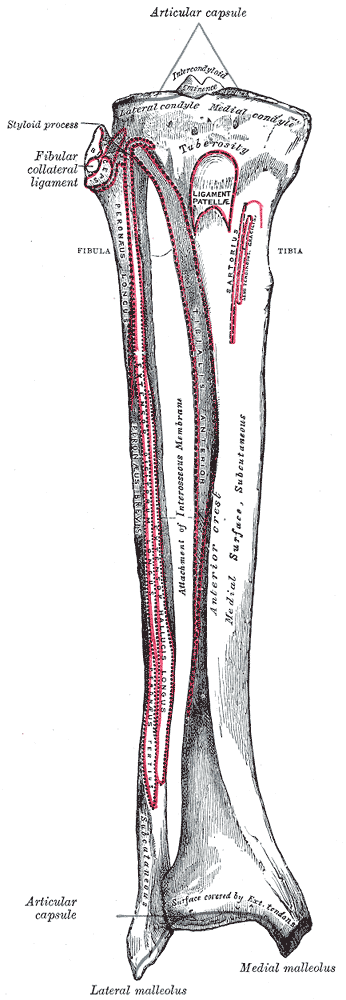
This is the one concept that makes everything else click. The fibula is a seesaw · the interosseous membraneA tough fibrous sheet connecting the tibia and fibula along their entire length. It's the fulcrum of the seesaw · when one end of the fibula moves, the membrane forces the other end to move oppositely. is the fulcrum.
When the proximal fibular head goes anterior, the distal end (lateral malleolus) goes posterior. And vice versa. Always. No exceptions. 🔑Seesaw = See the opposite. Top goes left? Bottom goes right. Always.
PIP = Posterior fibular head = Inversion + Plantarflexion (supination ease)
DEA = (D)orsiflexion + (E)version + (A)bduction = anterior fibular head (pronation ease) 🔑PIP = Posterior = Inversion + Plantarflexion. DEA = Dorsiflexion + Eversion + Abduction = Anterior. The ease tells you the name.
clinical medicine loves asking "which motions make up supination?" This is a three-part combo for each. Think of it as a martial arts stance.
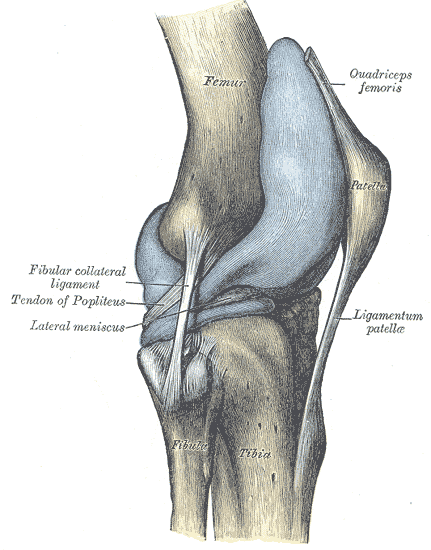
The diagnosis is about palpation comparison. You're checking the proximal tibiofibular jointThe joint where the fibular head articulates with the lateral tibial condyle. It's a synovial plane joint with slight gliding motion. Feel it just below and lateral to the tibial plateau. and comparing both sides.
Both anterior and posterior fibular head dysfunctions use muscle energy techniqueA direct technique where you position the patient at the restrictive barrier, have them push against you (isometric contraction for 3-5 seconds), then take up the new slack. Repeat 3-5 times. The patient does the work · you just hold position and move further into the barrier after each contraction. (MET). It's a direct technique · you push toward the barrier, not away from it.
1. Wrap hands around proximal fibula
2. Push fibular head posteriorly
3. Patient dorsiflexes + everts foot against your resistance (activates peroneal muscles which pull fibula posterior)
4. Hold 3-5 sec → relax → take up slack
5. Repeat 3-5 times
1. Wrap hands around proximal fibula
2. Push fibular head anteriorly
3. Patient plantarflexes + inverts foot against your resistance (activates muscles that pull fibula anterior)
4. Hold 3-5 sec → relax → take up slack
5. Repeat 3-5 times
Tap each card. Front = the concept. Back = the board-tested detail.
Proximal: Fibular head sits anterior + lateral
Distal: Lateral malleolus swings posterior + medial
Foot: Pronation (abd + ev + DF) · DEA
Treat with: Direct MET, push posterior. Patient does dorsiflexion + eversion.
Proximal: Fibular head sits posterior + medial
Distal: Lateral malleolus swings anterior + lateral
Foot: Supination (add + inv + PF) · PIP
Treat with: Direct MET, push anterior. Patient does plantarflexion + inversion.
TART: Tissue texture change, Asymmetry, Restriction of motion, Tenderness
Key palpation: compare fibular heads bilaterally. The dysfunctional side is more prominent in the direction of displacement. Check the lateral malleolus to confirm seesaw.
HVLA: High velocity low amplitude thrust. Direct technique. Fast thrust toward the restrictive barrier. Contraindicated if hypermobility, fracture, or osteoporosis present.
clinical medicine almost always test MET for fibular head.
Scroll to see anatomy and clinical context. Tap to enlarge.