Two cholestatic liver diseases. Both cause itching, jaundice, and elevated alk phos. But the patient, the antibody, and the duct histology tell you everything.
Scroll to continue
The Question You Missed
Clinical Images
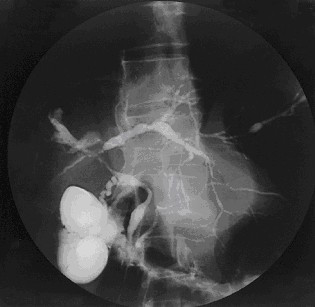
📷 PSC: beading pattern on cholangiogram · tap to expand
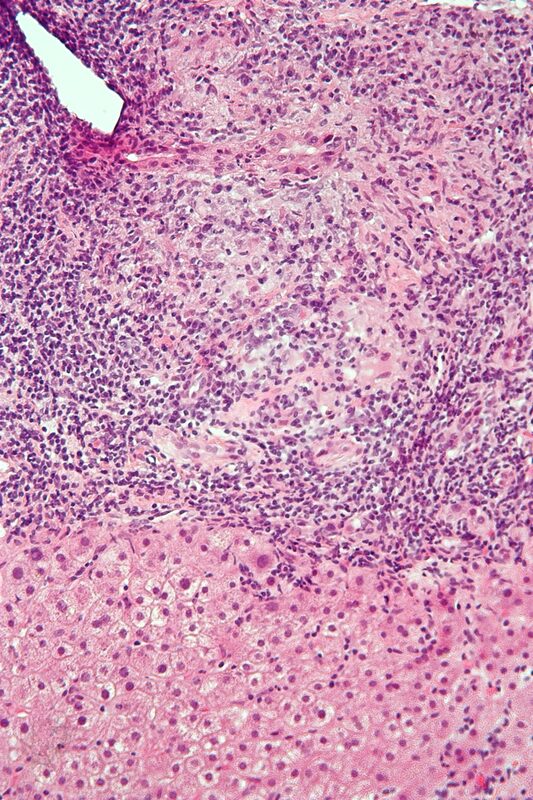
📷 PBC: bile duct destruction on biopsy · tap to expand
A 46-year-old man with a 10-year history of ulcerative colitis presents with worsening fatigue, jaundice, and pruritus. Labs show elevated alkaline phosphatase. Serum p-ANCA is positive. MRCP shows multifocal strictures and dilations of the intrahepatic bile ducts with a "beading" pattern. A liver biopsy is obtained. Which histologic finding is most characteristic?
That's it. Onion-skin fibrosis = PSC. The scar tissue wraps around bile ducts in concentric rings, like layers of an onion. UC + male + pANCA + beading on MRCP = PSC every single time. The concentric fibrosis is what creates the strictures that cause the beading pattern.
That's the exact trap. Here's the breakdown:
Granulomatous destruction = PBC. Those are immune cells surrounding and destroying small bile ducts, driven by anti-mitochondrial antibodies. But this patient is a man with UC · PBC hits middle-aged women.
Ductopenia = late-stage PBC, when the ducts have been destroyed and disappear.
Interface hepatitis with plasma cells = autoimmune hepatitis, a different disease entirely.
The answer is periductal concentric ("onion-skin") fibrosis · the hallmark of PSC. UC + male + pANCA + beading on MRCP. Those four clues all point one direction.
The Pattern
One Sentence Each
If you can say these from memory, you can answer any board question on this topic.
PSC = man with UC + pANCA + beading on MRCP + onion-skin fibrosisPicture an onion cut in cross-section. Each ring is scar tissue wrapping tighter around the bile duct, strangling it shut. That's PSC histology. The duct doesn't get destroyed, it gets squeezed. → cholangiocarcinoma10-15% lifetime risk. Chronic duct inflammation breeds cancer in those ducts. Screen with CA 19-9. The name: sclerosing = scarring = cancer risk in the scarred tissue. risk.
PBC = middle-aged woman + AMA positiveAnti-mitochondrial antibody. Positive in 95% of PBC patients. The immune system is attacking the pyruvate dehydrogenase complex on mitochondria in bile duct cells. That's the bullseye. AMA = PBC until proven otherwise. + granulomatous destruction of small bile ducts + xanthomasBile can't drain, so cholesterol builds up in blood. It deposits in skin (xanthomas) and around eyes (xanthelasma). Sky-high total cholesterol in a middle-aged woman with pruritus = think PBC. → ductopenia late.
Side by Side
The Split Screen
Everything that separates them, in one view.
PSC
Full NamePrimary Sclerosing Cholangitis
WhoMiddle-aged men (30-40s). M:F ~ 2:1.
Associated DiseaseUlcerative colitis (80-90% of PSC patients have UC). Does NOT improve after colectomy.
Antibodyp-ANCA (perinuclear antineutrophil cytoplasmic). AMA negative.
Which DuctsLarge intra- and extrahepatic bile ducts.
ImagingBeading on MRCP · alternating strictures and dilations. Diagnostic.
HistologyOnion-skin fibrosis · concentric periductal scarring wrapping around ducts.
Trace ItFibrosis and scarring around ducts → strictures → cholestasis.
Cancer RiskCholangiocarcinoma (10-15% lifetime). Screen with CA 19-9.
TreatmentLiver transplant is the only cure. Ursodeoxycholic acid may help labs but not survival.
Picture an onion sliced in cross-section. Each ring is a layer of scar tissue. Now put a bile duct in the center. That's onion-skin fibrosis · concentric rings of collagen wrapping tighter and tighter around the duct, squeezing it shut. The duct doesn't get destroyed. It gets strangled. That's why you see strictures on imaging.
Sensory · Beading Pattern
A normal bile duct on MRCP looks like a smooth tube. In PSC, the onion-skin fibrosis creates alternating tight spots (strictures) and ballooned spots (dilations). The result looks like a string of beads · narrow-wide-narrow-wide. That beading pattern on MRCP is enough to diagnose PSC without a biopsy.
Sensory · PBC Granulomatous Destruction
Imagine a cluster of immune cells surrounding a tiny bile duct like a mob. They're not scarring it from outside · they're eating it alive from within. Granulomatous = organized clusters of macrophages (epithelioid cells, giant cells). Eventually there's nothing left. The duct vanishes. That's ductopenia · you look on biopsy and the ducts that should be there simply aren't.
Board Traps
Where People Get Tricked
These are the exact traps that lose you points. Each one is a pattern you need to recognize.
PSC does NOT improve after colectomy. Even though PSC is linked to UC, removing the colon does NOT cure or slow PSC. It runs its own course. The cholangiocarcinoma risk persists. If a question says "patient had colectomy for UC, what happens to their liver disease?" · the answer is nothing. It keeps going.
PBC histology is NOT ductopenia on its own. Ductopenia is the late finding when ducts have already been destroyed. The characteristic finding is granulomatous destruction of bile ducts. If they show you ductopenia alone, that's a nonspecific late-stage cholestatic disease · not enough to nail PBC.
Both cause elevated ALP · do NOT use ALP to distinguish. Both PSC and PBC are cholestatic diseases with elevated alkaline phosphatase. The distinguishing labs are antibodies: p-ANCA (PSC) vs AMA (PBC). The enzyme pattern tells you "cholestatic." The antibody tells you which one.
PBC has a NORMAL MRCP. This one trips people hard. PBC destroys small intrahepatic ducts · way too small to see on imaging. If the MRCP shows beading, that's PSC. If the MRCP is clean, think PBC and order AMA.
"Sclerosing" = scarring. "Biliary" = bile duct itself. The name tells you the mechanism. PSC scleroses (scars around) ducts. PBC attacks the biliary (duct) cells directly. If you remember only the names, you know the histology.
Clinical Pearls
The Details That Clinch It
Tap each card to reveal the answer.
Pruritus
Which is more itchy?
PBC · pruritus is often the presenting symptom, sometimes years before jaundice. Bile acid deposition in skin. PSC causes pruritus too, but typically after jaundice develops.
Skin Findings
Xanthomas and xanthelasma?
PBC. Cholesterol can't be excreted in bile → hyperlipidemia → cholesterol deposits in skin (xanthomas) and around eyes (xanthelasma). Not typical of PSC.
Diagnosis
Which needs a biopsy?
Neither requires one for diagnosis. PSC = MRCP (beading pattern). PBC = AMA + elevated ALP. Biopsy helps staging but is not needed to make the call.
Cancer Type
Different cancer risks?
PSC → cholangiocarcinoma (bile duct cancer). PBC → hepatocellular carcinoma (once cirrhosis develops). Different cancers, different surveillance.
UDCA Response
Does UDCA help?
PBC · UDCA (ursodeoxycholic acid) is first-line and slows progression. In PSC, UDCA improves lab values but does NOT improve survival or prevent transplant. Treatment response = PBC clue.
Overlap
Can you have both?
Yes. PSC-AIH overlap and PBC-AIH overlap exist. If someone with PSC or PBC has unexpectedly elevated transaminases + ANA/anti-smooth muscle Ab, consider overlap with autoimmune hepatitis.
Feature
PSC
PBC
Sex
Male
Female
Age
30-40s
40-60s
Association
UC (80-90%)
Autoimmune (Sjogren, CREST)
Antibody
p-ANCA
AMA
Duct size
Large (intra + extrahepatic)
Small (interlobular only)
MRCP
Beading
Normal
Histology
Onion-skin fibrosis
Granulomatous destruction
Late finding
Strictures, cirrhosis
Ductopenia
Skin signs
Jaundice
Xanthomas, xanthelasma
Cancer risk
Cholangiocarcinoma
Hepatocellular carcinoma
Treatment
Transplant only
UDCA (slows disease)
Labs (shared)
Elevated ALP, direct bilirubin, GGT. Cholestatic pattern.
Sort It Out
Feature Sorting
Drag each feature into the right disease. Wrong guesses bounce back.
PSC
PBC
Memory Hooks
Burn These In
Tap to reveal each mnemonic.
PSC Hook
Tap to reveal
"PSC = Perinuclear ANCA, Sclerosing (scarring), Cholangiocarcinoma" · The name IS the disease. Scarring around ducts, cancer risk, and the antibody that goes with UC.
PBC Hook
Tap to reveal
"PBC = Pretty Bad Cholesterol" · Middle-aged women with sky-high cholesterol, xanthomas everywhere, and itching that won't quit. AMA-positive. Granulomas eating ducts alive.
The Histology Hook
Tap to reveal
"Sclerosing = Strangles from outside (onion-skin)" vs "Biliary = Burns from inside (granulomas)" · S wraps around. B bores in. Different letters, different directions of attack.
The Sex Hook
Tap to reveal
"PSC = Sir (male)" and "PBC = Belle (female)" · The second letter tells you the sex. S for Sir. B for Belle.
The Villains
Meet Your Board Adversaries
Tap each card to flip and reveal what makes each one unique in clinical practice.
🏃
PSC: The Strangler
Tap to reveal
PSC Fingerprint
Male, 30-40s. IBD (UC) in 80-90%. Scars bile ducts from outside with onion-skin fibrosis. Beading on MRCP. p-ANCA positive. Cancer risk: cholangiocarcinoma. No medical cure, only transplant.
🔥
PBC: The Destroyer
Tap to reveal
PBC Fingerprint
Female, 40-60s. AMA positive (95%). Granulomatous destruction of small interlobular ducts. Normal MRCP. Xanthomas + xanthelasma from bile cholesterol. UDCA actually works here.
🔍
PSC: The Imager
Tap to reveal
MRCP Tells All
PSC affects LARGE ducts visible on MRCP. The alternating strictures and dilations create a beading pattern. MRCP showing beading = PSC diagnosis without needing a biopsy. Normal MRCP rules PSC out.
🧬
PBC: The Invisible
Tap to reveal
Invisible on Imaging
PBC destroys SMALL intrahepatic ducts. Too tiny for MRCP to see. If MRCP is normal but ALP is high in a middle-aged woman, order AMA. That antibody is your diagnosis tool, not the scanner.
🇮🇳
PSC: Cancer Factory
Tap to reveal
Cholangiocarcinoma
10-15% lifetime risk of cholangiocarcinoma. Chronic bile duct inflammation breeds cancer in those ducts. Screen annually with CA 19-9. Courvoisier sign (palpable gallbladder) + sudden jaundice in a PSC patient = cancer until proven otherwise.
⚡
PBC: The Pretzel
Tap to reveal
UDCA: The One Med That Works
UDCA (ursodeoxycholic acid) actually slows PBC progression. Replaces toxic hydrophobic bile acids with a gentler hydrophilic version. First-line. In PSC, UDCA improves labs but does NOT improve survival. clinical medicine love this distinction.
Decision Tree
Cholestatic Liver Disease: PSC vs PBC vs Other
Follow each branch. Tap an option to reveal where it leads.
Patient with elevated ALP + jaundice. Where do you go first?
↓
↓
PSC (Primary Sclerosing Cholangitis) p-ANCA positive. ALP markedly elevated. IgM may be elevated. UC association (most common IBD link). Cholangiocarcinoma risk. No cure. Liver transplant is definitive.
↓
Choledocholithiasis or malignancy Proceed to ERCP + brush cytology
Autoimmune Hepatitis Elevated transaminases. IgG elevated. Liver biopsy confirms. Treat with steroids and azathioprine.
↓
Drug-induced cholestasis or other cause Review medications. Consider primary biliary cholestasis of pregnancy if applicable.
Test Yourself
Quiz
5 random questions from a pool of 10. Shuffled answers. No timer. Wrong is safe here.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 5, 2026 at 8:17 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.