THE FOUNDATION
Fryette's Three Laws
Every spinal dysfunction question on the board reduces to these three rules. Tap each law to expand.
When the spine is in neutral (not flexed or extended), sidebending to one side causes rotation to the opposite side. This always involves a group of vertebrae.
Clinical example: L2-L5 all sidebent right, rotated left. That is a Type 1 group curve: NSRRL. Multiple vertebrae, neutral spine, opposite directions.
Memory anchor: Think of a group of people all leaning one way but looking the other way. That's Type 1: the crowd leans together, looks opposite.
When the spine is flexed or extended (non-neutral), sidebending and rotation go to the same side. This involves a single vertebra.
Clinical example: L4 alone is flexed, rotated left, sidebent left. That is Type 2: FRSL. Single vertebra, non-neutral, same direction.
Memory anchor: One person, one direction. When you're bending forward or backward, you rotate and lean the same way. Type 2 = solo, same side.
Introducing motion in one plane of the spine reduces the ability to move in the other planes. This is why positioning matters for treatment.
Clinical meaning: If you flex the spine (sagittal plane motion), the ability to rotate and sidebend decreases. This principle is used during muscle energy technique: you stack barriers in all three planes to engage the restrictive barrier precisely.
Board angle: Law 3 explains why locking techniques work. When you flex or extend a patient to engage one plane, you reduce slack in the other planes, allowing you to target a specific segment.
THE COMPARISON
Type 1 vs Type 2
Toggle between the two types. Know the differences cold.
THE METHOD
How to Read L5 Findings
Four steps. Works every time. Tap each step to expand.
Neutral = no flexion or extension noted. Look for whether the segment is described as part of a group. If L5 is moving with L3 and L4, and the spine is neutral, you are in Type 1 territory.
Flexed or Extended = the segment is locked. If the stem says "L5 is flexed" or "L5 is extended," you are in Type 2 territory. Only L5 is involved, and it is stuck.
Physical exam clue: In seated flexion test, if the segment's transverse process asymmetry worsens in flexion, it is FRS. If it worsens in extension, it is ERS. If neither change makes one side more prominent than the other, suspect neutral (Type 1).
The vertebra is named as rotated toward the side of the more posterior (prominent) transverse process.
Example: If the right transverse process of L5 is more posterior than the left, L5 is rotated RIGHT. The vertebral body has turned so its right side moves back and its left side moves forward.
The vertebra is sidebent toward the concavity (the side that is shorter or compressed).
Example: If L5's left side is compressed and right side is open, L5 is sidebent LEFT. On a question stem, this is usually stated directly.
SAME direction (L5 rotation and sidebending match): Type 2 = non-neutral = backward sacral torsion. Rotation occurs OPPOSITE the oblique axis (L-on-R or R-on-L). Spring test is POSITIVE.
OPPOSITE directions (L5 rotation and sidebending differ): Type 1 = neutral = forward sacral torsion. Rotation occurs ON THE SAME SIDE as the oblique axis (L-on-L or R-on-R). Spring test is NEGATIVE.
The cheat: L5 same-side = backward. L5 opposite-side = forward. To name the torsion, remember the sacrum and L5 always rotate in OPPOSITE directions.
PRACTICE EXAMPLES
Neutral + opposite directions (sidebent R, rotated L) = Type 1.
Associated with a forward sacral torsion. The sacral axis and rotation direction match.
Flexed + same direction (rotated L, sidebent L) = Type 2.
Associated with a backward sacral torsion (L-on-R or R-on-L).
Extended + same direction (rotated R, sidebent R) = Type 2.
Associated with a backward sacral torsion.
THE LINK
The Sacral Connection
L5 findings tell you the sacral torsion type. Tap any connection to see the logic.
The sacrum sits directly below L5. The way L5 behaves tells you what the sacrum is doing. This is one of the most tested relationships in clinical practice.
L5 is in a neutral group curve (Type 1). Sidebending and rotation go in opposite directions.
This correlates with a forward (physiologic) sacral torsion: rotation occurs on the SAME side as the oblique axis (L-on-L or R-on-R). Spring test is NEGATIVE; sphinx test IMPROVES the asymmetry.
Forward torsions: Left-on-Left (L-on-L) or Right-on-Right (R-on-R). These are physiologic and occur during normal gait.
Example: L5 NSLRR. Sacrum and L5 always rotate in opposite directions, so an L5 rotated right means the sacrum rotates left. Left rotation on the left oblique axis = L-on-L forward torsion. Deep sacral sulcus would be on the right (opposite the axis in a forward torsion).
L5 is non-neutral (flexed or extended) with rotation and sidebending going the same direction (Type 2, FRS or ERS).
This correlates with a backward (non-physiologic) sacral torsion: rotation occurs OPPOSITE the oblique axis. Spring test is POSITIVE; sphinx test WORSENS the asymmetry.
Backward torsions: Left-on-Right (L-on-R) or Right-on-Left (R-on-L). These are non-physiologic and do not occur during normal gait.
Example: L5 FRSL. Sacrum rotates opposite L5: L5 rotated left means the sacrum rotates right. Right rotation on the left oblique axis (axis and rotation opposite) = R-on-L backward torsion. Deep sacral sulcus would be on the left (same side as the axis in a backward torsion).
Forward Torsions
- L-on-L: Left rotation on left oblique axis
- R-on-R: Right rotation on right oblique axis
- Axis and direction MATCH
- Associated with L5 Type 1 (NSR)
- Physiologic: occurs during normal gait
Backward Torsions
- L-on-R: Left rotation on right oblique axis
- R-on-L: Right rotation on left oblique axis
- Axis and direction OPPOSITE
- Associated with L5 Type 2 (FRS)
- Non-physiologic: does NOT occur in gait
APPLY IT
Diagnosis Practice
Four cases. Identify the dysfunction and connect the findings.
Structural exam of the lumbar spine reveals that L3, L4, and L5 are all sidebent left and rotated right. The lumbar spine is in a neutral position. There is no single-segment asymmetry noted.
Three vertebrae (L3-L5) are involved. The spine is neutral. Sidebending (left) and rotation (right) go in opposite directions. This is textbook Fryette's Law 1.
Sacral connection: L5 Type 1 points to a forward sacral torsion. The sacrum and L5 always rotate in opposite directions, so an L5 rotated right means the sacrum rotates left. Left rotation on a left oblique axis = L-on-L forward torsion. The deep sacral sulcus would be on the right (opposite the axis in a forward torsion).
A patient bends forward and the examiner notes that the left transverse process of L4 becomes significantly more posterior than the right. This asymmetry was not present in neutral or extension. Only L4 shows this finding.
Single vertebra (L4 alone). The asymmetry worsens in flexion, meaning L4 is stuck in flexion. The left transverse process is posterior, so L4 is rotated left. In Type 2, rotation and sidebending go the same direction, so L4 is also sidebent left.
Key exam principle: The position that makes the asymmetry worse tells you what the vertebra is stuck in. Worse in flexion = FRS. Worse in extension = ERS.
With the patient prone, the examiner springs L2 and notes resistance. In extension, the right transverse process of L2 is more posterior than the left. This asymmetry was minimal in neutral and flexion.
Single vertebra (L2 alone). Asymmetry worsens in extension, meaning L2 is stuck in extension. Right transverse process is posterior = rotated right. Same-side rule: also sidebent right.
Treatment direction: For muscle energy, you would position L2 into flexion (opposite of stuck position), then sidebend LEFT and rotate LEFT to engage the barrier. The patient pushes against your resistance, then you take up the new barrier. Always move toward the barrier, not away from it.
A patient has chronic low back pain. L5 is flexed, rotated right, and sidebent right. The seated flexion test is positive on the left. A deep sacral sulcus is palpated on the right. The left ILA is posterior and inferior. The lumbosacral spring test is positive.
L5 is flexed with rotation and sidebending going to the same side (right) = Type 2.
Type 2 at L5 predicts a backward torsion. The sacrum and L5 always rotate in opposite directions, so L5 rotated right means the sacrum rotates left. For a backward torsion, the axis and rotation are opposite: left rotation on a right oblique axis = Left-on-Right (L-on-R) backward torsion.
Confirm with sacral findings: In L-on-R, deep sulcus is on the right (same side as axis in a backward torsion), the posterior-inferior ILA is on the left, and the seated flexion test is positive on the left (contralateral to the right oblique axis). The positive spring test confirms backward sacral mechanics.
THE LINEUP
Lumbar Dysfunctions
Tap to flip.
Type I Neutral
- Law: Fryette Law I: neutral mechanics
- Segments: Multiple (group dysfunction)
- Directions: Sidebending and rotation are OPPOSITE (convexity = sidebending side, rotation = opposite)
- Cause: Postural, adaptive (carrying a bag, compensatory)
- Notation: N (neutral) S (side) R (rotation to opposite side)
- Rx: Treat the entire group
Type II Non-Neutral
- Law: Fryette Law II: non-neutral mechanics
- Segments: Single (key segment)
- Directions: Sidebending and rotation are SAME direction
- Cause: Traumatic, sudden loading, acute injury
- Position: Flexed (F) or extended (E) out of neutral
- Rx: Treat the key dysfunctional segment
Flexed Somatic Dysfunction
- Position: Segment stuck in flexion
- Opens: Posteriorly in flexion (facets gap open, spinous diverge)
- Restricted: Cannot extend fully
- Notation: FRSR = Flexed, Rotated Right, Sidebent Right
- Rx: Treat in flexion (MET, counterstrain in flexed position)
Extended Somatic Dysfunction
- Position: Segment stuck in extension
- Opens: Anteriorly in extension (facets load, disc opens anteriorly)
- Restricted: Cannot flex fully
- Notation: ERSR = Extended, Rotated Right, Sidebent Right
- Rx: Treat in extension (HVLA or MET in extended position)
L4-L5 Herniation
- Level: Posterolateral herniation most common
- L4 root: medial calf, knee jerk reduced, quad weakness
- L5 root: dorsal foot, dorsiflexion weakness, no reflex change
- SLR: Positive (straight leg raise reproduces radicular pain)
- Board pearl: Foot drop = L5; absent knee jerk = L4
L5-S1 Herniation
- Root: S1 dermatome (lateral foot, heel, lateral calf)
- Reflex: Ankle jerk reduced or absent
- Weakness: Plantar flexion (gastrocnemius, soleus)
- SLR: Positive
- Board pearl: Absent ankle jerk = S1. Combine with lateral foot pain = L5-S1.
Facet Syndrome
- Pain: Worsens with extension and lateral flexion toward the painful side
- Pattern: Local low back pain, may refer to buttock or thigh, but no dermatomal distribution
- Who: Older patient, degenerative facets
- No: neurological deficits, positive SLR
- Rx: OMT, NSAIDs, facet injection if needed
ALGORITHM
Decision Tree: Naming a Lumbar SD
Tap through the steps.
VISUAL REFERENCE
Lumbar Anatomy Reference
Swipe to browse. Wikimedia Commons.
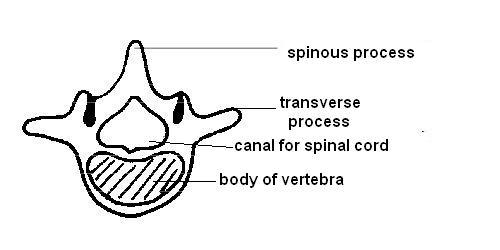 Lumbar vertebra anatomy
Lumbar vertebra anatomy
TEST YOURSELF
clinical Quiz
5 original questions. Type identification, notation, sacral connections, treatment direction.
