MG vs LEMS vs Botulism. The board's favorite "which direction does the weakness go?" question. Let's make sure you never mix them up again.
LEMS in cancer: Small cell lung paraneoplastic ›
Every NMJ disorder attacks a different part of the same synapse. Once you know WHERE the problem is, the clinical picture writes itself.
Action potential arrives at nerve terminal → VGCCsVoltage-Gated Calcium Channels. When the action potential depolarizes the nerve terminal, these channels open and let calcium flood in. Calcium is the signal that tells vesicles to fuse with the membrane and dump ACh into the cleft. No calcium entry = no ACh release. open → Ca2+ floods in → AChAcetylcholine. The neurotransmitter at the NMJ. Synthesized from choline + acetyl-CoA by choline acetyltransferase. Released in quanta (packets) from vesicles. Degraded by acetylcholinesterase in the cleft. Every step here is a potential drug target. vesicles fuse and release → ACh crosses the cleft → binds AChRsNicotinic Acetylcholine Receptors. These are ligand-gated ion channels (not muscarinic). When ACh binds, the channel opens, Na+ enters, the muscle depolarizes. In MG, antibodies block or destroy these receptors, fewer receptors = weaker signal = fatigable weakness. on muscle → muscle contracts.
Now break each step and watch what happens.
Anti-AChR antibodiesFound in ~85% of MG patients. These IgG antibodies bind to the nicotinic AChR, causing: (1) complement-mediated destruction of the postsynaptic membrane, (2) accelerated internalization of receptors, (3) direct blocking of ACh binding. Fewer functional receptors = each successive nerve impulse is less effective = fatigue. destroy or block AChRs on the muscle. The nerve releases ACh just fine, but there are fewer receptors to catch it.
First few contractions? Enough receptors still available. But with repeated use, the safety factor drops, each impulse recruits fewer and fewer receptors. The muscle gets weaker and weaker and weaker.
Worsens with repeated use. Better after rest.
Anti-VGCC antibodiesAntibodies against P/Q-type voltage-gated calcium channels on the presynaptic nerve terminal. These channels are what let calcium in to trigger vesicle fusion. Block them = less calcium = less ACh released per impulse. But with repeated stimulation, residual calcium BUILDS UP inside the terminal, eventually enough to trigger release. That's why repeated use HELPS. block calcium channels on the nerve terminal. Less Ca2+ gets in → less ACh gets released.
But here's the twist: with repeated nerve firing, residual calcium accumulates inside the terminal. Eventually enough builds up to trigger vesicle release despite the blocked channels. The muscle starts weak and gets stronger.
Improves with repeated use. The exact opposite of MG. 🔑 LEMS = Less at first, Eventually More Strength
Botulinum toxinClostridium botulinum produces the most potent toxin known. It's a zinc metalloprotease that cleaves SNARE proteins (SNAP-25, synaptobrevin, syntaxin), the machinery that fuses vesicles with the membrane. No fusion = no ACh release = no muscle contraction. Same mechanism as Botox injections (which just use tiny, localized doses). cleaves SNARE proteins, the molecular machinery that fuses ACh vesicles with the membrane. The calcium channels work fine. The receptors work fine. The vesicles just can't release their contents.
Unlike MG or LEMS, this doesn't wax and wane, it's an acute, descending paralysis starting with cranial nerves (eyes, face, swallowing) and spreading downward.
Each disorder is a villain with a signature attack. Tap to flip and read the full playbook.
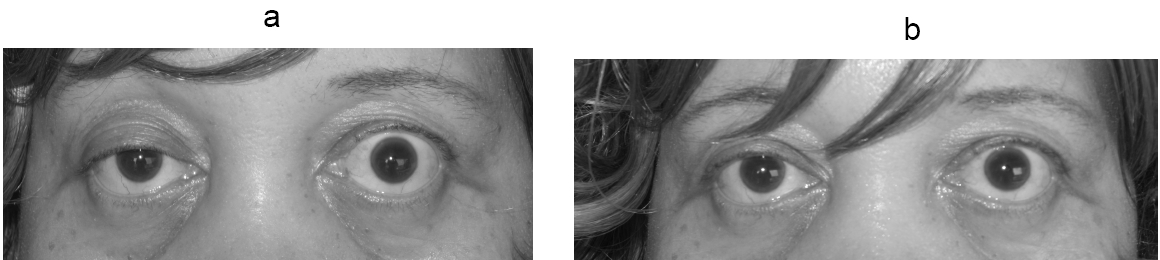
Clinical Images
One table. Three disorders. Every board-tested difference.
| Feature | MG | LEMS | Botulism |
|---|---|---|---|
| Target | Postsynaptic AChR | Presynaptic VGCC | SNARE proteins (presynaptic) |
| Antibody | Anti-AChR (85%) Anti-MuSK (5-8%) |
Anti-VGCC (P/Q-type) | None (toxin-mediated) |
| Repeated use | WORSENS | IMPROVES | No significant change |
| Weakness pattern | Ocular → bulbar → generalized Ptosis, diplopia first |
Proximal legs first "Can't get out of a chair" |
Descending Cranial nerves → trunk → limbs |
| Reflexes | Normal | Decreased (improve after exercise) | Decreased to absent |
| Autonomic | Not typical | Dry mouth, constipation, impotence | Dilated pupils, constipation, urinary retention |
| Cancer link | Thymoma (10-15%) | Small cell lung cancer (50-60%) | None |
| EMG pattern | Decremental response on repetitive stim | Incremental response at high-frequency stim | Decremental; incremental at high freq |
| Treatment | Pyridostigmine, thymectomy, immunosuppression | 3,4-DAP, treat underlying cancer | Antitoxin, supportive care |
| Crisis | Myasthenic crisis (resp failure) → IVIG or plasmapheresis | Rarely crises | Respiratory failure, ICU |
A patient walks in with weakness. You need to figure out if it's the junction. Let's practice the algorithm, you answer BEFORE the tree reveals.
Each clue eliminates one diagnosis. By the end, only the answer remains. Your working memory stays on the screen, not in your head.
PyridostigmineAn acetylcholinesterase inhibitor. It blocks the enzyme that breaks down ACh in the synaptic cleft. More ACh sticks around = more chances to bind to whatever AChRs remain. It treats symptoms but doesn't change the underlying autoimmune process. Side effects are cholinergic: diarrhea, cramping, salivation, bradycardia (think "SLUDGE", Salivation, Lacrimation, Urination, Defecation, GI distress, Emesis). (Mestinon) = first-line.
Blocks acetylcholinesterase → more ACh hangs around in the cleft → better chance of finding a receptor. Treats symptoms, NOT the autoimmune process.
For moderate-severe MG beyond symptom control:
Recommended for:
Respiratory failure from MG = emergency. The diaphragm fatigues.
12 questions in the pool, 5 random per load, shuffled answers. Every visit is different. Let's see if you were paying attention.
Original clinical vignettes. Shuffled, never-repeat, full explanations for every choice.