The pelvis is a seesaw. The hip is the fulcrum. Once you see it, you will never miss the diagnosis again.
🆕 OPENER · Can you crack it?
A 32-year-old runner comes in with chronic low back pain that is worse on the right side. Standing flexion test is positive on the right. On landmark assessment, the right ASIS is inferior and the right PSIS is superior compared to the left. What is the most likely somatic dysfunction?
Correct. Standing flexion test positive on the right tells you the RIGHT innominate is dysfunctional. Right ASIS inferior + right PSIS superior means the innominate has tipped forward: that is anterior rotation. Think of the seesaw: ASIS goes down (the front of the bone dips forward and inferiorly), PSIS goes up. The acetabulum gets pushed downward, making the leg appear longer.
Two-step system: Step 1, the standing flexion test tells you WHICH SIDE. It is positive on the right, so the right innominate is the problem. Step 2, ASIS and PSIS tell you the DIRECTION. Right ASIS is inferior and right PSIS is superior. The ASIS moved down and the PSIS moved up. That is the seesaw tipping forward: the front of the bone drops inferiorly = anterior rotation. Try again or tap B.
THE MODEL
The Innominate Seesaw
Tap a rotation to watch it happen. The hip joint is the fulcrum.
Neutral position. The ASIS and PSIS are level. The innominate sits balanced on the hip joint like a seesaw at rest.
🔥
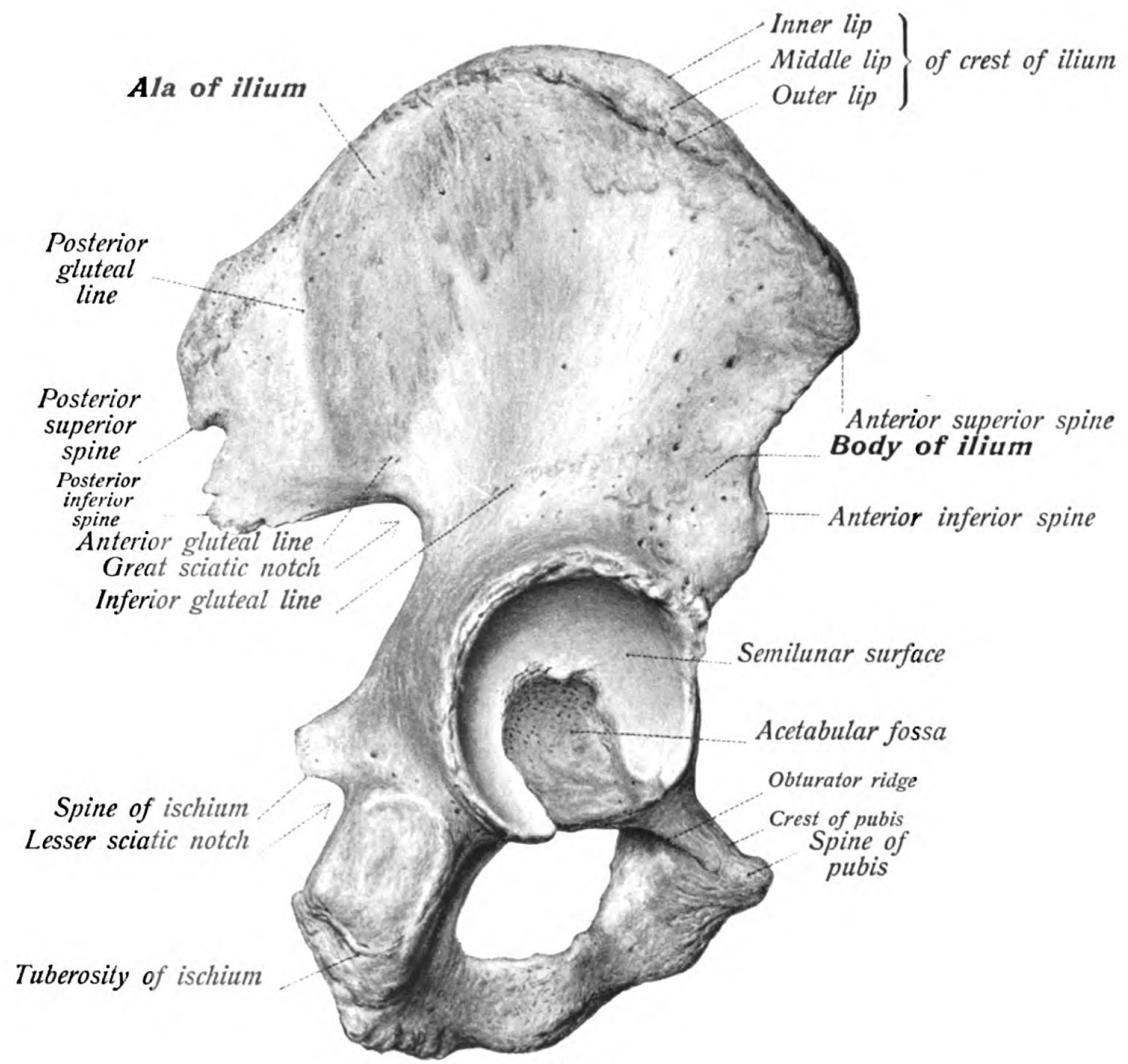
The innominate is a flat bone that pivots around the hip joint (acetabulum)The acetabulum is where the femoral head sits. This is the pivot point for innominate rotation. Everything else moves relative to it.. The ASIS is the front handle of the seesaw. The PSIS is the back handle. When one goes up, the other must go down.
💥Anterior rotation: ASIS goes inferior, PSIS goes superior, leg appears longer (the bone tips forward, pushing the acetabulum down).
💥Posterior rotation: ASIS goes superior, PSIS goes inferior, leg appears shorter (the bone tips backward, pulling the acetabulum up).
📷 ASIS: anterior superior iliac spine · tap to expand
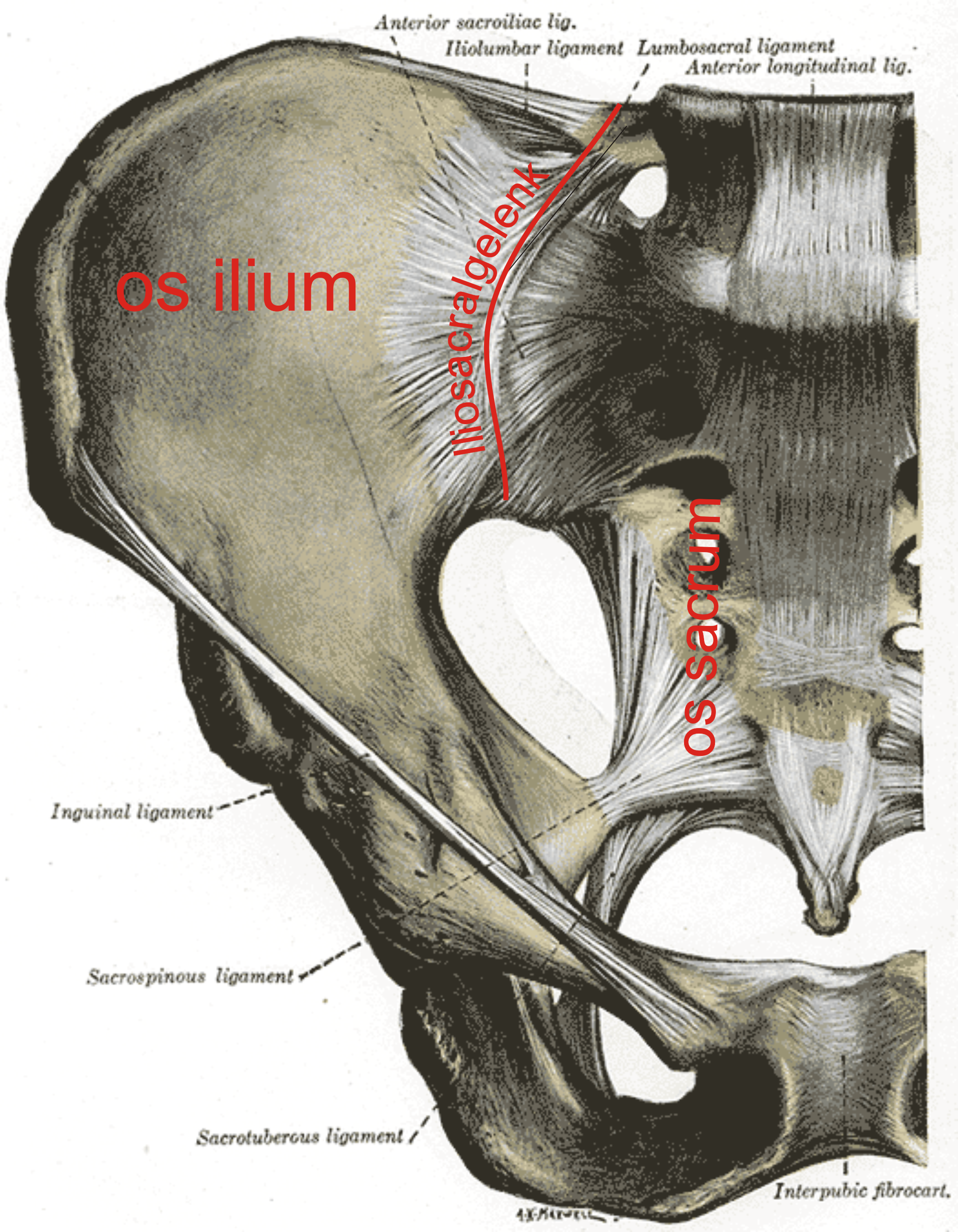
📷 Sacroiliac joint: fulcrum of innominate rotation · tap to expand
THE DYSFUNCTIONS
Rotation Profiles
Each card front: the single diagnostic clue. Flip to get tissue texture, ROM restriction, leg length, and treatment direction.🔑clinical medicine test ONE distinguishing clue per rotation. ASIS inferior = anterior. ASIS superior = posterior. Lock that in before you flip.
💥
Anterior Innominate Rotation
ASIS inferior. PSIS superior. Leg appears longer.🔑The bone tips FORWARD: the front drops down (ASIS inferior), the back rides up (PSIS superior). The acetabulum pushes down, making the leg look longer. Hip flexors are the culprit.
tap to flip
Anterior Innominate Rotation
LandmarksASIS inferior (low), PSIS superior (high) on dysfunctional side
Leg LengthAppears longer (acetabulum pushed inferiorly)
ROM RestrictHip extension restricted; patient cannot fully extend on that side
Tissue TextureTight hip flexors (iliopsoas, rectus femoris); anterior hip fullness
Pubic BonePubic tubercle inferior on dysfunctional side
TreatmentHip FLEXION muscle energy: flex hip to barrier, patient pushes into extension, take up slack
🔄
Posterior Innominate Rotation
ASIS superior. PSIS inferior. Leg appears shorter.🔑The bone tips BACKWARD: the front rides up (ASIS superior), the back drops down (PSIS inferior). The acetabulum pulls up, making the leg look shorter. Hamstrings and glutes are the culprits.
tap to flip
Posterior Innominate Rotation
LandmarksASIS superior (high), PSIS inferior (low) on dysfunctional side
Leg LengthAppears shorter (acetabulum pulled superiorly)
ROM RestrictHip flexion restricted; patient cannot fully flex on that side
Tissue TextureTight hamstrings and glutes; posterior hip fullness and tenderness
Pubic BonePubic tubercle superior on dysfunctional side
TreatmentHip EXTENSION muscle energy: leg off table in extension, patient pushes into flexion, take up slack
⚠️
The Board Trap
Standing flex positive RIGHT. "LEFT ASIS is more inferior." What is the dysfunction?🔑If LEFT ASIS is inferior, then RIGHT ASIS is superior by comparison. The test is positive RIGHT = right innominate is dysfunctional. Right ASIS superior = posterior rotation. Trap defused.
tap to flip
The Side Trap
Step 1Standing flexion test positive RIGHT = RIGHT innominate is the dysfunction
Step 2LEFT ASIS inferior means RIGHT ASIS is relatively SUPERIOR
Step 3On the RIGHT (positive) side: ASIS superior = posterior rotation
AnswerRIGHT posterior innominate rotation
RuleAlways name the dysfunction from the positive flexion test side, not from the described side
THE DIAGNOSIS
The 3-Step System
Tap each step to expand. This is the entire diagnostic algorithm.
Step 1 · Find the Side
Standing Flexion Test = THE SIDE
The positive side is the dysfunctional innominate.
Have the patient stand, feet shoulder-width apart. Place your thumbs on the inferior slopes of the PSIS bilaterally. Ask the patient to bend forward slowly. Watch which thumb moves first and/or travels further superiorly. That side is the positive side.
Why it works: When the patient bends forward, the sacrum should nutate (rock forward) and the innominates should move symmetrically. A restricted innominate gets "dragged along" with the sacrum instead of moving independently, causing that side's PSIS to ride higher.
Board pearl: Standing flexion test = innominate dysfunction. Seated flexion test = sacral dysfunction. If the stem says STANDING, you are in innominate territory. If it says SEATED, think sacral torsion.
Step 2 · Find the Direction
ASIS + PSIS Position = THE DIRECTION
Landmark heights tell you anterior vs posterior.
On the POSITIVE side (from Step 1), check ASIS and PSIS height compared to the other side:
ASIS inferior + PSIS superior = Anterior rotation
The bone tipped forward. The front (ASIS) swung downward and forward, the back (PSIS) swung upward.
ASIS superior + PSIS inferior = Posterior rotation
The bone tipped backward. The front (ASIS) swung upward, the back (PSIS) swung downward.
Memory trick: "ASIS follows the tilt." Anterior = the bone tilts forward, so the ASIS drops (inferior). Posterior = the bone tilts backward, so the ASIS rises (superior). Think of a seesaw: the side that tips down is the direction of the rotation.
Step 3 · Watch the Wording
clinical medicine Describe from the WRONG Side
They tell you about the OPPOSITE side to trip you up.
This is the single most common board trap for innominate rotations. The question stem will say something like: "The LEFT ASIS is more inferior compared to the right." Your instinct is to focus on the left. But check: where is the standing flexion test positive?
If the standing flexion test is positive on the RIGHT, then the RIGHT innominate is dysfunctional. The LEFT ASIS being low is just describing what the normal side looks like relative to the abnormal side.
Rule: Always start with the standing flexion test. The positive side IS the dysfunction. ASIS/PSIS positions only tell you the direction ON THAT SIDE. Ignore everything described about the other side.
⚠️
Board Trap: Standing vs Seated Flexion
Standing flexion test tells you the innominate. Seated flexion test tells you the sacrum. If both are positive on the same side, the innominate is "dragging" the sacrum along. The clinical medicine love mixing these up. Read the stem carefully: STANDING = innominate. SEATED = sacral torsion. If they do not specify, and you see ASIS/PSIS landmarks, it is innominate.
THE TRAP
The Side Trap
The same landmarks can mean two different diagnoses depending on the standing flexion test
Exam finding: "ASIS is more superior on the LEFT." Tap each scenario to see what it means.
SCENARIO A
Standing flexion: Positive LEFT
The LEFT innominate is dysfunctional. LEFT ASIS is superior. That means the front of the LEFT innominate went up = LEFT posterior innominate rotation.
LEFT ASIS: SuperiorLEFT PSIS: InferiorLeg: Appears shorter on LEFT
✅ Straightforward case. Positive side = same side the ASIS is high on. ASIS superior = posterior rotation. No trap here.
SCENARIO B · THE TRAP
Standing flexion: Positive RIGHT
The RIGHT innominate is dysfunctional. But the exam says the LEFT ASIS is superior. Wait: if the LEFT ASIS appears higher, the RIGHT ASIS must appear lower (inferior). On the positive (right) side, ASIS is inferior = RIGHT anterior innominate rotation.
RIGHT ASIS: InferiorRIGHT PSIS: SuperiorLeg: Appears longer on RIGHT
⚠️ THIS is the board trap. They described the LEFT side, but the dysfunction is on the RIGHT. You MUST start with the standing flexion test, not the landmarks.
⚠️
The Golden Rule
Never name the dysfunction from the described side. Always name it from the standing flexion test side. The clinical medicine describe landmarks from whatever angle makes you pick the wrong answer. The standing flexion test is the anchor. Start there, then translate the landmarks to that side.
THE ALGORITHM
Workup Decision Tree
Walk each step before the next reveals. This is the full diagnostic sequence.🔑Three sequential questions: Which side? Which direction? What does the sacrum do? Answer in order and you will never name the wrong dysfunction.
ChallengeBefore you reveal the rotation, which test names the dysfunctional side?
Standing flexion names the innominate side. Seated flexion moves you into sacral diagnosis.
Next nodeOnce the side is named, which landmark gives direction?
ASIS is the steering wheel for innominate rotations. Inferior ASIS tips forward. Superior ASIS tips backward.
THE FIX
Muscle Energy Treatment
Tap each card to see the full setup, action, and why it works
Anterior Rotation
Hip Flexion ME
Patient supine, hip and knee flexed to the barrier. Patient pushes leg DOWN (into extension) against your resistance.
Setup: Patient supine. Affected leg flexed at the hip and knee until you feel the restrictive barrier.
Patient action: "Push your foot down toward the table" (hip extension). You resist. Isometric contraction for 3-5 seconds.
Your action: After the contraction, take the hip further into flexion (take up the slack). Repeat 3-5 times.
Why it works: In anterior rotation, the ASIS is inferior (the bone tipped forward). Flexing the hip drives the ASIS back superiorly, tipping the bone posteriorly to correct the anterior rotation. You are reversing the seesaw.
Memory: Anterior rotation = hip flexion ME. The bone tipped forward, so you push it backward with flexion.
Posterior Rotation
Hip Extension ME
Patient supine, leg hanging off table in extension. Patient pushes leg UP (into flexion) against your resistance.
Setup: Patient supine. Affected leg hanging off the table edge with hip in extension. Opposite leg flexed at the hip and knee (patient holds it to their chest to stabilize the pelvis).
Patient action: "Push your leg up toward the ceiling" (hip flexion). You resist. Isometric contraction for 3-5 seconds.
Your action: After the contraction, take the leg further into extension (take up the slack). Repeat 3-5 times.
Why it works: In posterior rotation, the ASIS is superior (the bone tipped backward). Extending the hip pulls the ASIS inferiorly, tipping the bone forward to correct the posterior rotation. You are reversing the seesaw.
Memory: Posterior rotation = hip extension ME. The bone went backward, so you pull it forward with extension.
MUSCLE ENERGY PRINCIPLES
Direct vs Indirect: Muscle energy is a direct technique. You position the patient INTO the restrictive barrier (the direction they cannot go freely), then use their own muscle contraction against your resistance to engage and release the barrier.
Isometric contraction: The patient pushes AGAINST you. You do not let them move. This is isometric: same length, muscle fires but the joint stays still. After 3-5 seconds of effort, the muscle's Golgi tendon organ fires and the muscle reflexively relaxes. You take up the new slack.
Repetitions: 3-5 reps. Each time, you move further into the barrier as the muscle releases. The endpoint is when tissue tension equalizes or movement normalizes.
💥Quick recall: Anterior rotation = hip flexion ME (push ASIS back up). Posterior rotation = hip extension ME (pull ASIS back down). The treatment reverses the seesaw.
THE DETAILS
Associated Findings
What else changes with each rotation
Anterior Rotation
Posterior Rotation
Leg Length
Appears longer
Appears shorter
ASIS
Inferior (low)
Superior (high)
PSIS
Superior (high)
Inferior (low)
Medial Malleolus
More inferior (longer)
More superior (shorter)
Pubic Tubercle
Inferior on dysfunctional side
Superior on dysfunctional side
Ischial Tuberosity
Superior on dysfunctional side
Inferior on dysfunctional side
Short Muscles
Rectus femoris, iliopsoas
Hamstrings, glutes
Anterior Rotation Pattern
ASIS low (inferior), PSIS high (superior) on affected side
Ipsilateral leg appears longer at the medial malleolus
Pubic tubercle sits inferior, ischial tuberosity sits superior on that side
Hip flexors (iliopsoas, rectus femoris) are hypertonic and shortened
Common in runners, cyclists, and people who sit with one leg extended
Posterior Rotation Pattern
ASIS high (superior), PSIS low (inferior) on affected side
Ipsilateral leg appears shorter at the medial malleolus
Pubic tubercle sits superior, ischial tuberosity sits inferior on that side
Hamstrings and gluteal muscles are hypertonic and shortened
Common after heavy hamstring loading (deadlifts, hill running)
💡Leg length clue: The medial malleolus moves with the rotation. Anterior rotation tips the bone forward, pushing the acetabulum inferiorly and making the leg appear longer. Posterior rotation tips the bone backward, pulling the acetabulum superiorly and making the leg appear shorter. Always compare medial malleoli with the patient supine and legs extended.
⚠️
Board Trap: Pubic Tubercle Direction
Do not confuse the pubic tubercle position in a rotation with a "pubic shear" (which is a separate dysfunction; see the shears page). With anterior innominate rotation the bone tips forward, so the pubic tubercle drops inferior on the dysfunctional side and the ischial tuberosity rides superior. With posterior rotation the directions flip: pubic tubercle superior, ischial tuberosity inferior. Memory: anything in front of the hip axis (ASIS, pubic tubercle) follows the ASIS up or down, and anything behind it (PSIS, ischial tuberosity) follows the PSIS the opposite way.
THE LINEUP
Innominate Dysfunctions
Six clinical entities. Each card front: the dysfunction name and the single landmark that gives it away. Flip for the full landmark pattern, leg length change, and treatment direction.
Dysfunction #1
Anterior Innominate Rotation
ASIS drops inferior. Bone tips forward around the transverse axis.
Tap to see the full pattern →
Landmark pattern:
ASIS: inferior (low) on affected side
PSIS: superior (high) on affected side
Pubic tubercle: inferior on affected side
Ischial tuberosity: superior on affected side
Leg length: appears longer (acetabulum tips down)
Tx: hip extension, MET or HVLA to close anterior rotation
Dysfunction #2
Posterior Innominate Rotation
ASIS rises superior. Bone tips backward. Hamstrings and gluteals are shortened.
Tap to see the full pattern →
Landmark pattern:
ASIS: superior (high) on affected side
PSIS: inferior (low) on affected side
Pubic tubercle: superior on affected side
Ischial tuberosity: inferior on affected side
Leg length: appears shorter (acetabulum rides up)
Tx: hip flexion stretch, MET targeting hamstrings
Dysfunction #3
ASIn Left on Left Oblique Axis
Left innominate rotates anterior on the left oblique axis. A sacral shear variant.
Tap for axis and axis rule →
Key concepts:
Axis: left oblique axis (L5-S1 left ILA pivot)
Left ASIS: inferior, left PSIS: superior
Sacrum: may show anterior sacral base on left
Rule: innominate names its own side rotation first
Tx: correct the sacral component first, then address innominate
Dysfunction #4
PSIn Right on Right Oblique Axis
Right innominate rotates posterior on the right oblique axis.
Tap for axis and landmarks →
Key concepts:
Axis: right oblique axis (L5-S1 right ILA pivot)
Right ASIS: superior, right PSIS: inferior
Leg: right appears shorter
Common cause: heavy hamstring loading on right side
Tx: hip flexion MET, address sacral dysfunction if present
Landmark #5
ASIS vs PSIS: The Seesaw Rule
ASIS and PSIS move in OPPOSITE directions. Lock this in before clinical medicine day.
Tap to drill the rule →
Seesaw pattern (anterior rotation):
ASIS goes DOWN (inferior)
PSIS goes UP (superior)
Pubic tubercle DOWN, ischial tuberosity UP
Posterior rotation: reverse every direction above.
Memory: front of pelvis (ASIS, pubic) follows same direction; back (PSIS, ischial) flips
Concept #6
Normal Innominate Motion
With walking, the innominate rotates anterior during hip extension and posterior during hip flexion.
Tap for the gait pattern →
Normal gait cycle:
Heel strike: innominate rotates posterior
Toe off: innominate rotates anterior
Axis: transverse axis through the pubic symphysis
Clinical pearl: dysfunction = innominate stuck in one position; restricted motion is the key finding
Test with ASIS, PSIS, and medial malleolus comparison supine
PROVE IT
Clinical Questions
Five patients. Five traps. Let's see if the seesaw model sticks.
Medically reviewed by Fatima Ali, DO and Kaitlyn Cocuzzo, MD · Last updated July 1, 2026 at 10:03 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.