Stop memorizing fundus photos as separate trivia. The board move is smaller: where is the vision lost, what does the fundus show, and does the retina need help today?
PeripheralNight and side vision point to rods and retinitis pigmentosa.
CentralMetamorphopsia and central scotoma point to the macula.
EmergencyCurtain, cherry-red spot, papilledema, or rapid wet AMD changes the pace.
Rods burn out first: night and peripheral field shrink.Cones pack the fovea: central detail and color.Disc swelling means pressure is backing into CN II.
Pick the cannot-wait case
Four patients call about vision loss. Which one gets same-day emergency eye evaluation?
Yes. Flashes plus floaters plus a curtain is retinal tear or detachment until proven otherwise. The retina has separated from choroid support, so photoreceptors are ischemic and the clock matters.
Screen 1
Put the complaint on the retina before naming the disease.
Central vision, peripheral vision, the optic disc, and the vessel tree each produce a different board flavor. Tap a region, then read the pattern it creates.
Macula and fovea
The macula is the central high-resolution zone. The fovea is packed with cones, so disease here gives central scotoma, distorted straight lines, and loss of color/detail.
Memory lockMacula equals middle of the movie screen. Peripheral retina can still see the theater wall.
ActionSeparate dry, slow drusen from wet, rapid neovascular leakage.
CurtainRetina peeling away from choroid support.
Cherry redInner retina ischemic, fovea still choroid-red.
Blood thunderVein blocked, blood backs up everywhere.
Disc blurICP transmits down optic nerve sheath.
Screen 2
Fundus pattern lab: match the picture to the mechanism.
Each disease gets one visual signature and one pathophysiology chain. The goal is not a photo museum. The goal is seeing a fundus clue and knowing what process made it.
Inherited rod loss
Retinitis pigmentosa
PatientChildhood onset night blindness and shrinking peripheral fields.
FundusBone-spicule pigmentation where photoreceptors disappeared.
WhyRods are hit early, so dark adaptation and side vision go first.
If the board says legal blindness by middle age plus tunnel vision, think inherited photoreceptor death, not a vascular event.
Clinical image strip
Tap any image to enlarge. Photos are used as whole-image pattern anchors; the page does not place guessed markers on real fundus photos.
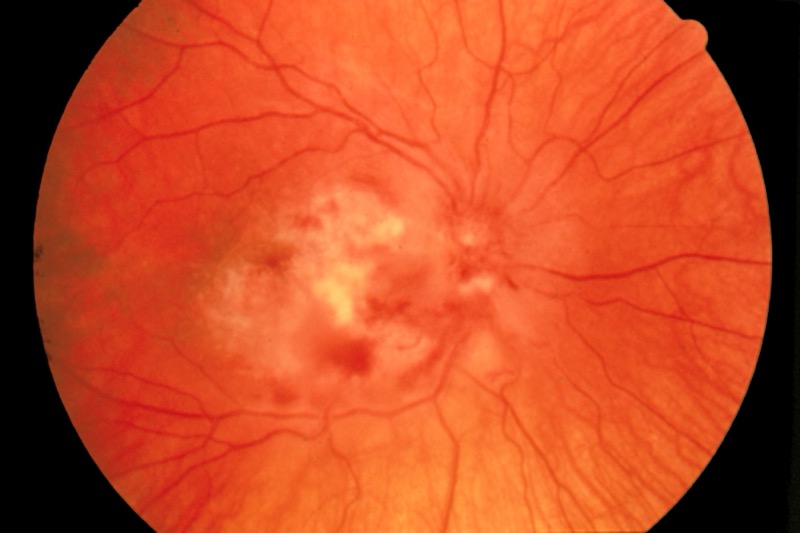
CMV retinitisWhitish retinal necrosis with hemorrhage in a severe immunosuppression pattern.Proliferative diabetic retinopathyIschemia drives fragile new surface vessels that can bleed or pull retina.PapilledemaSwollen optic disc margins from raised intracranial pressure.Retinal detachmentA whole-retina emergency pattern: flashes, floaters, then curtain.
Retinal disease is a triage topic. The board stem usually tells you whether the problem is slow degeneration, blocked flow, pressure, or a retina separating from its blood supply.
Flashes, floaters, curtain
Think posterior vitreous traction causing a retinal tear or detachment. Once the retina peels away from the choroid, photoreceptors lose metabolic support. That is why a curtain complaint is not watchful waiting.
TriggerMyopia, trauma, prior surgery, or proliferative diabetic retinopathy.
Retina logicVitreous traction tears retina, fluid tracks under it, choroid support is lost.
Exam actionUrgent ophthalmology. Treat as a surgical emergency.
Macula membrane model
Dry AMD is debris, slow vision loss.
Dry disease is more common. Drusen accumulate between retinal pigment epithelium and Bruch membrane, so central vision fades gradually. Vitamins and antioxidant supplements can slow risk in selected patients, but there is no acute vessel leak to seal.
Screen 4
Board walkthrough: make the fundus clue do the work.
One vignette at a time. Right-click or long-press to cross out. Double-click or double-tap to highlight. The bank shuffles answers and will not repeat until you have seen all 29.
Vignette 1 of 29
Progress 0/29
Teaching chain
Next useful reps
Retina pages connect cleanly to visual fields, lens/refraction, and intracranial pressure. Keep the eye complaint mapped to the structure before you chase disease names.