The metal that hijacks your heme factory, cripples enzymes at two critical steps, and leaves a trail of clues only a sharp clinician will catch.
Opening Case
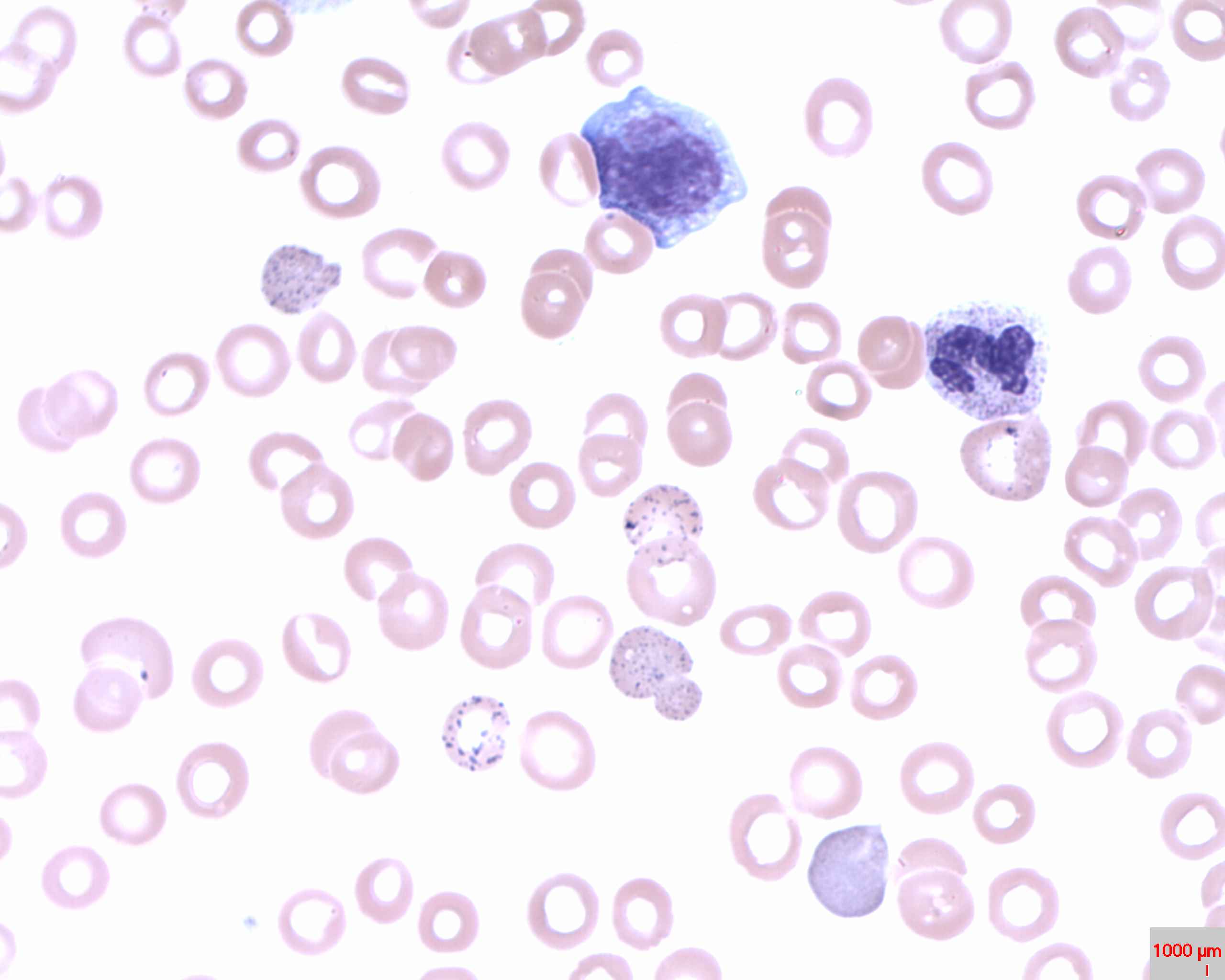
A 4-year-old with pica lives in a pre-1978 apartment. His mother reports irritability and regression in speech. CBC shows microcytic, hypochromic anemia. Serum iron is normal. Peripheral smear shows coarse basophilic stippling. What is the single most important next test?
The clue combo is airtight: microcytic anemia + normal serum iron + basophilic stippling + pica in old housing = lead poisoning until proven otherwise. Ferritin and electrophoresis address iron deficiency and hemoglobinopathies, neither of which causes stippling. FEP is a marker that rises in lead poisoning, but it is not diagnostic on its own and doesn't give you a number to guide chelation decisions. Blood lead level is the diagnostic and treatment-threshold test. Answer: C.
▼ scroll to continue
Why Lead Is Toxic
Two enzyme targets. One collapsed heme factory.
The core mechanism: Lead binds sulfhydryl groups on enzymes. It attacks heme synthesis at two specific steps, causing a traffic jam of precursors upstream and an inability to make functional heme downstream. The result looks like iron deficiency, but iron has nothing to do with it.
🧪
Target 1
ALA Dehydratase
Early in the pathway. Converts ALA → porphobilinogen. Lead blocks it, causing ALA to accumulate. ALA is neurotoxic: drives encephalopathy, neuropathy, abdominal colic. Same ALA accumulation seen in AIP, but different enzyme hit.
🔧
Target 2
Ferrochelatase
The final step. Inserts Fe²₊ into protoporphyrin IX to make heme. Lead blocks this, so protoporphyrin IX accumulates. Zinc substitutes for iron, creating zinc protoporphyrin (ZPP), the same thing as FEP on lab reports.
🦸
Why It Looks Like IDA
Normal Iron, Broken Factory
Iron stores are normal or high. Iron cannot be used because ferrochelatase is blocked. So the RBCs end up small and pale (microcytic, hypochromic) just like iron deficiency anemia, but serum iron/ferritin are not low. Transferrin saturation is also normal or high.
AIP vs. Lead comparison: Both hit heme synthesis. AIP knocks out PBG deaminase (step 3). Lead knocks out ALA dehydratase (step 1) and ferrochelatase (final step). AIP gives you neurologic attacks without anemia. Lead gives you microcytic anemia plus neurologic symptoms. The shared upstream toxin is ALA accumulation.
1 / 6
Labs and Findings
Classic clues on the smear and in the blood. Flip each card.
📷 BASOPHILIC STIPPLING · tap to expand
📷 LEAD LINES (METAPHYSEAL BANDS) · tap to expand
🧟
Smear Finding
Basophilic Stippling
tap to reveal mechanism
Trace It
Lead inhibits pyrimidine 5'-nucleotidase (an RNase). Ribosomal RNA cannot be degraded normally. It clumps inside the RBC as visible blue-purple dots under Wright stain. Classic board finding. Coarse stippling = lead. Fine stippling = thalassemia or other causes.
📐
Lab Value
Elevated FEP / ZPP
tap to reveal meaning
What It Means
Free erythrocyte protoporphyrin = zinc protoporphyrin = same thing. Ferrochelatase is blocked, so protoporphyrin IX piles up and zinc grabs the iron-binding site instead. ZPP is a reliable marker of chronic lead exposure. Blood lead level confirms diagnosis; ZPP confirms the heme factory is broken.
🦷
Clinical Sign
Burton's Lines
tap to reveal
Burton's Lines
Blue-gray line at the gingival margin. Lead is deposited in the gums by bacteria (hydrogen sulfide reacts with lead to form lead sulfide). Pathognomonic for chronic lead exposure in adults. Seen in battery workers, smelters, radiator repair. Rare in children.
🦴
Imaging
Lead Lines on X-ray
tap to reveal
Dense Metaphyseal Bands
In children, lead deposits at zones of provisional calcification (growth plates). X-ray shows dense white bands at the metaphyses of long bones, especially the distal femur and proximal tibia. Not actual calcium · it is lead and calcium phosphate. Seen in chronic childhood exposure.
Severe: Encephalopathy, seizures, coma at very high levels.
Imaging: Dense metaphyseal bands on X-ray of long bones.
👷
Adults
Occupational Exposure
Sources: Battery manufacturing, smelting, radiator repair, painting (old leaded paints), plumbing, moonshine distilled through old radiators.
Presentation: Peripheral neuropathy (wrist drop, foot drop from motor axonopathy), abdominal colic, constipation, Burton's lines.
Classic board scenario: Battery worker with wrist drop, anemia, and abdominal pain. Think lead.
Wrist drop vs. foot drop: Both are motor neuropathies from lead. Wrist drop = radial nerve involvement. Foot drop = peroneal nerve involvement. Lead targets long peripheral motor nerves. This distinguishes it from AIP, which also causes neuropathy but in a very different clinical context (acute attacks triggered by drugs/fasting).
🏠
Environmental Risk
Pre-1978 Housing
The US banned lead paint in residential buildings in 1978. Any home built before that date is a risk. Deteriorating paint peels into dust. Children ingest it directly (pica) or through contaminated hands. Low-income, urban housing carries the highest risk. Always ask about housing age in pediatric anemia workup.
🍺
clinical medicine Trap
Moonshine + Abdominal Pain
Classic board vignette: rural adult with recurrent abdominal pain, constipation, peripheral neuropathy, anemia. Drinks homemade alcohol. Old car radiators used as stills contaminate the product with lead. Order a blood lead level in any adult with this constellation. Moonshine vignette appears in clinical practice more than you'd expect.
3 / 6
Chelation Protocol
Blood lead level drives every decision. Walk through the tree.
Board priority: The thresholds and drug choices are high-yield. Know: 5, 45, and 70 mcg/dL as the decision cutoffs. Know that succimer is the only oral chelator. Know that BAL goes before EDTA in severe cases.
What is the blood lead level?
Normal · No Treatment Needed
Blood lead below 5 mcg/dL is within the reference range. No chelation. No action required beyond routine well-child care. Reassure and repeat screening per guidelines if risk factors present.
Elevated · Remove from Source + Monitor
No chelation at this level. The primary intervention is source removal: relocate the child from the hazardous environment, remediate the housing, eliminate exposure. Nutritional support (iron, calcium, vitamin C) may reduce absorption. Repeat blood lead levels at 1 to 3 months. Developmental monitoring is essential.
Blood lead is 45 to 69 mcg/dL. Are neurological symptoms present?
Succimer · Oral Chelation
Drug: SUCCIMER (DMSA)
Dimercaptosuccinic acid. The only oral chelator for lead. Outpatient treatment. Safe for children. Binds lead and promotes renal excretion.
Also remove from source. Follow blood lead levels during and after treatment. FEP/ZPP will normalize slowly over weeks to months.
Blood lead is 70+ mcg/dL (or neurological symptoms present). Which drug goes FIRST?
Incorrect · EDTA Alone Can Worsen Encephalopathy
EDTA given first in encephalopathy mobilizes lead from bone and soft tissue faster than it can be excreted. This redistributes lead to the brain, worsening encephalopathy. Always give BAL first to mobilize and bind lead, then follow with EDTA.
Incorrect · Succimer Is Not for Severe Cases
Succimer is oral and used for moderate levels (45 to 69 mcg/dL) without neurological symptoms. Severe lead poisoning or encephalopathy requires IV/IM chelation with BAL + EDTA. BAL goes first.
Correct · BAL First, Then EDTA
Regimen: DIMERCAPROL (BAL) first, then add EDTA
BAL is given IM (oil-based suspension). It rapidly chelates lead and prevents redistribution to the brain. After BAL is on board (usually after the first dose), EDTA is added to enhance excretion via the kidneys.
Key rule: Never give EDTA alone when encephalopathy is present. BAL first, always.
Blood Lead Level
Action
Drug(s)
< 5 mcg/dL
None
None
5 to 44 mcg/dL
Source removal, monitor
None
45 to 69 mcg/dL
Oral chelation
Succimer (DMSA)
≥ 70 mcg/dL or neuro sx
Dual IV/IM chelation
BAL first → + EDTA
4 / 6
Chelation Drug Profiles
Four drugs. One wins for oral. One goes first in severe cases. Know them cold.
Succimer
DMSA · dimercaptosuccinic acid
RouteORAL only
UseLead 45 to 69 mcg/dL
Also chelatesMercury, arsenic
Board board lock: The ONLY oral chelator for lead. Everything else is IM or IV. If the question asks about outpatient chelation or oral treatment, the answer is succimer.
Dimercaprol
BAL · British Anti-Lewisite
RouteIM only (oil-based)
UseSevere lead (≥ 70) + EDTA
GoesFIRST before EDTA
Originally developed as an antidote for lewisite (World War I nerve agent). Now used for severe lead, arsenic, mercury. Cannot give IV → oil suspension, IM only.
EDTA
Calcium EDTA · ethylenediaminetetraacetic acid
RouteIV or IM
UseSevere lead (with BAL)
CautionNEVER alone in encephalopathy
Chelates lead renally. Given after BAL is on board. EDTA alone in encephalopathy redistributes lead to the brain and worsens the picture. BAL first, then EDTA.
Penicillamine
D-penicillamine
RouteOral
Primary useWilson's disease (copper)
AlsoLead, mercury (2nd line)
Main clinical medicine use is Wilson's disease (copper chelation). It works for lead and mercury too but succimer is preferred for lead. Oral. Side effects: lupus-like reaction, nephrotoxicity, bone marrow suppression.
Quick Matrix · Chelators by Metal
Lead
Succimer (oral, moderate)
BAL + EDTA (severe / encephalopathy)
Penicillamine (second line)
Copper (Wilson's)
Penicillamine (first line)
Trientine (if penicillamine intolerant)
Zinc (maintenance)
Mercury / Arsenic
BAL (dimercaprol)
Succimer (oral alternative)
DMPS (not widely available in US)
Iron Overload
Deferoxamine (acute, IM/IV)
Deferasirox (oral, chronic)
Phlebotomy (hemochromatosis)
Memory hook: BAL was invented to save soldiers from a chemical weapon. It goes FIRST because it is the most aggressive binder. Think of BAL as the front-line soldier. EDTA is the reinforcement that mops up. Succimer is the outpatient pill. Penicillamine owns Wilson's disease. That is the whole chelation map.
5 / 6
Quiz
8 questions. No time pressure. See how much stuck.
Question 1 of 8
A 3-year-old girl lives in a pre-1978 row house. Her mother reports that she eats paint chips from the windowsill. CBC shows hemoglobin 9.2 g/dL, MCV 68 fL. Peripheral smear shows microcytic, hypochromic cells with coarse basophilic stippling. Serum iron is 110 mcg/dL (normal). Blood lead level returns at 55 mcg/dL. She has no seizures or focal neurological deficits. What is the best next step?
The clue: Blood lead 55 mcg/dL (in the 45 to 69 range), no neurological symptoms. The chain: No encephalopathy at this level means parenteral chelation is not yet required. Succimer is the only oral chelator and is approved for outpatient use in children. EDTA alone is contraindicated in encephalopathy, and this child has none but we still avoid it here since succimer handles this range adequately. BAL + EDTA is reserved for levels 70+ or with neuro involvement. Break it down: 45 to 69, no neuro = succimer, oral, outpatient. Always pair with source removal.
Question 2 of 8
A 47-year-old automotive battery factory worker is brought to the ED with confusion, severe abdominal cramping, and bilateral wrist weakness. He cannot extend his wrists against gravity. Blood lead level is 84 mcg/dL. Which chelation regimen is most appropriate?
The clue: Blood lead 84 mcg/dL + confusion (encephalopathy) + wrist drop (motor neuropathy). The chain: This is severe lead toxicity with neurological involvement. Succimer is oral and only for moderate cases without neuro. EDTA alone with encephalopathy redistributes lead to the brain and worsens it. BAL (dimercaprol) goes first because it is the most aggressive binder and prevents redistribution. Once BAL is working, EDTA is layered in to enhance renal excretion. Break it down: Encephalopathy + blood lead 70+ = BAL first, always. Then EDTA. Never EDTA alone in encephalopathy.
Question 3 of 8
Lead inhibits which enzyme at the FINAL step of heme synthesis, causing protoporphyrin IX to accumulate?
The clue: "Final step" + "protoporphyrin IX accumulates." The chain: Ferrochelatase (also called heme synthase) is the last enzyme. It inserts Fe²₊ into protoporphyrin IX. Block it and protoporphyrin piles up. Zinc grabs the empty iron slot instead, producing zinc protoporphyrin (ZPP) = FEP on lab reports. ALA synthase is the rate-limiting first step. ALA dehydratase is the second target lead hits (but early in the pathway). PBG deaminase is the AIP target. Break it down: Two enzyme targets. ALA dehydratase early, ferrochelatase final. Both blocked by lead.
Question 4 of 8
A 5-year-old has a blood lead level of 58 mcg/dL and elevated free erythrocyte protoporphyrin (FEP). His serum iron is 130 mcg/dL. What does the elevated FEP represent?
The clue: Elevated FEP + elevated serum iron + lead exposure. The chain: Ferrochelatase is blocked by lead. Iron cannot be inserted into protoporphyrin IX. The protoporphyrin ring sits empty. Zinc scavenges the binding site, creating zinc protoporphyrin (ZPP). FEP and ZPP are the same measurement reported differently by different labs. Serum iron is high because iron is present but cannot be used. This is the mechanistic fingerprint of lead poisoning. Break it down: High FEP + high (or normal) serum iron = ferrochelatase blockade. The iron is there; the enzyme is not.
Question 5 of 8
A child with a blood lead level of 62 mcg/dL is asymptomatic. His parents ask if he can be treated at home. Which chelating agent makes this possible?
The clue: "Home" treatment + lead 62 mcg/dL (moderate range) + asymptomatic. The chain: Only succimer is oral. BAL is IM-only (oil suspension). EDTA is IV or IM. Deferoxamine chelates iron, not lead. Succimer (dimercaptosuccinic acid / DMSA) was developed specifically as an oral agent that is safe and effective for moderate lead levels in pediatric outpatients. Neurological symptoms or levels 70+ require admission for parenteral therapy. Break it down: Succimer = oral = outpatient. It is the ONLY oral chelator for lead in clinical practice.
Question 6 of 8
A 6-year-old with a blood lead level of 76 mcg/dL and lead encephalopathy is brought to the ED. The team considers immediate chelation. Why is IV EDTA contraindicated as a solo agent in this scenario?
The clue: Encephalopathy + EDTA alone = dangerous. The chain: EDTA chelates lead and promotes renal excretion, but it mobilizes lead from bone and soft tissues before the chelate can be excreted. This free lead redistributes to the brain, which is already inflamed and vulnerable. The result is worsening encephalopathy. BAL is given first because it rapidly binds lead and keeps it bound during mobilization. Only after BAL has been working can EDTA safely be added to assist renal clearance. Break it down: EDTA alone redistributes lead to the brain. BAL prevents this. BAL first. Always.
Question 7 of 8
A 34-year-old man presents with arthralgias, Kaiser-Fleischer rings on slit-lamp exam, elevated liver enzymes, and hemolytic anemia. Ceruloplasmin is undetectable. Which chelating agent is the first-line treatment for his condition, and what other metal does this drug also chelate?
The clue: Kaiser-Fleischer rings + low ceruloplasmin + hemolytic anemia + liver disease = Wilson's disease (copper accumulation). The chain: Penicillamine is the first-line chelator for Wilson's disease. It chelates copper and promotes urinary excretion. It also chelates lead and mercury, making it a second-line option for those toxicities when first-line agents fail or are unavailable. Side effects of penicillamine include lupus-like syndrome, nephrotoxicity, and bone marrow suppression. Break it down: Penicillamine owns Wilson's (copper). It also works on lead and mercury but it's not first-line for either.
Question 8 of 8
A peripheral blood smear from a 52-year-old plumber shows small red blood cells with irregular blue-purple granules scattered throughout the cytoplasm. His hemoglobin is 10.1 g/dL, serum iron is normal, and ferritin is 280 ng/mL. What is the classic name for this smear finding and what is its mechanism?
The clue: Plumber (occupational lead exposure) + microcytic anemia + normal serum iron + blue-purple cytoplasmic granules. The chain: Basophilic stippling is the board classic for lead poisoning. Lead inhibits pyrimidine 5'-nucleotidase, an enzyme that normally degrades ribosomal RNA in maturing RBCs. The RNA aggregates into visible clumps that stain blue-purple on Wright stain. Heinz bodies are oxidized hemoglobin (G6PD deficiency). Howell-Jolly are nuclear remnants. Pappenheimer bodies contain iron (sideroblasts). Break it down: Coarse basophilic stippling + occupational history + normal iron = lead poisoning. Know your RBC inclusions.
questions correct out of 8
6 / 7
clinical Walkthrough
clinical Walkthrough
Original clinical vignettes. Shuffled, never-repeat, full explanations for every choice.
7 / 7
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 1, 2026 at 10:03 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.