Lower Extremity · Nerve Injuries
Six nerves. Six patterns of injury. Master the anatomy and you will never confuse foot drop with Trendelenburg again.
Anatomy
The lumbosacral plexus (L2-S3) generates six nerves. Each has a unique anatomic pinch point and a unique injury signature. Tap a nerve to see its territory.
Clinical Challenge
Read the clinical scenario. Identify the nerve before choosing. The anatomy is the answer.
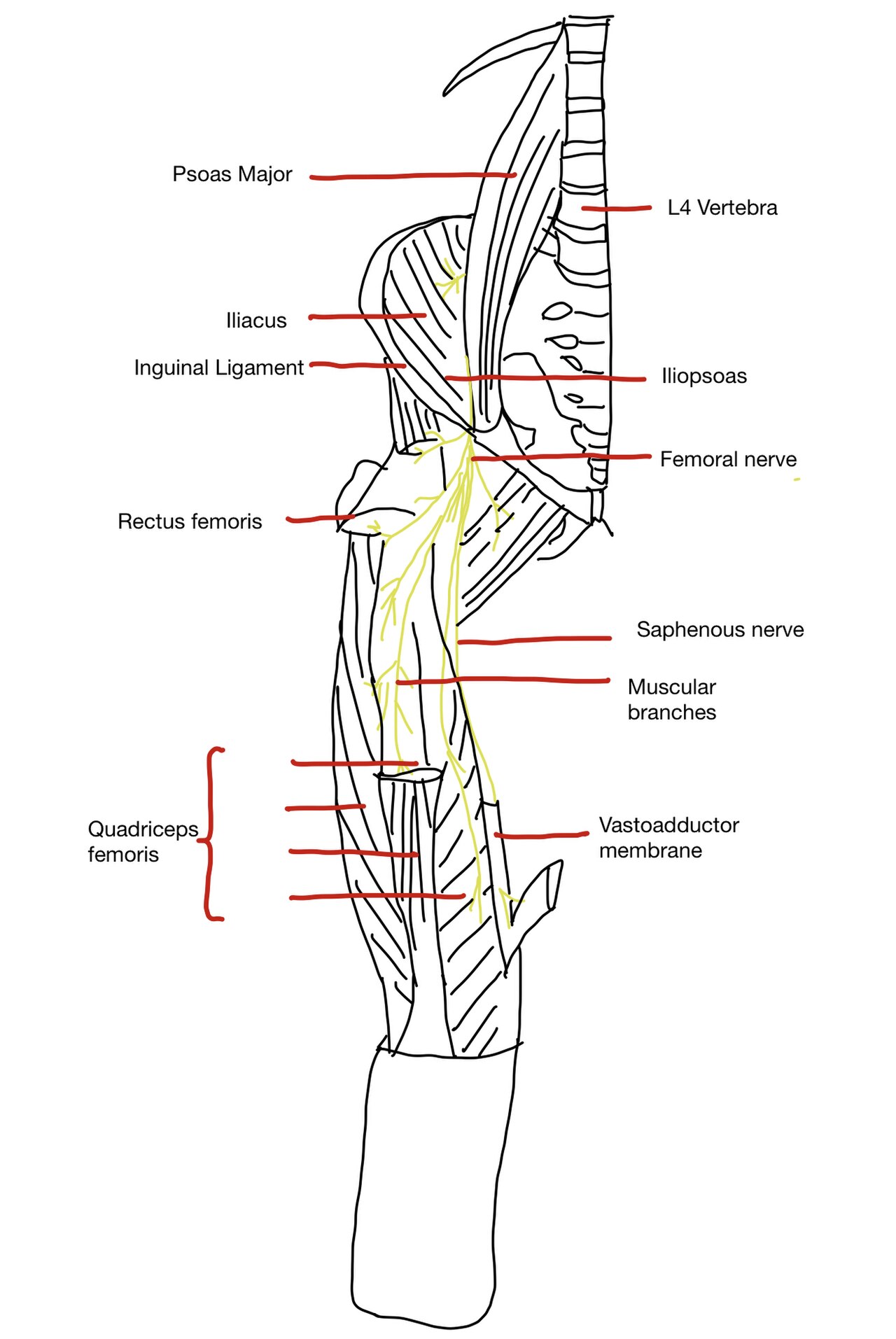
Anatomy Reference
Tap any image to view full size. Source: Wikimedia Commons public domain anatomical plates.


Clinical Pearls
| Root | Sensory territory | Motor loss | Reflex |
|---|---|---|---|
| L2-L3 | Anterior/medial thigh | Hip flexion (partial) | None |
| L4 | Medial leg, medial malleolus | Dorsiflexion weakness | Patellar |
| L5 | Lateral leg, dorsal foot, great toe | Dorsiflexion, hip abduction | None (or medial hamstring) |
| S1 | Lateral malleolus, lateral foot, sole | Plantarflexion weakness | Achilles |
| S2-S4 | Posterior thigh, perineum, perianal | Sphincter (S2-S4) | Bulbocavernosus |
Board Walkthrough
Each vignette contains exactly one final question and a tap-to-reveal teaching chain after answering. Shuffle with the remix button.