposed internal rotators and adductors dominate. Grip is intact because the hand muscles (C8-T1) are unaffected.
Why not C8-T1? C8-T1 injury = Klumpke's = claw hand + intrinsic weakness. Grip would be gone and the fingers would claw. This patient has intact grip - the hand works fine. The problem is all proximal. Rule: waiter's tip posture with absent biceps reflex and intact grip = upper trunk injury, C5-C6.
scroll to learn
Section 1
Brachial Plexus Anatomy
Five roots to five terminal branches. The whole road map in one diagram. Know the layers and you localize every injury instantly.
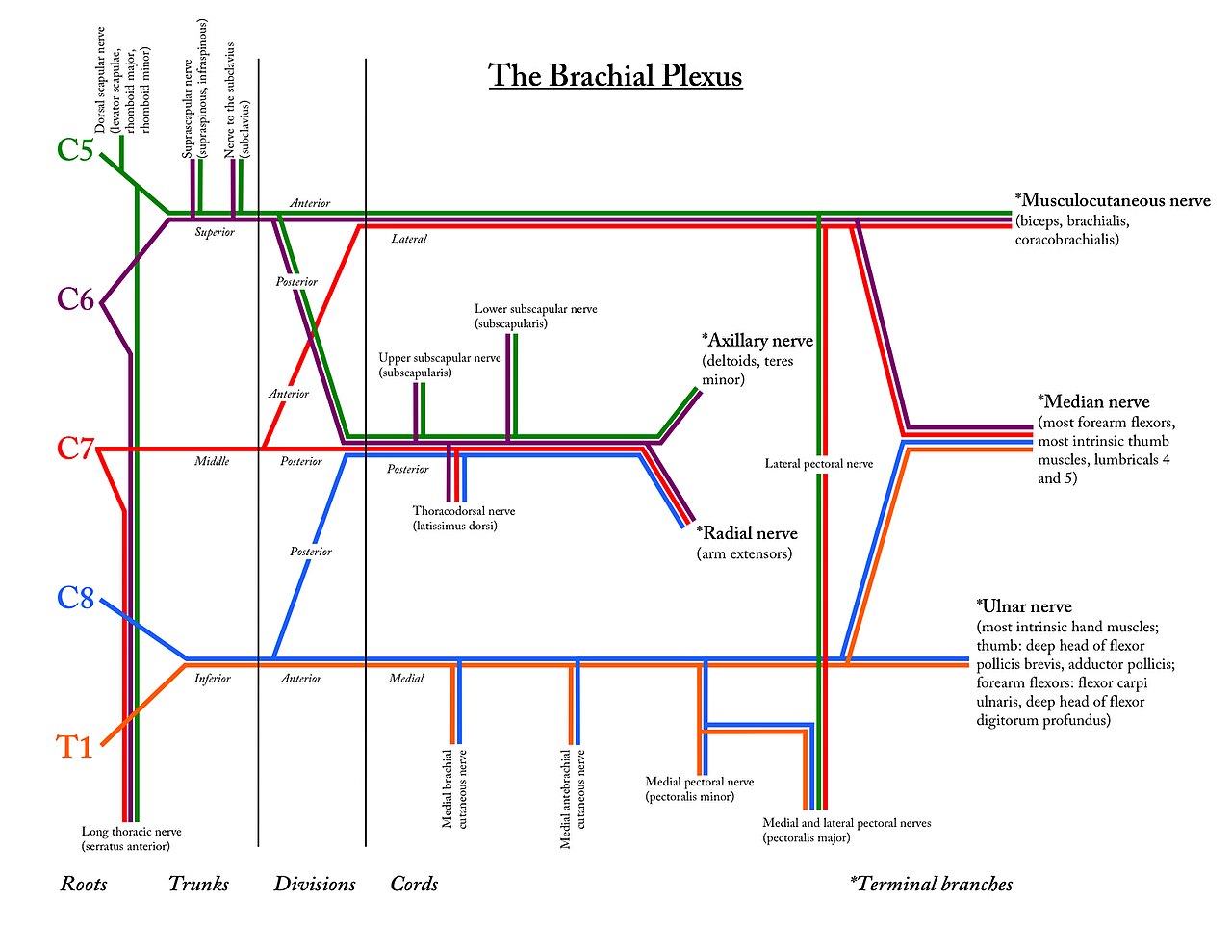
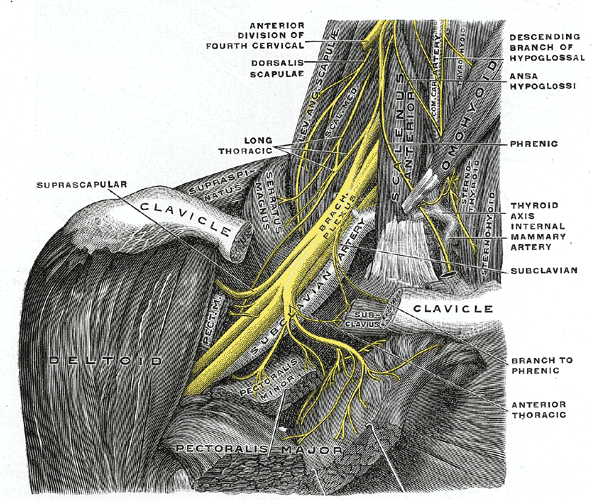
Brachial plexus schematic: roots (C5 to T1), trunks, divisions, cords, and terminal branches. Public domain, via Wikimedia Commons.Ulnar nerve - Gray's Anatomy (plate 808): course and distribution in the forearmBrachial plexus: labeled schematic of the right side showing roots through branches
Cords are named for their position relative to the axillary artery: Lateral, Posterior, Medial. Median nerve = lateral + medial cords. That is why it is called the median nerve - it is the bridge.
High-Yield Fact
Axillary Nerve (C5-C6)
The axillary nerve exits the axilla through the quadrilateral space with the posterior humeral circumflex artery. An anterior shoulder dislocation or surgical neck of humerus fracture puts it at risk.
Loss: deltoid paralysis (cannot abduct past 15 degrees) + lateral shoulder numbness over the "regimental badge" area. Test with resisted abduction at 90 degrees.
From the Attending
Brachial plexus questions always tell you where the lesion is through the combination of muscles lost and the level of reflex loss. The biceps reflex (C5-C6) down with arm posture = upper trunk. Intrinsic hand loss with a claw = lower trunk. All of this is pattern recognition once you know the root-to-muscle assignments. Know your clues. Every time.
Section 2
Erb's vs Klumpke's
Two directions of traction, two completely opposite presentations. Get the mechanism right and the posture follows logically every time.
C5 and C6 - Upper Trunk
Erb-Duchenne Palsy
Mechanism: lateral traction of head away from shoulder (birth - shoulder dystocia; adult - motorcycle fall) stretches the C5-C6 roots away from the spine.
Losses: deltoid (abduction), biceps/brachialis (flexion), brachioradialis, supraspinatus and infraspinatus (ER)
The muscles that abduct and externally rotate are gone (deltoid, supraspinatus, infraspinatus). The opposing muscles - pectoralis major (adduction) and subscapularis (internal rotation) - work unopposed. Gravity wins at the elbow because biceps is out. Pronation defaults because supinator (C6) is also damaged.
Board rule: the posture tells you WHICH muscles are absent. Adducted + IR + pronated means the C5-C6 muscle group is down.
C8 and T1 - Lower Trunk
Klumpke's Palsy
Mechanism: hyperabduction of the arm (grabbing overhead during a fall, or breech delivery with arm raised above head) stretches C8-T1 roots.
Losses: ALL intrinsic hand muscles (all lumbricals, all interossei, thenar, hypothenar) via both median and ulnar C8-T1 contributions
Posture:all four fingers clawed (MCP hyperextension + IP flexion), wrist flexed
Bonus: if T1 is avulsed hard enough, the cervical sympathetic chain is dragged - producing Horner syndrome: ptosis, miosis, anhidrosis, all ipsilateral
Distinction
Erb's vs Klumpke's
Erb's: proximal arm lost, hand intact. Patient has grip. Klumpke's: distal hand lost, proximal arm intact. Patient can move shoulder and elbow but the hand is useless.
Key discriminator in clinical practice: the question will specify whether grip/intrinsics are preserved or absent. If grip is intact - upper trunk. If grip is gone and there is a claw - lower trunk.
Horner syndrome in the context of brachial plexus injury = always Klumpke's (T1 avulsion dragged the sympathetic chain).
TOS - Three Zones
Thoracic Outlet Syndrome
The brachial plexus + subclavian vessels must pass through three anatomically narrow spaces between neck and axilla. Compression at any zone = TOS:
1. Scalene triangle - between anterior and middle scalenes. Adson test: deep breath + head turned toward affected side compresses.
2. Costoclavicular space - between first rib and clavicle. Military brace test: shoulders pulled back and down.
3. Pec minor tunnel - under pec minor + coracoid. Wright's / hyperabduction test.
Neurogenic vs Vascular
TOS Types
Neurogenic TOS (95%): C8-T1 most affected (lower plexus runs closest to first rib). Hand intrinsic weakness, medial forearm and hand numbness (ulnar distribution).
Vascular TOS: arm pallor, pulselessness, color change with position. Subclavian artery or vein involved.
clinical medicine trap: TOS mimics ulnar nerve injury (both affect medial hand/ring-pinky). TOS is positional (provoked by arm elevation); ulnar nerve injury is not. Positive Adson or Wright test = TOS.
Section 3
The Three Peripheral Nerve Palsies
Ulnar, median, and radial. Each has a signature posture, a signature mechanism, and a board trap built in. Select a nerve to see the injury animate.
Ulnar Nerve Injury
Site: Medial epicondyle groove or Guyon's canal (wrist)
Motor loss: Lumbricals 3 and 4 (ring/pinky), all interossei, hypothenar, adductor pollicis
Sensory loss: Medial hand + ring (medial half) + pinky
Sign: Froment's sign - patient flexes thumb IP joint (using FPL via median) when trying to pinch paper because adductor pollicis (ulnar) is out
Board rule: Ulnar paradox - wrist-level injury produces a WORSE claw than elbow-level because FDP to ring and pinky is still intact at the wrist, driving strong IP flexion.
A patient with a humeral midshaft fracture presents with wrist drop. Which nerve is most likely injured, and at which anatomical level?
Nerve
Common injury site
Motor loss
Sensory loss
Posture
Ulnar (C8-T1)
Medial epicondyle groove; Guyon's canal
Lumbricals 3-4, all interossei, hypothenar, adductor pollicis
Posterior dislocation: caused by seizures or electrocution - the massive simultaneous muscle contraction posteriorly levers the humeral head backward. X-ray shows "lightbulb sign" because the internally rotated humerus looks like a light bulb on AP view. Often missed on first read. Any "seizure + arm held adducted and internally rotated" = posterior dislocation until proven otherwise.
Carpal Tunnel
Median Nerve Compression
Nine tendons + one nerve pass under the flexor retinaculum. Any volume increase inside the tunnel compresses the median nerve.
Classic: nocturnal paresthesias in lateral 3.5 fingers, relieved by shaking the hand (flick sign)
Dermatomes C5-T1 quick rule: lateral to medial = C5 to T1. C5 = lateral arm (deltoid patch). C6 = thumb and index. C7 = middle finger. C8 = ring and pinky. T1 = medial arm. The dermatome pattern is the same as the root innervation pattern - knowing the dermis tells you the root.
Section 5 · Board Walkthrough
Board Walkthrough
7 original 3rd-order vignettes. One at a time. Shuffle on. Cross out wrong answers with a long-press. Highlight your reasoning with a double-tap.
VIGNETTE 1 OF 7
A 3-day-old male infant is brought to the clinic after a prolonged vaginal delivery complicated by shoulder dystocia. On physical exam the right arm hangs adducted and internally rotated, with the forearm pronated. The biceps reflex is absent on the right but the grasp reflex is intact and symmetric. X-ray of the right humerus and clavicle shows no fracture. The Moro reflex is absent on the right. The infant tracks visually and the left extremities appear normal.
Which nerve roots are most likely injured?
Correct: A, C5 and C6. The "waiter's tip" posture - arm adducted, internally rotated, forearm pronated, with absent biceps reflex and intact grip - is the textbook presentation of Erb-Duchenne palsy. The mechanism here is shoulder dystocia: the infant's head is pulled laterally away from the right shoulder, stretching C5 and C6 roots of the upper trunk. Deltoid (abduction), biceps (flexion and supination), brachioradialis, and supraspinatus are all C5-C6 innervated. With those muscles absent, gravity and the intact pectoralis and subscapularis dominate, producing adduction and internal rotation. Grip is intact because the intrinsic hand muscles run through C8-T1 - untouched here.
Why not C7 (choice B)? C7 middle trunk injury targets the triceps (elbow extension weakness) and wrist extensors, causing a picture closer to wrist drop with preserved shoulder and elbow flexion. There is no characteristic "waiter's tip" posture from isolated C7 injury. C7 injury means triceps weakness and wrist extension problems, not the proximal arm posture seen here.
Why not C8-T1 (choice C)? C8-T1 (Klumpke's) destroys all intrinsic hand muscles. This infant would have absent grip and finger clawing. The shoulder and elbow would move normally. This patient has preserved grip - that rules out lower trunk injury. Intact grip with proximal arm palsy = upper trunk, not lower.
Why not pan-plexus (choice D)? Pan-plexus injury would eliminate BOTH proximal and distal function - no shoulder, no elbow, no hand. This infant has intact grip and symmetric hand reflexes, so the lower trunk is functioning. Selective proximal arm deficit with intact hand = upper trunk C5-C6, not the full plexus.
The arm assumes adduction because pectoralis major (adductor, intact) and latissimus dorsi win over the dead deltoid and supraspinatus. Internal rotation persists because subscapularis (IR, intact) faces no opposition from infraspinatus and teres minor (ER, dead). Pronation defaults because the supinator (C6, out) can no longer oppose gravity and the intact pronator teres. The whole posture is just physics: show me which muscles died and I will show you the position.
The biceps reflex (C5-C6) is absent here because both roots innervating that arc are damaged. The grasp reflex is intact because it runs through C8-T1 - untouched. in clinical practice, whenever a reflex is absent you can read the root level directly. Absent biceps = C5 or C6 problem. Absent triceps = C7 problem. That is the shortcut. Every absent reflex is a direct window into a root level. Use it.
VIGNETTE 2 OF 7
A 22-year-old man is brought to the emergency department after falling asleep with his arm draped over the back of a chair for several hours at a party. He awakens unable to extend his right wrist. On physical exam the wrist droops against gravity and he cannot actively extend the fingers. Sensation is diminished over the dorsum of the first web space between the thumb and index finger. Elbow extension is fully preserved. Brachioradialis reflex is absent. X-ray of the right humerus shows no fracture.
Which structure is most likely injured?
Correct: B, radial nerve at the spiral groove. "Saturday night palsy" - compression of the radial nerve in the spiral groove of the humerus while sleeping with the arm draped over a hard surface. The spiral groove level explains EVERYTHING here: wrist drop (wrist extensors gone), finger extension loss (EDC gone), absent brachioradialis reflex (C6, radial innervated), and sensory loss over the dorsal first web space. Elbow extension is PRESERVED because the branch to triceps arises proximal to the spiral groove - this localizes the injury beautifully to the midshaft level.
Why not axillary nerve (choice A)? The axillary nerve at the quadrilateral space causes deltoid weakness (shoulder abduction loss) and lateral shoulder numbness. It does NOT cause wrist drop or finger extension loss - it has no forearm or hand targets at all. Axillary nerve injury means flattened deltoid and badge area numbness - no wrist involvement ever.
Why not PIN (choice C)? The posterior interosseous nerve branches from the radial nerve distal to the elbow. A pure PIN injury causes finger and thumb extension loss but SPARES wrist extension (ECRL is innervated before the PIN branches off) and has NO sensory component (PIN is purely motor). This patient has wrist drop AND sensory loss - that pattern requires a more proximal radial nerve lesion. PIN injury = no sensory loss + wrist can extend (ECRL preserved). Spiral groove = wrist drops + sensory loss.
Why not ulnar nerve (choice D)? Ulnar nerve injury at the medial epicondyle produces ring and pinky clawing, medial hand sensory loss, and Froment's sign. It does NOT cause wrist drop - the wrist extensors are radial nerve territory. This patient's presentation is entirely in the radial distribution. Ulnar injury = claw of ring and pinky, not wrist drop.
At the spiral groove, the triceps branches are already off - so triceps works. Brachioradialis branch is at or just distal to the groove - that reflex drops. Wrist extensors and finger extensors are hit. So the rule is: if triceps works but brachioradialis is out and wrist drops, you are at the spiral groove. If everything from triceps down is out, you are at the axilla. If only finger extension drops (wrist extends fine) and there is no sensory loss, you are at the PIN level. Know your levels. The motor and reflex losses tell you exactly where on the nerve you are standing.
VIGNETTE 3 OF 7
A 34-year-old construction worker presents with right hand weakness after striking the medial aspect of the right elbow against steel scaffolding one week ago. On physical exam he is unable to abduct the little finger or cross his fingers. EMG shows denervation of the flexor digitorum profundus to the ring and little fingers. The ring and pinky show clawing with MCP hyperextension and IP flexion. A second patient in the same clinic sustained an injury to the same nerve at the wrist level and presents with an equivalent claw deformity.
Compared to the wrist-level injury, this patient's ring and pinky claw is most likely which of the following?
Correct: B - less severe claw because FDP to ring and pinky is also lost. This is the ulnar paradox. At the elbow, the ulnar nerve innervates FDP to the ring and little finger BEFORE branching into the hand intrinsics. So an elbow-level injury knocks out BOTH the intrinsics (causing MCP hyperextension via EDC unopposed) AND the FDP to ring/pinky (reducing IP flexion). The result is partial MCP hyperextension but minimal IP flexion - a less dramatic claw. At the wrist, FDP branches are already given off and intact, so IP flexion is strong - creating a more pronounced claw. The paradox: higher (elbow) injury = less claw; lower (wrist) injury = worse claw.
Why not choice A (more severe)? This is the intuitive but wrong answer. Bigger injury does not mean more dramatic claw. The claw requires active IP flexion to look dramatic - you need working FDP for that. When FDP is also out, IP flexion collapses, and the claw is milder. The severity of the claw depends on FDP status, not injury level per se.
Why not choice C (identical)? The intrinsic deficit IS the same at both levels in terms of which intrinsics are absent. The difference is that FDP adds to IP flexion. Without FDP (elbow injury), IP flexion weakens, reducing claw severity. Identical intrinsic loss does not mean identical clinical picture when FDP status differs. Same intrinsic loss, different FDP status, different claw severity - this is the paradox.
Why not median compensation (choice D)? The median nerve innervates lumbricals 1 and 2 (index and middle), not 3 and 4. There is no median compensation for ring and pinky lumbricals. Compensation across nerve territories for a specific muscle does not happen in peripheral nerve anatomy. Median nerve does not compensate for ulnar ring and pinky lumbricals - the lumbrical 3-4 territory is strictly ulnar.
The claw posture requires two things: MCP hyperextension (from intact EDC with no lumbrical opposition) and IP flexion (from intact FDP). Lumbricals normally oppose EDC at the MCP and transmit force to IP joints for extension. Kill the lumbrical: EDC hyperextends the MCP. If FDP is intact (wrist injury), it can flex the IP joint strongly - full dramatic claw. If FDP is also dead (elbow injury), IP flexion is gone - the finger just collapses limply. Claw formula: EDC unopposed at MCP + FDP driving IP flexion = dramatic claw. Remove FDP and the claw becomes less pronounced.
VIGNETTE 4 OF 7
A 38-year-old woman at 28 weeks gestation presents with a 3-week history of right hand numbness that is worst at night and wakes her from sleep. She reports that shaking the hand provides temporary relief. On physical exam, sensation is reduced over the palmar surface of the thumb, index finger, middle finger, and radial half of the ring finger. Thenar muscle bulk is symmetric. Nerve conduction studies show prolonged median nerve distal motor latency at the right wrist (5.8 ms; normal less than 4.5 ms). A bedside provocative test reproduces the tingling after 45 seconds of maintained wrist flexion.
Which physical examination test was most likely performed to reproduce her symptoms?
Correct: B, Phalen's test. The clue is "maintained wrist flexion reproduces numbness after 45 seconds." That is the exact mechanism of Phalen's test: sustained wrist flexion increases carpal tunnel pressure, compressing the median nerve and reproducing paresthesias in its distribution (lateral 3.5 fingers). Phalen's is the most sensitive clinical test for CTS. The presentation - pregnancy, nocturnal paresthesias, shaking relief (flick sign), lateral 3.5 finger distribution, and prolonged NCS latency - is a textbook carpal tunnel syndrome case. Pregnancy causes increased interstitial fluid volume that raises tunnel pressure.
Why not Tinel's (choice A)? Tinel's sign involves tapping OVER the tunnel (not sustained flexion) and produces an electric shock-like tingling if median nerve is compressed. It requires percussion, not wrist flexion. The stem says "45 seconds of maintained wrist flexion" - that is Phalen's by definition. Tinel's is less sensitive than Phalen's. Percussion over tunnel = Tinel's. Sustained wrist flexion = Phalen's. Know the distinction.
Why not Finkelstein's (choice C)? Finkelstein's tests the first extensor compartment (APL and EPB tendons) for DeQuervain's tenosynovitis. It produces radial wrist pain at the radial styloid, not finger paresthesias. This patient has finger numbness - not radial wrist pain - and the affected region is the median distribution, not the first extensor compartment. Finkelstein's = radial wrist pain at the styloid = DeQuervain's, not carpal tunnel.
Why not Froment's sign (choice D)? Froment's tests adductor pollicis weakness (ulnar nerve). The patient would flex the thumb IP joint using FPL (median innervated) when trying to hold paper. This patient has intact thenar bulk and no mention of ulnar territory symptoms. Her sensory loss is lateral (median) not medial (ulnar). Froment's = ulnar nerve deficit at the adductor pollicis, not carpal tunnel syndrome.
Pregnancy causes systemic fluid retention via increased aldosterone and estrogen effects on fluid distribution. The carpal tunnel is a closed rigid compartment - bones on three sides, flexor retinaculum on the fourth. Any increase in interstitial fluid raises tunnel pressure directly onto the median nerve. It is the same mechanism as hypothyroidism (myxedema), acromegaly (bony and soft tissue hypertrophy), and rheumatoid arthritis (synovial proliferation) - all increase tunnel contents, all compress the nerve. CTS risk factors = anything that adds volume inside a fixed rigid compartment.
VIGNETTE 5 OF 7
A newborn female infant was delivered by breech presentation. During delivery the right arm was hyperabducted to complete the delivery of the aftercoming head. On physical exam at 2 hours of life, the right hand is held in a claw posture with MCP hyperextension and IP flexion of all four fingers. The grasp reflex is absent on the right. Right-sided ptosis, miosis, and anhidrosis are noted on examination. Moro reflex is intact on the left. X-ray of the right clavicle and shoulder shows no fracture.
Which nerve roots are most likely responsible for both the hand posture and the facial findings?
Correct: C, C8 and T1 lower trunk with T1 sympathetic chain involvement. This is Klumpke's palsy with Horner syndrome - a classic pairing. The mechanism of hyperabduction during breech delivery specifically stretches the lower trunk (C8-T1), destroying all intrinsic hand muscles and creating the all-finger claw. The bonus finding is Horner syndrome (ptosis, miosis, anhidrosis), which occurs because T1 sits adjacent to the cervical sympathetic chain. A forceful enough avulsion of T1 drags the sympathetic fibers with it, interrupting the ipsilateral oculosympathetic pathway. Klumpke's plus Horner = lower trunk plus T1 sympathetic chain - they travel together.
Why not C5-C6 (choice A)? Erb's palsy produces waiter's tip - the proximal arm deformity. The hand in Erb's is completely normal because C8-T1 (hand intrinsics) are untouched. This infant has all-finger clawing and absent grasp - that means the hand intrinsics are gone, which is strictly C8-T1. An infant with intact hand function but limp proximal arm = Erb's. Absent hand function with clawing = Klumpke's. The hand function status is the discriminating clue here.
Why not pan-plexus (choice B)? Pan-plexus would eliminate both proximal and distal arm function - no shoulder, no elbow, no hand. The Moro reflex being intact on the left and the fact that only the right arm is affected is consistent with a unilateral lower trunk injury, not a total plexus avulsion. The shoulder moves (deltoid and supraspinatus intact) - evidence that C5-C6 is working. Preserved proximal arm motion rules out pan-plexus avulsion.
Why not C7-C8 (choice D)? C7 middle trunk injury adds triceps weakness and wrist drop. The stem does not mention either finding. The isolated combination of all-finger intrinsic loss plus Horner syndrome points cleanly to lower trunk C8-T1, not a middle-lower combination. C7 involvement would produce triceps and wrist extensor weakness - absent here, so C7 is not involved.
The preganglionic sympathetic fibers for the eye originate in the hypothalamus, descend through the spinal cord, exit at C8-T1-T2 (the ciliospinal center of Budge), travel along the T1 root, ascend through the stellate ganglion, follow the internal carotid artery to the eye. The T1 root is the gateway for this pathway. Avulse T1 hard enough (as in a traumatic Klumpke's from hyperabduction) and you sever the preganglionic sympathetic fiber, interrupting the entire arc. The eye loses sympathetic tone: eyelid droop (ptosis, from superior tarsal muscle), small pupil (miosis, from unopposed sphincter), and dry skin (anhidrosis, from absent sweat gland drive). T1 avulsion = Horner syndrome because T1 carries the preganglionic oculosympathetic fibers out of the cord.
VIGNETTE 6 OF 7
A 46-year-old male cyclist presents with a 2-week history of right forearm ache and progressive right hand weakness following an unusually long ride. On physical exam, he is unable to extend the index finger at the MCP joint; ring and pinky extension is also weak, but wrist extension is preserved and the wrist actively extends to neutral against resistance. Sensation is completely normal over the entire hand and dorsal forearm. MRI of the right forearm shows edema in the soft tissues adjacent to the proximal radius with no fracture.
Which nerve is most likely injured?
Correct: B, posterior interosseous nerve (PIN). The PIN is the motor branch of the radial nerve that arises at the elbow and enters the radial tunnel. It innervates finger extensors (EDC, EDQ, EIP) and thumb extensors, but NOT the wrist extensors (ECRL takes off before PIN branches). The classic PIN pattern is: finger extension loss + thumb extension loss with INTACT wrist extension and NO sensory loss. Cyclists are at risk because repeated forearm pronation and supination during long rides can entrap the PIN at the arcade of Frohse (fibrous arch near the proximal radius). The MRI showing edema near the proximal radius confirms the location. Finger extension loss + intact wrist extension + no sensory loss = PIN injury.
Why not radial nerve at spiral groove (choice A)? Spiral groove injury causes wrist drop (wrist extension lost) AND sensory loss over the dorsal first web space. This patient has preserved wrist extension and no sensory loss - two findings that immediately exclude a spiral groove lesion. The spiral groove hits the nerve before ECRL branches, so wrist extension falls. PIN is after ECRL branches, so wrist extension is spared. Preserved wrist extension + no sensory loss = distal to the ECRL branch point = PIN, not spiral groove.
Why not anterior interosseous nerve (choice C)? AIN is a motor branch of the MEDIAN nerve. It innervates FPL and FDP to the index finger, enabling the distal "OK" sign (pinch). AIN injury produces loss of terminal flexion of the thumb IP and index DIP - the patient cannot form a precise circle with the OK gesture. This patient has EXTENSION problems, not flexion problems. AIN and PIN are both pure motor branches but they are on opposite sides of the limb. AIN = median motor branch, flexion problem, no sensory loss. PIN = radial motor branch, extension problem, no sensory loss.
Why not Guyon's canal ulnar (choice D)? Guyon's canal (wrist-level ulnar nerve) can present as a purely motor lesion if the lesion is distal to the sensory branch takeoff. However, ulnar motor territory at the wrist covers intrinsic hand muscles (lumbricals 3-4, interossei, hypothenar, adductor pollicis) - not finger extensors. Extension is entirely in the radial nerve territory. Ulnar nerve injury never causes wrist drop or finger extension loss - those are radial territory exclusively.
ECRL (extensor carpi radialis longus) takes off from the radial nerve just before the PIN branches in the radial tunnel. This is the anatomical dividing line: injury above ECRL takeoff = wrist drops. Injury below ECRL takeoff = wrist extends, but fingers cannot. in clinical practice, this becomes a one-clue diagnosis: preserved wrist extension with lost finger extension means the injury is distal to the ECRL branch point, which is the PIN level. Use ECRL status as your localizer every time. ECRL intact (wrist extends) means the lesion is at or below the radial tunnel - that is PIN territory.
VIGNETTE 7 OF 7
A 31-year-old physical therapist presents with right elbow stiffness following a fall onto an outstretched hand (FOOSH) three days ago. On osteopathic structural examination, the radial head is palpated lateral to the biceps tendon insertion and is found to be in an anteriorly displaced position. Range of motion reveals that pronation is limited at 60 degrees (normal 80-90 degrees) while supination is full and painless. X-ray of the elbow shows no fracture or dislocation of the radial head.
Which osteopathic treatment most directly addresses this radial head dysfunction?
Correct: B - posterior force on the radial head while pronating the forearm. This is an anterior radial head dysfunction. The radial head is stuck in the anterior (supinated) position. The motion restriction is pronation - the head cannot move posteriorly. Treatment follows a simple rule: the head is displaced anteriorly, so push it posteriorly. And the forearm should be taken INTO the restricted direction (pronation) simultaneously, using the kinetics of the radioulnar joint to seat the head in its corrected position. Push posterior + guide into pronation = corrects the anterior displacement. Anterior radial head: push posterior + pronate. Posterior radial head: push anterior + supinate. Named position is treated by reversal.
Why not choice A (anterior force + supination)? This describes the treatment for a POSTERIOR radial head dysfunction - the opposite of what is present here. A posterior radial head is stuck in pronation, needs anterior push and supination to restore. Applying this treatment to an anterior head would push the already anteriorly displaced head even further forward. Match the treatment direction to the dysfunction: anterior head needs posterior correction, not more anterior force.
Why not choice C (lateral force)? Radial head dysfunction at the proximal radioulnar joint involves anterior-posterior displacement related to pronation-supination mechanics, not lateral displacement. Lateral force does not address the relevant joint axis and would not restore the head to its correct position within the annular ligament. Radial head OMM uses anterior-posterior corrective vectors, not lateral ones.
Why not choice D (long-axis traction)? Long-axis traction may be useful as a general elbow mobilization technique but does not specifically address the anterior positional displacement of the radial head. The dysfunction here is positional - the head is anteriorly displaced - not a distraction or compression problem. Traction does not correct a positional fault at the radioulnar joint. Positional faults need positional corrections: posterior vector to correct the anteriorly displaced head.
The radial head moves anteriorly during supination (the head rotates forward as the radius rotates to face palm up) and posteriorly during pronation (rotates backward as the forearm turns palm down). When stuck anteriorly, the restriction is that it cannot go posterior during pronation - so pronation is limited. When stuck posteriorly, supination is limited. The rule is simple: named position = where it is stuck = the motion that is free. What is restricted is the opposite. Treatment: take the restriction to its barrier. Anterior head cannot pronate, so treatment takes it to pronation while correcting the positional fault by pushing posterior. OMM rule: the dysfunction is named for where the structure is, treatment moves it away from that position into the restricted direction.
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.