Why "dextro" means left and your brain hates it. Naming, classification, rib humps, and how to never miss the structural vs functional question again.
🤯
Here's the thing that trips everyone up: In scoliosis, dextroscoliosis means the vertebrae are sidebent to the LEFT. Not right. Left. The name describes the convexity → the bump-out side → not the direction the spine actually bends.
Once you see WHY it's named that way, you'll never mix it up again. Let's build the mental model.
THE RULE
Scoliosis = Named by Convexity
One rule governs ALL scoliosis naming. Everything else follows from this.
🎯
Scoliosis is ALWAYS named by the direction of the CONVEXITY → the side the curve bows OUT toward. Not the direction the vertebrae sidebend. The convexity is on the OPPOSITE side of the sidebend.
🔑Dextro = convexity points to your DominanD hanD (right). The vertebrae bend the OTHER way.
The link
Why the Name Feels Backwards
Follow the dominoes. Each step makes the next one inevitable.
Vertebrae sidebend LEFT→Concavity forms on LEFT→Convexity bows out RIGHT→Named by convexity = DEXTRO
Think of it like a bow (the weapon). You pull the string LEFT → that's the sidebend. The bow itself curves out to the RIGHT → that's the convexity. We name the bow by where it's pointing, not where you're pulling.
Vertebrae sidebend RIGHT→Concavity forms on RIGHT→Convexity bows out LEFT→Named by convexity = LEVO
SEE IT
Interactive Spine
Watch the curve form. See where the convexity lands.
Normal spine → no lateral curvature
WHY IT MATTERS
The Rib Hump Connection
This is where it gets real on exam day.
When vertebrae sidebend in a structural curve, the vertebral bodies rotate toward the convexity. The ribs are bolted to those vertebral bodies. So the ribs on the convex side get shoved backwards → creating a posterior rib hump you can see on the Adam's forward bend testPatient bends forward at the waist with arms hanging and knees straight. Examiner looks from behind for asymmetry. A rib hump = structural scoliosis. No hump = functional..
Structural curve→Vertebral bodies rotate toward convexity→Ribs follow the body→Rib hump on CONVEX side
💡
Rib hump on the RIGHT = convexity on the RIGHT = dextroscoliosis. The hump TELLS you the name. It's literally pointing at the answer.
THE SPLIT
Structural vs Functional
One is real. One is a posture problem. The test is dead simple.
Structural
The real deal
Functional
The impostor
Structural scoliosis = the vertebrae are physically wedged, rotated, and stuck. The curve is built into the bone.
Think of it like a tree that grew crooked. You can't straighten it by pushing → the wood itself is bent.
Functional scoliosis = the spine LOOKS curved, but the bones are fine. Something else is pulling it off-center.
Feature
Finding
Sidebend correction
CORRECTS with opposite sidebending
Adam's test
No rib hump (no vertebral rotation)
Vertebral rotation
None → spine is structurally normal
Cause
Leg length discrepancy, muscle spasm, pain-guarding, herniated disc
X-ray
No vertebral wedging, curve disappears on lateral bending films
Think of it like leaning to one side because one shoe has a thicker sole. Take the shoe off → you're straight again. Fix the cause and the curve goes away.
🚨Board Trap: "Does not improve with sidebending" When the stem says the curvature "does not improve with sidebending to the opposite side" → that's the writers telling you it's structural. If it corrected, it would be functional. They hand you this clue in almost every scoliosis question. Grab it.
🔑Structural = Stuck. Functional = Flexible.
THE CONNECTION
Fryette's Laws & Scoliosis
Same rules you already know → just applied to curves.
When a question gives you segmental findings like "L1-L5 neutral, sidebent right, rotated left" → that's Fryette's Type IType I (group curves): vertebrae are in neutral (not flexed/extended), sidebending and rotation go in OPPOSITE directions. This is the behavior of grouped vertebrae → like a whole spinal region curving together. behavior. Neutral spine, sidebending and rotation go opposite directions.
Fryette's Law
Position
Sidebend & Rotation
Clinical Example
Type I (group)
Neutral
Opposite directions
L1-L5 neutral, SB right, rot left → group lumbar curve
Type II (single)
Flexed or Extended
Same direction
T6 flexed, SB left, rot left → single segment dysfunction
🧩
In scoliosis, group curves follow Type I mechanics. The sidebend tells you the concavity side. Flip it for the convexity. That gives you the name. Example: sidebent RIGHT → concavity RIGHT → convexity LEFT → levoscoliosis.
TEST YOURSELF
Name That Curve
Three quick scenarios. Can you name the scoliosis from the findings?
A patient has a posterior rib hump on the LEFT at T5-T10 on forward bending. The curve does not correct with right sidebending. What is this?
Structural dextroscoliosis
Structural levoscoliosis
Functional levoscoliosis
Functional dextroscoliosis
L1-L5: neutral, sidebent left, rotated right. Curve corrects when patient sidebends right. What type of lumbar scoliosis is this?
Structural levoscoliosis
Functional dextroscoliosis
Structural dextroscoliosis
Functional levoscoliosis
T3-T12 shows right-sided convexity on X-ray with a Cobb angle of 35 degrees. L1-L5 shows left-sided convexity. How do you name this?
Thoracic levo + lumbar dextro
Thoracic levo + lumbar levo
Thoracic dextro + lumbar levo
Thoracic dextro + lumbar dextro
THE VILLAINS
Scoliosis Types: Flip to Compare
Three villains. Same curve, different causes and rules. Tap each card.
🧬
Idiopathic
Most common type (80%)
tap to learn
Adolescent Idiopathic Scoliosis (AIS)
Peak onset: 10-18 years, especially girls. Right thoracic curve is classic. Cobb angle determines treatment.
Cobb thresholds: <25° = observe. 25-40° = brace (TLSO). >40-45° = surgical fusion. Greater than 50° in adults = progressive.
Vertebral formation failure (hemivertebrae) or segmentation failure (bar). Present at birth, often found in infancy.
Key: associated with VACTERL anomalies (cardiac, renal, tracheoesophageal). Always get cardiac echo and renal ultrasound.
Board trap: congenital does not correct with sidebending and progresses rapidly during growth spurts.
🧠
Neuromuscular
Muscle / nerve driven
tap to learn
Neuromuscular Scoliosis
Caused by cerebral palsy, Duchenne MD, spina bifida, Friedreich ataxia. Muscle imbalance drives the curve.
Tends to be a long C-shaped curve (vs S-curve in idiopathic). Progresses even after skeletal maturity. Often requires surgery at lower Cobb angles than idiopathic.
Always structural. There is no functional neuromuscular scoliosis.
THE REVEAL
Same Pattern, Different Clothes
You've already seen this naming logic somewhere else.
You know how in EKGs, we name the axis deviationThe QRS axis tells you which direction the heart's electrical vector is pointing. Left axis deviation means the vector points leftward → but it's the RIGHT-sided leads (like Lead III) that show the negative deflection. The abnormal side is OPPOSITE to the name. by where the vector POINTS, not by which side is doing the pulling? Left axis deviation = the vector points LEFT, but the problem might be in the LEFT anterior fascicle pulling it there.
Scoliosis naming works the same way. We name the OUTPUT direction (where the curve points / where the vector points), not the INPUT direction (which way the vertebrae bend / which fascicle pulls). Once you see this pattern → "name by where it's going, not what's causing it" → it clicks across both topics.
THE ALGORITHM
Exam Day: 4 Steps
When you see a scoliosis question, run this.
Step 1: Does the curve correct with opposite sidebending?
Yes → Functional | No → Structural
Step 2: Where is the convexity? (Look for rib hump side, or stated convexity, or flip the sidebend direction)
Convexity RIGHT → Dextro | Convexity LEFT → Levo
Step 3: Which region? (Thoracic, lumbar, or both?)
Name each region separately: "thoracic dextroscoliosis with lumbar levoscoliosis"
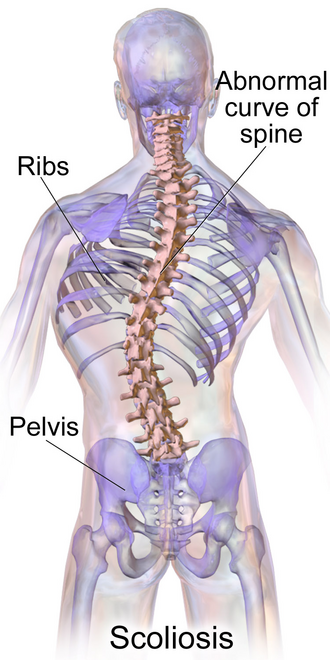
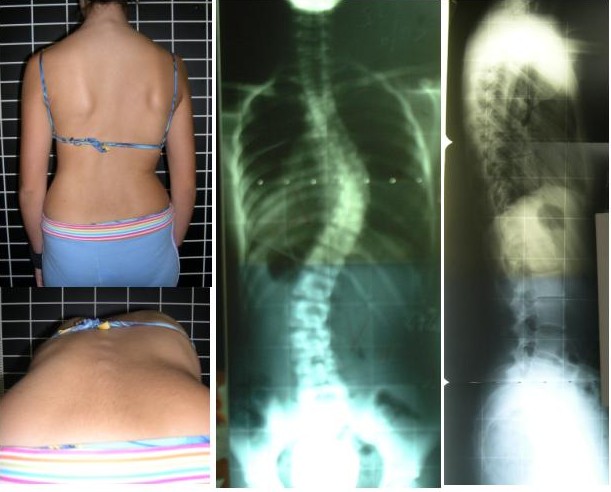
What the examiners see. Lock in the visual. Scroll right for all images.
Scoliosis (medical illustration)
Adam's forward bend test (left) with scoliosis X-rays
TLSO brace (Cobb 25-40 degrees)
Cobb angle measurement technique
Hemivertebra: congenital scoliosis cause
×
DECISION TREE
Cobb Angle → Treatment
One number drives every management decision. Click each node for the reasoning.
Patient has lateral spinal curvature on X-ray. Measure Cobb angle.
The Cobb angle is measured between the most tilted vertebra above and below the curve apex. Draw a line along the superior endplate of the top vertebra and the inferior endplate of the bottom vertebra. The angle between these lines (or their perpendiculars) = Cobb angle. Every treatment decision in scoliosis flows from this single number.
Cobb <25 degrees
Observe only. X-ray every 6-12 months. No brace needed.
Below 25 degrees, curves are unlikely to progress significantly. Monitor with imaging during growth. If the curve increases by 5-10 degrees on two consecutive X-rays, upgrade to bracing. Curves under 25 degrees usually do not require treatment in skeletally mature patients.
Cobb 25-40 degrees
Skeletally immature? Is patient still growing?
The key question is skeletal maturity. The Risser sign (iliac apophysis ossification) grades 0-5: Risser 0-2 = still growing = brace. Risser 4-5 = done growing = curve unlikely to progress. Age alone is less reliable than the Risser sign for assessing maturity.
MATURE (Risser 4-5)
Observe. Curve stable. No brace.
In skeletally mature patients, curves 25-40 degrees are unlikely to progress significantly. Annual monitoring is sufficient. Brace is ineffective after growth is complete because the whole point of bracing is to guide growth.
IMMATURE (Risser 0-2)
Brace (TLSO). Wear 16-23 hrs/day.
Bracing works by applying corrective forces during growth. The TLSO (thoracolumbar sacral orthosis) is the standard. Compliance is everything: 16+ hours/day prevents progression in 72% of patients vs 48% in low-compliance. The goal is NOT to correct the curve but to STOP it from getting worse. If Cobb reaches 40+, reassess for surgery.
Cobb >40-45 degrees → Surgical spinal fusion
Above 40-45 degrees in an immature patient (or 50+ in a mature patient), surgery is recommended. Posterior spinal fusion with instrumentation is standard. Surgery corrects and stabilizes the curve permanently. In adolescent idiopathic scoliosis, outcomes are excellent. Neuromuscular scoliosis may need surgery at lower Cobb angles due to faster progression.
🎯
Cobb thresholds on one card: <25° = watch. 25-40° + growing = brace. >40-45° = surgery. The Cobb angle is everything.
🔑25-40-45 rule: Watch / Brace / Cut. Under 25 = watch. 25-40 + growing = brace. Over 40-45 = surgery.
CLASSIFY IT
Decision Tree: Scoliosis Classification and Management
Work through the type and cause first, then follow the management branch.
What type of curve is this? Does it correct on the Adam's forward bend test or with lateral bending?
Structural scoliosis confirmed. Vertebral rotation is present (rib hump on forward bend). What is the cause?
Adolescent idiopathic scoliosis (AIS). Screen with Adam's forward bend test. Confirm with X-ray Cobb angle. What is the Cobb angle?
Observe. X-ray every 6 months during growth. No intervention needed unless curve progresses by 5 or more degrees on two consecutive films.
Bracing. Milwaukee brace (cervical to pelvis) or Boston brace (TLSO, more common now). Wear 16 to 23 hours per day. Goal: stop progression, not correct the curve. Risser sign 0 to 2 (still growing) = brace. Risser 4 to 5 (done growing) = observe only.
Surgical correction. Posterior spinal fusion with instrumentation. Corrects and permanently stabilizes the curve. Indicated when bracing fails or the patient presents late with a large curve.
Congenital scoliosis. High risk for rapid progression. Treat early. Surgical intervention often needed in childhood. Associated anomalies (cardiac, renal) must be ruled out.
Neuromuscular scoliosis. Typically C-shaped curve. Bracing is less effective due to poor muscle control. Surgery is indicated when the curve interferes with sitting balance or respiratory function. Lower Cobb threshold for surgery than idiopathic.
Functional scoliosis. No true vertebral rotation. Common causes: leg length discrepancy (pelvic tilt), paraspinal muscle spasm, antalgic posture from a herniated disc. Treat the underlying cause. OMT is highly effective here. Heel lift for leg length discrepancy. Reassess after correction.
OMT role: functional scoliosis responds well to treatment. Structural scoliosis responds less, but OMT addresses compensatory somatic dysfunctions and improves quality of life. Zink patterns are frequently present. Treat the compensatory dysfunctions even if the structural curve cannot be corrected.
PROVE IT
Board Walkthrough
Full clinical vignettes. One at a time. Cross out distractors, commit, then read every teaching line.
Medically reviewed by Fatima Ali, DO and Kaitlyn Cocuzzo, MD · Last updated July 5, 2026 at 8:04 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.