OA, AA, and C2-C7 , naming, diagnosing, and treating cervical somatic dysfunction
Opening Challenge
A 35-year-old woman presents with neck pain after a rear-end collision. Osteopathic examination finds that at the occipitoatlantal (OA) joint, the right occiput is posterior and inferior. Tissue texture changes are present on the right. She has restricted right sidebending and right rotation. What is the correct notation for this dysfunction?
A) OA ERS right
B) OA FRS right
C) OA NS right
D) OA ERS left
OA ERS right. OA is a Type II (non-neutral) joint that obeys Fryette's Law II. The right occiput is posterior, meaning the joint has moved into extension (backward-bent) on that side. Extended position + right sidebending + right rotation = ERS right. The dysfunction is named for the position it IS stuck in, not where it cannot go. For HVLA: flex the head, then sidebend and rotate LEFT (toward the restrictive barrier) and thrust. MET is an alternative if HVLA is contraindicated. Common traps: FRS right would mean the occiput is ANTERIOR (flexed), which is the opposite of what the vignette says. NS right would mean no flexion-extension restriction at all. ERS LEFT means the restriction is on the left side, but the vignette clearly places the posterior occiput and the tissue changes on the right. Think of ERS notation as a parking ticket: it describes where the car is illegally parked (the malposition), not where you want it to go. The right occiput is parked in extension, right-tilted, right-rotated. Break it down: OA follows Law II always (ERS or FRS, never NS); ERS = stuck extended, sidebent and rotated in the same direction; the letter after ERS is the side of the restriction, matching the side of the posterior occiput.
01 · The Framework
Cervical Anatomy & Naming
Three distinct joints. Each with its own motion rules. Get this wrong and the notation falls apart.
Occipitoatlantal (OA) Joint
The OA joint sits between the occiput and C1 (atlas). The atlas has no spinous process and no vertebral body. It is a ring of bone with lateral masses on each side.
Primary motion: flexion and extension (nodding). Think: the skull nods forward and backward on the ring of C1.
Fryette's Law: Type II applies here. Non-neutral mechanics. Sidebending and rotation occur to the SAME side. So if the segment is extended, sidebent right, and rotated right, that is one coherent dysfunction.
Notation:
OA ERS right = extended, rotated right, sidebent right.
OA FRS right = flexed, rotated right, sidebent right.
Named for the position the joint IS stuck in (the free side).
HVLA for OA ERS right: flex the head (off the extension), sidebend and rotate LEFT (toward the barrier), thrust. The rule: move toward the restrictive barrier, not away from it.
Alternative: MET (muscle energy technique) if HVLA is contraindicated or the patient prefers gentler treatment.
Type II FryetteNod joint (flex/ext)ERS or FRSHVLA toward barrier
Atlantoaxial (AA) Joint
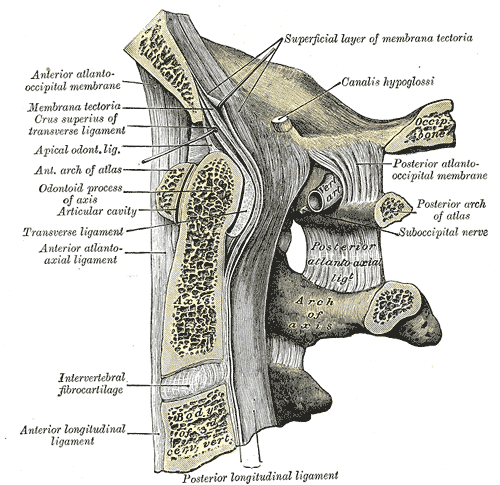
The AA joint sits between C1 (atlas) and C2 (axis). C2 has a dens (odontoid process) that projects superiorly into the ring of C1, held in place by the transverse atlantal ligament.
Primary motion: ROTATION. The AA joint provides roughly 50% of total cervical rotation. Nodding occurred at OA. Rotation lives at AA.
Dysfunction notation: AA rotated right means the segment IS rotated right and rotation to the right is the free motion. Rotation back to the left is restricted (that is the barrier).
Absolute contraindications to HVLA at AA:
1. Rheumatoid arthritis with odontoid erosion (pannus erodes the dens, destroying the pivot; thrust risks spinal cord compression).
2. Down syndrome (ligamentous laxity at the transverse atlantal ligament; atlantoaxial instability is a known complication).
Use MET or counterstrain as the safe alternative in these populations.
50% of cervical rotationRA = HVLA contraindicatedDown syndrome = HVLA contraindicatedDens projects into C1 ring
C2-C7 (Typical Cervical)
C2-C3 is transitional: C2 has a bifid spinous process and acts as a bridge between the atypical upper cervical region and the typical lower cervical segment. C3-C7 are the true typical cervical vertebrae.
Motion: All three planes (flexion/extension, sidebending, rotation). Fryette's Laws apply.
Type I (neutral, group) dysfunction: Multiple segments involved. Sidebending and rotation occur to OPPOSITE sides. Example: C3-C5 group dysfunction with sidebending right and rotation left.
Type II (non-neutral, single segment) dysfunction: One segment. Sidebending and rotation to the SAME side. Named for the extended or flexed position + side.
Key diagnosis rule: The spinous process deviates AWAY from the direction of rotation. If the spinous process points right, the vertebra is rotated LEFT. This is because the spinous is on the posterior side; rotation of the body to the left sends the spinous to the right.
All 3 planesType I = group, oppositeType II = single, same sideSpinous deviates OPPOSITE to rotation
Board anchor: OA = nod joint (flexion/extension). AA = rotation joint (50% of cervical rotation). C3-C7 = standard Fryette's rules apply. OA and AA are atypical with special motion rules. Know which joint you are at before you name the dysfunction.
02 · How to Find It
Diagnosis Techniques
Tap each card to reveal the technique. These are the clinical tools you use to find somatic dysfunction at the cervical spine.
Motion Testing▼
Tap to reveal
Active ROM first: the patient moves their own head. Watch for restrictions, pain, deviation. This tells you where to look more carefully.
Passive ROM: the examiner moves the head and feels for resistance, end-feel, and tissue changes at each segment.
Spring testing (segmental): the examiner applies an anterior-posterior pressure to the spinous process or transverse process. A normal segment springs back. A dysfunctional segment feels stiff or "blocked."
Naming rule: the segment is named for where it went (the position it IS stuck in), not where it cannot go. Restricted motion to the right means it is stuck in left sidebending, and the dysfunction is named FRS left or ERS left depending on flex/extension status.
Active then passiveSpring test = segmentalNamed for free side (where it IS)
TART Criteria▼
Tap to reveal
The four diagnostic criteria for somatic dysfunction. All four should be present:
T = Tissue texture changes. Acute: warm, edematous, boggy, doughy. Chronic: cool, fibrotic, ropy, stringy. This is the most reliable finding.
A = Asymmetry. Structural position of the segment is asymmetric compared to adjacent segments. Identified by palpation of the transverse processes and spinous process.
R = Range of motion restriction. The segment does not move freely in all planes. The restriction defines the barrier.
T = Tenderness. Local tenderness on palpation of the affected segment and surrounding musculature.
You can also use the mnemonic in reverse: STAR (Structural asymmetry, Tissue texture changes, Asymmetry, Range of motion, Tenderness).
Tissue textureAsymmetryROM restrictionTenderness
Cervical Treatment Techniques▼
Tap to reveal
HVLA (High Velocity Low Amplitude): the thrust technique. Patient supine, operator at head of table. Operator introduces the three motion components of the dysfunction (e.g., OA ERS right: flex head, left sidebend, left rotate), then delivers a rapid low-amplitude thrust at the restrictive barrier. The audible pop is cavitation of the joint, not cracking bone.
MET (Muscle Energy Technique): active technique using the patient's own muscles. Operator brings the segment to the restrictive barrier. Patient isometrically contracts against operator's unyielding resistance for 3-5 seconds. Patient relaxes completely. Operator takes up the new (improved) barrier. Repeat for 3-5 cycles. Works via post-isometric relaxation and reciprocal inhibition.
Counterstrain: indirect technique. Examiner finds the tender point. Positions the patient away from the tender point into a position of ease (the body's preferred shortened position) for 90 seconds. Returns slowly to neutral. Tender point should resolve by at least 70%.
Absolute HVLA contraindications (cervical): Rheumatoid arthritis (upper cervical), Down syndrome, severe osteoporosis, acute fracture, vertebrobasilar insufficiency, known metastatic disease to the spine, anticoagulation with INR above therapeutic range. When in doubt, use MET or counterstrain.
03 · Clinical Patterns
Special Cervical Syndromes
Three conditions where cervical somatic dysfunction shows up as something that looks like a different diagnosis entirely.
Cervicogenic Headache▼
Tap to reveal
Somatic dysfunction at OA, AA, or C2-C3 refers pain to the occiput, temporal region, or retro-orbital area via the suboccipital and upper cervical nerves.
Distinguishing features from migraine: unilateral, non-throbbing quality, no aura, no nausea or photophobia, directly aggravated by neck movement or sustained neck posture, and reproducibly relieved by cervical OMT.
Diagnostic test: cervical flexion-rotation test. Patient fully flexes the neck (chin to chest), then the examiner passively rotates the head left and right. Restricted rotation with the neck fully flexed points to upper cervical (OA-C2) as the source. Normal rotation should be about 44 degrees each direction. Less than 32 degrees is positive for upper cervical involvement.
OMT target: OA dysfunction is the most common culprit. C2-C3 dysfunction also common, especially after whiplash.
OA/AA/C2-C3 somatic dysfunctionNo aura, no nauseaRelieved by cervical OMTFlexion-rotation test positive
Torticollis (Wry Neck)▼
Tap to reveal
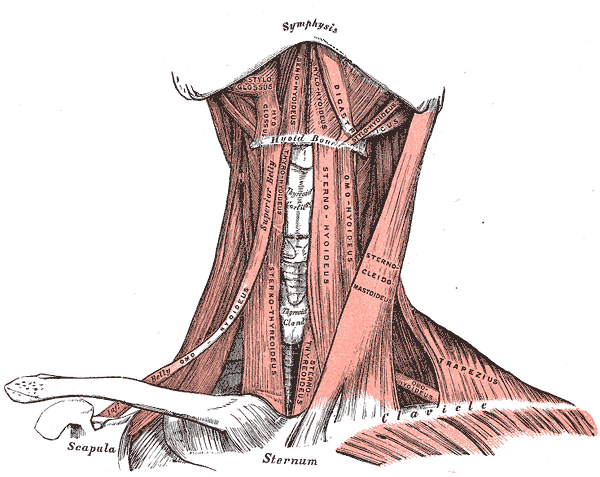
Acute torticollis is spasm of the sternocleidomastoid (SCM) pulling the head into a fixed position. The SCM runs from the mastoid process (behind the ear) to the sternum and clavicle on the opposite side.
Positional anatomy of SCM spasm: The shortened SCM pulls the head rotated to the OPPOSITE side and laterally flexed (sidebent) to the IPSILATERAL side. Right SCM spasm = head rotates left and tilts right. This is opposite to what you might guess.
OMT approach:
Acute phase: gentle MET to the SCM. Do NOT thrust into an acute spasm. Spray-and-stretch (vapocoolant spray over the SCM, then gentle passive stretch) is effective for acute presentations.
Subacute/chronic: once the acute spasm resolves, HVLA to address the underlying segmental dysfunction at C1-C3 is appropriate.
Congenital torticollis (in infants) is due to fibrosis of the SCM from birth injury. Distinguish from acute acquired torticollis.
SCM spasmRotates to opposite side of spasmTilts to same side as spasmMET first, not HVLA in acute
Chapman Points (Cervical)▼
Tap to reveal
Chapman reflex points represent viscerosomatic reflexes. Visceral dysfunction creates palpable nodular tissue changes at specific anterior and posterior locations.
Sinus-related Chapman points:
Anterior: between ribs 1 and 2 on the anterior chest wall (for sinusitis).
Posterior: in the upper cervical region near OA-C2, often palpable as small, firm, tender nodules.
Clinical pattern: Recurrent sinusitis with persistent posterior upper cervical somatic dysfunction may have a viscerosomatic component. Treating the cervical Chapman points (firm circular pressure for 30 seconds) along with OMT of the upper cervical region can reduce the frequency of sinus infections by improving lymphatic drainage and normalizing autonomic tone.
Board point: Chapman points are NOT traditional tender points. They are palpable ganglionic condensations in the fascia. Anterior points are diagnostic; posterior points can be treated.
Use the clues to eliminate wrong answers one by one. Only the correct notation survives.
A 45-year-old physician undergoes a routine osteopathic structural exam. The examiner finds the right occiput posterior. There are tissue texture changes on the right side of the upper cervical region. Motion testing shows the segment moves freely into left sidebending and left rotation, but is restricted in right sidebending and right rotation. What is the most appropriate notation for this dysfunction?
OA FRS right
OA ERS right
OA NS right
OA ERS left
Clue 1: The right occiput is posterior. Posterior occiput means the occiput has moved backward, which is extension. If the joint were flexed (FRS), the occiput would be anterior. NS (neutral/group) does not apply to OA because OA is a Type II joint and cannot have neutral dysfunction. This eliminates OA FRS right and OA NS right.
Clue 2: The segment moves freely into left sidebend and left rotation, and is restricted right. The dysfunction is named for where the segment IS (the free side), not where it cannot go. Free motion is to the left. So the segment is stuck in right sidebending and right rotation. ERS right = extended, rotated right, sidebent right. ERS left would mean free motion to the right, which is the opposite of what we see here. This eliminates OA ERS left.
OA ERS right. Extended (posterior occiput), rotated right, sidebent right. The free motion is to the left, confirming the segment is stuck on the right. HVLA treatment: flex the head off the extension, sidebend and rotate left toward the barrier, thrust. MET: introduce the same components, patient isometrically resists, repeat 3-5 cycles.
05 · Retrieval Practice
Quiz
Four board-style questions. Original vignettes. Lock in your answer before reading the explanation.
Question 1 of 4
A 55-year-old woman with rheumatoid arthritis presents for a routine exam. Osteopathic structural examination identifies restricted rotation at the C1-C2 level. The segment is rotated right with restricted return to the left. Which motion is primarily restricted at this joint, and which treatment approach is MOST appropriate for this patient?
Which answer correctly identifies both the restricted motion AND the safest treatment?
AFlexion restricted; HVLA is appropriate and well-tolerated
BRotation restricted; HVLA is the first-line treatment
CRotation restricted; HVLA is absolutely contraindicated, use MET
DSidebending restricted; counterstrain is appropriate, HVLA contraindicated
Tempting to pick HVLA since it is the standard first-line technique for AA rotation dysfunctions in a healthy patient, but rheumatoid arthritis changes the calculus completely. Think of the dens as a door stopper that keeps C1 from sliding backward into the spinal cord: RA pannus erodes the stopper, and HVLA with no stopper means the door can swing all the way into the cord. Correct: C.
The AA (atlantoaxial, C1-C2) joint provides approximately 50% of total cervical rotation. Its primary motion is rotation, not flexion or sidebending. When a rotational dysfunction is present at AA, HVLA is the treatment of choice in a healthy patient. However, in rheumatoid arthritis, pannus formation can erode the odontoid process (dens) of C2. The dens is what stabilizes C1 from translating forward on C2. Without an intact dens, HVLA at the AA joint risks driving C1 posteriorly into the spinal cord. HVLA is absolutely contraindicated. MET (muscle energy technique) or counterstrain are safe alternatives.
Choices A and D: Flexion is OA's primary motion, not AA. Sidebending is not AA's primary motion. Both eliminate these as the primary restricted motion. Choice B is tempting because HVLA is often the first-line treatment for AA rotation dysfunctions in a healthy patient. The critical detail is rheumatoid arthritis: pannus erodes the dens, removing the structural stop that prevents C1 from sliding back into the cord. Think of the dens as a door stopper: without it, the door (C1) can swing all the way back and crush what is behind it. RA removes the stopper. HVLA with a missing stopper = potential cord injury. Break it down: AA is the primary rotation joint (50% of cervical rotation); HVLA is contraindicated at AA when RA has destroyed the dens; MET or counterstrain are safe alternatives when dens integrity is uncertain.
Question 2 of 4
During a practical skills exam, a student identifies a cervical somatic dysfunction. The examiner asks: "What do the four letters in TART stand for?" The student begins: "T is tissue texture changes, A is asymmetry, R is range of motion restriction..."
What does the final T in TART stand for?
ATightness of the surrounding musculature
BTemperature change at the skin surface
CTenderness on palpation
DTone of the paraspinal musculature
Tempting to pick temperature change since it is the most concrete measurable finding in tissue assessment and sounds like a standalone criterion, but temperature is filed under the first T (tissue texture changes), not as a fourth T. Think of TART as four labeled drawers in a filing cabinet: temperature, tightness, and tone all get filed in the T1 drawer; only tenderness gets its own drawer at position T4. Correct: C.
TART = Tissue texture changes, Asymmetry, Range of motion restriction, Tenderness. All four criteria must be present for somatic dysfunction to be diagnosed. Tenderness is elicited by palpating the affected segment and surrounding soft tissues.
Traps: Temperature change is sometimes discussed as part of tissue texture assessment (acute = warm, chronic = cool), but it is included under the first T (tissue texture changes), not a separate criterion. Tightness and tone are also components of tissue texture, not a standalone TART criterion. Think of TART as four drawers in a filing cabinet: temperature, tightness, and tone all get filed in the tissue-texture drawer. Only tenderness gets its own drawer at the end. Common trap: choosing temperature because it sounds distinctive and measurable. It is real but it belongs to the T1 drawer, not a new T4 category. Break it down: TART = Tissue texture changes (T1) + Asymmetry + Range of motion restriction + Tenderness (T4); temperature, tightness, and tone are all filed under T1 (tissue texture), not as a separate criterion.
Question 3 of 4
An osteopathic physician is treating a 42-year-old man with C5 ERSR dysfunction using muscle energy technique. The physician positions the segment at the restrictive barrier and instructs the patient to gently push back against the physician's hand.
How long should the patient hold the isometric contraction, and how many cycles should be performed for maximum effectiveness?
A10 seconds per contraction, 1-2 cycles
B3-5 seconds per contraction, 3-5 cycles
C3-5 seconds per contraction, 1 cycle is sufficient
D90 seconds of sustained contraction, then release
Tempting to pick 10-second contractions since longer effort seems more thorough for working against a restriction, but post-isometric relaxation happens in the brief window immediately after effort stops, and shorter cycles stacked 3-5 times accumulate more gain than one long effort. Think of MET like gaining ground on a slippery slope: one short push loosens the footing just a little, and three to five pushes stack those small gains before the footing resets. Correct: B.
MET protocol: 3-5 second isometric contraction, then full relaxation. The operator takes up the new barrier (which should have moved because of post-isometric relaxation). Repeat 3-5 cycles. Each cycle slightly increases the available range of motion as the muscle spindle resets.
Mechanism: Post-isometric relaxation causes the Golgi tendon organ to inhibit the contracted muscle after effort. The muscle spindle resets to a longer length. Reciprocal inhibition also relaxes antagonist muscles. Three to five repetitions compounds the gain.
Choice D (90 seconds): That is the counterstrain hold time. Counterstrain holds the patient in a position of ease for 90 seconds, then slowly returns to neutral. It is an entirely different technique with a different mechanism. Choice A (10 seconds, 1-2 cycles) is tempting because longer and fewer seems more thorough. Choice C (1 cycle) underestimates how PIR compounds. Think of gaining ground on a slippery slope: one isometric effort loosens the grip just a little. Three to five reps stack those small gains before the muscle tone fully resets. A single long effort (10s) fatigues but does not compound; one cycle does not stack. Break it down: MET = 3-5 second isometric contraction + 3-5 repetitions; each rep uses post-isometric relaxation to advance the barrier slightly; 90 seconds is counterstrain, not MET.
Question 4 of 4
On structural exam of the thoracic spine, the examiner notes that the spinous process of T6 deviates to the right relative to adjacent vertebrae. The examiner confirms this is a fixed structural finding, not an artifact of positioning.
In which direction is the T6 vertebral body rotated?
ATo the right, because the spinous process follows the body
BTo the right, because spinous deviation predicts ipsilateral rotation
CTo the left, because the spinous process deviates opposite to the direction of rotation
DCannot be determined from spinous position alone
Tempting to pick "to the right" since intuition says the spinous process should point in the same direction the vertebra turned, but the spinous is a posterior projection that swings the opposite way. Think of a steering wheel: turning the wheel left makes the top of the wheel go right. The spinous is that tail. Correct: C.
The spinous process is a posterior projection. When the vertebral body rotates to the LEFT, the posterior elements (including the spinous) swing to the RIGHT. Think of it like a steering wheel: turning the wheel to the left makes the top of the wheel go to the right relative to a fixed reference point.
This is one of the most commonly tested rules in OMM: spinous process deviates OPPOSITE to the direction of vertebral body rotation. Spinous goes right = body rotated left.
This applies to the cervical spine as well as the thoracic and lumbar regions. On boards, if they give you spinous deviation, flip it to get the rotation direction. Common trap: choosing "to the right" because intuition says the spinous should point the same way the body turned. The spinous projects POSTERIORLY. When the body rotates left, the front swings left but the tail (spinous) swings right, just like the steering wheel top going right when you turn left. Choices A and B both say right, and are both wrong for different stated reasons, but both share the same misunderstanding about the anatomy. Choice D is a distracter that is designed to make you second-guess a deterministic rule. The spinous position is always a reliable indicator of rotation direction. Break it down: spinous process ALWAYS deviates opposite to vertebral body rotation direction; spinous right = body rotated left; this rule applies universally from cervical to lumbar spine.
0/4
quiz complete
OA joint: occiput on C1 atlas
AA joint: C1 atlas and C2 axis dens
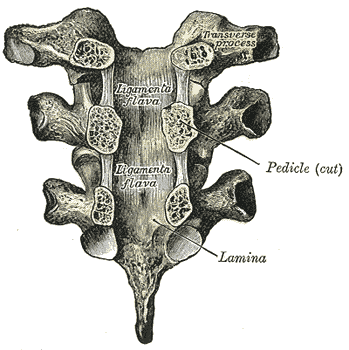
Typical cervical vertebra C3-C7
Ligamenta flava between the laminae (posterior view)
SCM muscle: mastoid to sternum/clavicle
Board Practice
Board-Style Walkthrough
Five original board-style vignettes. Shuffle and never repeat until bank is exhausted.
A patient has OA dysfunction with the right occiput posterior. What is the correct ERS notation and which motion is RESTRICTED?
OA ERS right; restricted in left sidebend and left rotation
OA FRS right; restricted in extension
OA NS right; restricted in rotation only
Correct. Posterior occiput = extended. OA ERS right = extended, sidebent right, rotated right. The free side (where it IS) is right. The restriction is to the left: left sidebend and left rotation are blocked. HVLA: flex the head off extension, introduce left SB and left rotation, thrust.
FRS right means the occiput is anterior (flexed), not posterior. A posterior occiput has moved into extension. The first letter must match the actual position.
NS (neutral/group) notation does not apply to the OA joint. OA is a Type II joint and always follows ERS or FRS notation. The OA cannot be in a neutral group dysfunction.
The same patient has RA. You confirm atlantoaxial instability. Can you perform HVLA at OA?
Yes, HVLA at OA is safe as long as you avoid AA
No, RA with upper cervical instability is an absolute contraindication to HVLA throughout the upper cervical region
RA with atlantoaxial instability is an absolute contraindication to HVLA anywhere in the upper cervical region. The OA and AA joints are biomechanically linked; thrusting at OA can transmit forces to the unstable AA joint.
Correct. RA-related atlantoaxial instability is an absolute contraindication to upper cervical HVLA including OA. Use MET or counterstrain as the safe alternative.
Walk the chain: Patient has OA ERS right. What is the step-by-step HVLA treatment?
1
What does ERS right tell you about where the segment is stuck?
Tap to reveal
2
What motion must you introduce first to "unlock" the extended position?
Tap to reveal
3
After flexion, which direction do you sidebend and rotate toward for HVLA?
Tap to reveal
4
What is the MET alternative if HVLA is contraindicated?
Tap to reveal
ERS right = stuck in extension, SB right, rot right. Fix it by going opposite: flex first, then SB left and rotate left toward the barrier, thrust. MET: same setup, patient pushes right against resistance, relax, advance left. Three to five cycles.
Memory Hook
How do I remember that ERS right means the RIGHT occiput is posterior?
ERS right = the segment went Extended, Sidebent right, Rotated right. Think of it as the "crime scene label": you are naming where the bone PARKED itself illegally. Right occiput parked posterior = Extended. The name says where it IS, not where it needs to go.
Memory Hook
How do I remember AA gives 50% of cervical rotation?
OA = NODDING (flexion/extension). AA = ROTATING. Saying "No" = OA. Saying "I don't know" (side to side shake) = AA. The AA dens is the pivot pin for 50% of total cervical rotation. Without the dens, there is no pivot and no rotation.
Memory Hook
Why is RA an absolute contraindication at AA but not at C5?
RA erodes the dens via pannus. The dens is the stopper that keeps C1 from sliding back into the spinal cord. Without the stopper, HVLA = C1 slides back = cord compression. At C5, RA can cause disc and facet changes but there is no single structural stopper whose failure leads directly to cord injury.