Everyone gets lost in sacral torsions. They shouldn't. The whole topic is six rules and one diagonal line. Start with the question that trips up most students.
Medically reviewed by Fatima Ali, DO
Before you scroll
A 28-year-old man presents with 3 days of low back pain after no specific injury. On exam, the standing and seated flexion tests are both positive on the right. The right sacral sulcus is deep, the left ILA is posterior, and the lumbosacral spring test is negative. What is the diagnosis?
Deep RIGHT sulcus means what for rotation?
The right base sank forward. Push the top-right corner of a card and its face rotates LEFT. Right base forward = sacrum rotated LEFT. Rotation is always opposite the deep sulcus.
Seated flexion positive RIGHT means which axis?
Seated flexion is positive on the side OPPOSITE the axis. Positive right = LEFT oblique axis.
Put it together.
Left rotation on the left axis = Left-on-Left. Same letters = forward, and the negative spring confirms it. Answer: Left-on-left forward torsion. L5 will be NRRSL.
Scroll ↓ the six rules come next
The Landmarks
Know the Parts
Every test and rule below names these landmarks. Learn them first. Tap each one.
The lever picture
The sacrum is a see-saw lever.
Picture a wedge-shaped bone slung between your two hip bones. The lumbosacral junction at the top (where your last spine bone sits on it) is the fulcrum the whole spine balances on. The base (top) and the ILAs (bottom corners) are the two ends of the lever, and the SI joints on each side are the hinges. Push one end and the other end swings the opposite way: that single idea is the entire topic.
Tap a landmark to see what it is and why it matters.
Top fulcrum = lumbosacral junction. Two lever ends = base (top) and ILAs (bottom). Two hinges = SI joints.
Start Here · The Core Model
The Sacral Diamond
Think of the sacrum as a stiff card. Push a top corner forward (away from you, toward the table) and the whole face turns the OTHER way: push the top-RIGHT corner, the face rotates LEFT. That pushed corner is now the deep sulcus. Do this until it's obvious, and you never memorize a table again.
Grab a top corner and pull it forward. Watch the groove and the far corner.
What just happened
When a base corner dives forward, your thumb sinks into a deep sulcus on that side. The diamond pivots on its diagonal, so the far bottom corner swings posterior (that's the ILA), and the whole face turns toward the opposite side. That is why deep-sulcus and posterior-ILA always land on opposite corners. That is a torsion.
The Six Decision Rules
The Six Rules
Six rules, each with the reason it's true and a hook to remember it. You should be able to explain WHY, not just recite.
Why: sitting plants the pelvis and takes the legs out of the motion, so only sacrum-on-pelvis movement shows up. Standing lets the legs drive the ilia, so you're testing the innominate. The PSIS that rises is the stuck side.
Seated = Sacrum (S = S). Standing on your legs = innominate.
POP QUIZStanding flexion is positive on the right, but the seated flexion test is negative. You still feel an asymmetric sulcus. Sacral or innominate?
Innominate. A negative seated flexion takes the sacrum off the table no matter how the landmarks feel: sitting removes the legs and isolates the sacrum, and it did not move. Asymmetric landmarks never override a negative seated flexion.
Rule 2 · Sulcus → rotation
Deep sulcus = base dove forward = sacrum rotated to the OPPOSITE side.
Why: the sulcus is the groove your thumb rests in next to the sacral base. When that base rotates anterior, it drops away from your thumb, so the groove feels deep. And because the whole bone pivots, the face turns the other way: push the top-right corner of a card and its face rotates left.
Deep = Dove away. Deep RIGHT sulcus → rotated LEFT.
POP QUIZYou palpate a deep LEFT sulcus. A classmate says "so the sacrum rotated LEFT, toward the deep side." Are they right?
No. The deep side is the corner that dove forward; the face turns the other way. Deep LEFT sulcus → rotated RIGHT. Rotation is opposite the deep sulcus, every single time.
Rule 3 · Seated flexion → axis
Seated flexion is positive OPPOSITE the oblique axis.
Why: the oblique axis is the locked diagonal the sacrum pivots on. The corner off that axis is free, so when the patient bends forward it gets dragged up and that PSIS rises. The free (positive) side is the one away from the axis.
The positive seated-flexion side points AWAY from the axis.
POP QUIZSeated flexion is positive on the LEFT and the right sulcus is deep. Which axis, and which way did the sacrum rotate?
Right axis (positive is opposite the axis) and rotated left (deep right sulcus). Put together, that is a Left-on-Right. The positive seated-flexion side names the axis on the OTHER side; the deep sulcus names the rotation on the other side. Both flip.
Rule 4 · Naming
Name it rotation-on-axis. Same letters = forward. Different = backward.
Both are dysfunctions. This only tells you which DIRECTION the sacrum is stuck. When the sacrum rotates toward the same side as the axis it is spinning on, the letters match (L-on-L) and it has gone forward (flexed/nutated): the everyday, gait-type torsion. When something twists it the opposite way from its axis, the letters differ (L-on-R) and it is locked backward (extended): the trauma-type. Forward vs backward is just stuck-forward vs stuck-back, and the spring test confirms which.
Letters MATCH = stuck Forward. Letters DIFFER = stuck Backward. (Both are dysfunctions; this is only direction.)
POP QUIZA sacrum is rotated LEFT on the RIGHT oblique axis. Forward or backward, and what is the spring test?
Different letters (L on R) = backward = positive spring. The exact same left rotation on the left axis would be forward with a negative spring. A left rotation is forward or backward depending entirely on the axis: the letters decide.
Rule 5 · The shape
Opposite sides = torsion. Same side = unilateral. Symmetric = bilateral.
Why: a twist on a diagonal throws the deep sulcus and the posterior ILA onto opposite corners (that's the Diamond you just dragged). One side simply nodding forward or back keeps both findings on the same side. Both sides equal means nothing feels asymmetric, so the seated-flexion test reads falsely negative.
Opposite corners = Twist. Same side = one-sided. Mirror image = both sides.
POP QUIZDeep RIGHT sulcus AND posterior RIGHT ILA, both on the same side. Torsion?
No. Deep sulcus + posterior ILA only spell torsion when they sit on opposite corners. Both on the same side is a unilateral dysfunction. It is the geometry, not the words: same side is one-sided, never a torsion.
Rule 6 · Spring / Sphinx
Feel it HARD? It is stuck further BACK. Feel it give? It can still go forward.
Dead simple: you press the sacral base forward. If it springs and gives, the sacrum still has room to go forward, so it is a forward (flexed) problem (negative spring). If you hit a hard wall, it is already jammed back in extension and cannot go forward, so it is a backward (extended) problem (positive spring). Hard wall = further back. That is the whole test.
Hard wall = stuck Back (positive = backward). Springy give = still Forward (negative = forward).
POP QUIZSeated AND standing flexion tests are both negative, but the spring test is positive and the patient cannot stand up straight. Is there a sacral dysfunction?
Yes. A bilateral dysfunction is symmetric, so it gives a false-negative seated flexion: both sides are equally stuck, so nothing reads as asymmetric. The positive spring is the only test that catches it. Negative flexion tests + positive spring + cannot straighten = bilateral.
The trap that kills everyone
L-on-L and L-on-R feel identical under your hands.
Both give a deep RIGHT sulcus + posterior LEFT ILA, because both are a left rotation. Palpation only tells you the rotation. The seated-flexion side reveals the axis and the spring test reveals forward vs backward. Skip either and you are guessing between a normal gait pattern and a traumatic lock.
Same hands-on findings ≠ same diagnosis. Always get the seated-flexion side AND the spring.
Build the Diagnosis Live
Oblique Axis Visualizer
Set the three findings. Watch the sacrum rotate, the axis light up, and the diagnosis name itself. This is the whole topic on one screen.
1 · Seated flexion positive on
→ the axis lands on the OPPOSITE side from this.
2 · Deep sacral sulcus on
3 · Lumbosacral spring test
Set all three findings above to build the diagnosis.
What each color means
Green dot = deep sulcus. That base rotated anterior, so your thumb sinks in. It marks the side the sacrum rotated AWAY from.
Red dot = posterior ILA. The far bottom corner that kicked backward as the sacrum twisted.
Purple line = the oblique axis. This is the diagonal HINGE the sacrum twists around in a torsion, and it is the axis you name. The axis is ALWAYS on the side opposite the positive seated-flexion test: positive on the right means a left axis, and vice versa. Watch the line jump to the other side each time you switch the seated-flexion button. The curved arrow shows which way the face turned.
Notice the geometry: the green deep sulcus and the red posterior ILA always land on opposite corners. That opposite-corner pattern is the signature of a torsion.
Every Possibility
The 8 Dysfunctions
Four torsions, two unilateral, two bilateral. Tap one to see its exact fingerprint.
Forward torsion · physiologic
Left-on-Left
Seated flexion +
RIGHT
Deep sulcus
RIGHT
Posterior ILA
LEFT
Axis
LEFT oblique
Spring
Negative
L5
NRRSL
Sacrum rotated LEFT (deep right sulcus), on the LEFT axis (seated flexion+ right). Same letters = forward. L5 rotates opposite the sacrum (right) and sidebends toward the axis (left).
Forward torsion · physiologic
Right-on-Right
Seated flexion +
LEFT
Deep sulcus
LEFT
Posterior ILA
RIGHT
Axis
RIGHT oblique
Spring
Negative
L5
NRLSR
Mirror of L-on-L. Sacrum rotated RIGHT (deep left sulcus), on the RIGHT axis (seated flexion+ left). Negative spring = forward.
Backward torsion · non-physiologic
Left-on-Right
Seated flexion +
LEFT
Deep sulcus
RIGHT
Posterior ILA
LEFT
Axis
RIGHT oblique
Spring
Positive
L5
FRRSR
Same palpation as L-on-L (deep right sulcus, posterior left ILA) but seated flexion+ is on the LEFT (right axis) and the spring is POSITIVE (backward). L5 is Type II (non-neutral): the grid shows FRRSR, but a backward torsion can equally be ERRSR, rotated and sidebent right.
Backward torsion · non-physiologic
Right-on-Left
Seated flexion +
RIGHT
Deep sulcus
LEFT
Posterior ILA
RIGHT
Axis
LEFT oblique
Spring
Positive
L5
FRLSL
Mirror of L-on-R. Same palpation as R-on-R (deep left sulcus, posterior right ILA) but seated flexion+ RIGHT (left axis) and POSITIVE spring (backward). L5 is Type II (non-neutral): the grid shows FRLSL, but a backward torsion can equally be ERLSL, rotated and sidebent left.
Unilateral · transverse axis
Unilateral Flexion
Seated flexion +
Affected side
Deep sulcus
Affected side
Posterior ILA
SAME (affected) side
Spring
Negative
Sphinx
Improves
Lordosis
Increased
Deep sulcus AND posterior/inferior ILA on the SAME side = unilateral, not torsion. The whole side nodded forward. Negative spring = flexion.
Unilateral · transverse axis
Unilateral Extension
Seated flexion +
Affected side
Shallow sulcus
Affected side
Anterior (deep) ILA
SAME (affected) side
Spring
Positive
Sphinx
Worsens
Lordosis
Decreased
Shallow sulcus AND anterior (deep) ILA on the SAME side. To separate from a backward torsion: check the ILAs. Same-side anterior ILA = unilateral extension; opposite-side = torsion.
Bilateral · both sides
Bilateral Flexion
Seated flexion
FALSE negative
Sulci
Deep, both sides
ILAs
Posterior, both sides
Spring
Negative
Lordosis
Increased
Key sign
Can't stand straight
Both sides symmetric = false-negative seated flexion. Deep sulci bilaterally + negative spring. Rowers, cyclists, sustained flexion.
Both flexion tests positive = the sacrum. Standing positive but seated negative = the innominate (iliosacral). An anterior innominate shows ASIS inferior + PSIS superior on that side (a long-leg look); a posterior innominate is the reverse.
POP QUIZStanding flexion positive on the right, seated negative, with the right ASIS inferior and right PSIS superior. Diagnosis?
Anterior right innominate. Seated negative takes the sacrum off the table, and ASIS-down + PSIS-up is an anterior innominate rotation. Standing-positive / seated-negative is always iliosacral, never a sacral torsion.
Unilateral vs backward torsion
Check the ILAs.
A shallow sulcus could be a unilateral extension or a backward torsion. The ILA decides: a deep (anterior) ILA on the same side as the shallow sulcus = unilateral extension. A deep ILA on the opposite side = torsion.
POP QUIZShallow LEFT sulcus. The LEFT ILA is deep (anterior). Torsion or unilateral?
Unilateral. The deep ILA is on the same side as the shallow sulcus, so it is a left unilateral extension. A deep ILA on the opposite side would make it a torsion. Same-side deep ILA = one-sided; opposite-side = twist.
Torsion vs bilateral
A positive seated flexion means it is not bilateral.
Torsions and unilaterals make one seated flexion positive. Bilateral dysfunction is symmetric, so the seated flexion reads falsely negative and only the spring test (plus a patient who cannot stand straight, often with a pelvic side-shift and apparent long leg) gives it away.
POP QUIZBoth flexion tests negative, deep sulci bilaterally, negative spring, cannot stand straight. Category?
Bilateral flexion. Symmetric restriction gives a false-negative seated flexion; deep sulci + a negative spring point to flexion. Negative flexion tests with real symptoms = bilateral, and the sulci + spring tell you flexion vs extension.
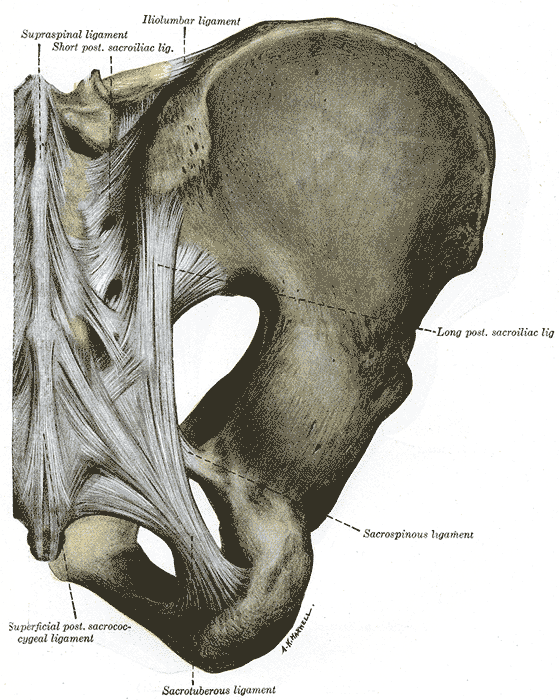
Why it matters clinically · tap a ligament
Tap a ligament to light it up and learn who strains it and when it is most likely the culprit.
Posterior pelvis ligaments (public domain). Tap to enlarge.
POP QUIZA woman has chronic pelvic pain and uterine retroversion, and you find a sacral somatic dysfunction. Which ligament links the two?
Uterosacral. It tethers the cervix to the sacrum, so a sacral dysfunction stretches it and refers pelvic pain. The sacrotuberous resists nutation but has no uterine attachment. Uterosacral = the sacrum-to-pelvic-pain bridge.
Run the Algorithm
Diagnose a Case
Walk one case through the rules, one step at a time. Build the answer yourself.
Muscle Energy
Treatment
One rule covers most of it: the axis side always goes DOWN. After that, forward and backward split.
The one rule
Axis side DOWN. Forward = face down, push ankles. Backward = face up, push knee.
Why axis-side-down: the oblique axis is the hinge the sacrum is stuck on. Lay the patient on that side so the axis corner is pinned to the table and cannot move; now gravity and the free leg can unwind the twist around it. Why the patient does the work: their muscle contraction (you just resist) is what rotates the sacrum off the axis: push, you resist 3-5 seconds, relax, take up the new slack.
Pin the hinge (axis down), then let the patient's own muscles unwind the twist.
Forward torsion (L-on-L, R-on-R)▼
PositionModified Sims, axis side DOWN, patient face DOWN (forehead toward the table).
SetupBoth legs hang off the table edge to add sidebending. Flex to engage the lumbosacral junction.
ForcePatient lifts both feet toward the ceiling against your resistance. 3-5 sec hold, 3-5 reps.
WhyA forward torsion is physiologic and follows gait. Face down with the legs dropped lets gravity and the leg-lift carry the sacrum back along its axis toward neutral. The ankle lift is the lever because the legs are long and extended off the table.
MemoryFORWARD = FACE DOWN (FOREHEAD on the table). Push the ankles.
Backward torsion (L-on-R, R-on-L)▼
PositionLateral recumbent, axis side DOWN, patient face UP (back toward you).
SetupHips flexed roughly 30 degrees to the extension barrier; top leg dropped off the table.
ForcePatient pushes the top knee up against your resistance. 3-5 sec hold, 3-5 reps.
WhyA backward torsion is stuck in extension and non-physiologic. Turning the patient face up and flexing the hips opens that extension barrier, and pushing the bent knee recruits the piriformis to pull the sacrum forward and derotate it. The bent knee is the lever because the hips are flexed.
MemoryBACKWARD = BACK DOWN (face up). Push the knee.
Unilateral flexion▼
PositionProne. Hypothenar on the affected ILA.
ForceAnterior pressure on the ILA during INHALATION; resist on exhalation. Repeat 3-5 cycles.
Why inhaleThe sacrum rides the breath: on inhalation it EXTENDS (counter-nutates) so the base rocks posterior and the ILA swings anterior. A unilateral flexion is stuck FLEXED (base anterior), so you treat it on the breath that pulls it the other way. Pushing the ILA anterior on inhalation rides that built-in extension, then you hold the gain on exhalation so it cannot flex back.
MemoryINHALE = sacrum EXTENDS. So a FLEXED sacrum is treated on the IN-breath (opposite breath fixes the dysfunction).
Unilateral extension▼
PositionProne. Hypothenar on the affected sacral base.
ForceAnterior pressure on the base during EXHALATION; patient inhales and resists. Follow anteriorly on exhale. 3-5 cycles.
Why exhaleMirror image: on exhalation the sacrum FLEXES (nutates) so the base rocks anterior. A unilateral extension is stuck EXTENDED (base posterior), so you ride the exhale that carries the base forward, then follow it anteriorly each cycle.
MemoryEXHALE = sacrum FLEXES. So an EXTENDED sacrum is treated on the OUT-breath. (Flexed = inhale, Extended = exhale: always the opposite breath.)
Bilateral flexion / extension▼
FlexionSupine, knees flexed; hyperflex toward chest to engage the LSJ; patient pushes knees away against resistance.
ExtensionProne sphinx; thenar on the sacral base; anterior pressure on exhale; patient inhales and resists.
WhyBoth sides are stuck the same way, so you just push the whole sacrum the OTHER way. A bilateral flexion is stuck nutated forward, so you drive it into extension (knees to chest tips the sacral base back). A bilateral extension is stuck back, so you push the base forward on the exhale to flex it. You are simply taking it the opposite direction of where it is jammed.
MemoryStuck flexed, push it extended. Stuck extended, push it flexed. Treat the opposite of where it is stuck.
Clinical Anatomy
Anatomy
Where you actually put your hands: the sacral base (sulci) and the inferior lateral angles.
Read top to bottom and you can derive any sacral case. No table to memorize.
1 · Which test. Both flexion tests positive = sacrum. Standing-only = innominate. The positive side is the restricted side.
2 · Deep = Dove (rotation). A deep sulcus = that base dove forward; the sacrum rotated to the OPPOSITE side. Deep RIGHT → rotated LEFT. (Push a card's top-right corner: its face turns left.)
3 · Away from the axis. The oblique axis is OPPOSITE the positive seated-flexion side. Positive RIGHT → LEFT axis.
4 · Letters = direction (both are dysfunctions). Same letters (L-on-L) = stuck FORWARD/flexed. Different (L-on-R) = stuck BACKWARD/extended.
5 · Spring confirms. Springy = it can still go forward (FORWARD). Hard wall = jammed back (BACKWARD). Sphinx: forward eases, backward worsens.
6 · Corners = the shape. Opposite corners = torsion. Same side = unilateral. Symmetric = bilateral (false-negative seated flexion).
7 · L5 follows Fryette. L5 rotates OPPOSITE the sacrum, sidebends TOWARD the axis. Forward = Type I (NR, opposite). Backward = Type II (FRS or ERS, same).
8 · Treat it. Axis side DOWN, always. Forward = face down, push the ankles. Backward = face up, push the knee.
clinical Practice
25 Vignettes
All 25, one at a time, in a shuffled order. Progress saves to your account on this device, so you can pick up where you left off. Cross out (right-click / long-press) and highlight (select text) as you go.
1 / 8
References
Greenman PE. Principles of Manual Medicine. Sacral and pelvic mechanics, oblique axes, seated flexion testing.
Nicholas AS, Nicholas EA. Atlas of Osteopathic Techniques. Sacral muscle energy positioning.
Savarese RG. OMT Review. Sacral torsion diagnosis and naming conventions.
DiGiovanna EL, Schiowitz S, Dowling DJ. An Osteopathic Approach to Diagnosis and Treatment. Sacral somatic dysfunction.
Chila AG, ed. Osteopathic Medicine (comprehensive text), 3rd ed. Pelvic and sacral dysfunction.
Reviewed by Fatima Ali DO and Kaitlyn Cocuzzo MD. Vignettes are clinical teaching cases; demographics and answer order are altered for original practice.
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.
That was the free half
You understand it. Now make it automatic.
The Diamond and the six rules are yours free. Everything that turns "I get it" into a 10-second answer on exam day lives in Elite:
Build any torsion live on the Axis Visualizer
All 8 dysfunctions, plus how to split the look-alikes