Your own digestive enzymes leak inside the organ and start digesting it. Same disease in kids and adults, completely different reasons. Let's walk the chain.
The Stem You'll See
Mid-Epigastric, Bores to the Back
One of the most stereotyped pain stories in medicine. If you can name the pain, you're already at the diagnosis.
Patient comes in with severe mid-epigastric pain
that radiates straight to the back.
They lean forward to make it stop. Nausea. Vomiting.
🔑Pancreas sits behind the stomach. Pain shoots backward because that's where the organ actually lives.
That radiation pattern isn't random. The pancreas is a
retroperitonealSits behind the lining of the abdominal cavity, glued to the back wall. Not floating in the gut like the intestines.
organ. Inflammation there leaks straight into the back muscles. Stomach pain shoots forward; pancreas pain shoots backward. Same body, different address.
Challenge Before Reveal
Why Does It Bore to the Back?
Before you scroll past, pick the right answer. There is no wrong-answer punishment here, just the reasoning chain.
A patient lurches in clutching the epigastrium, leaning forward. Pain shoots through to the back. Why backward?
B is the clean answer. The pancreas lives behind the stomach, mortared to the back wall of the abdomen. When the organ inflames, the inflammation has nowhere to bulge except backward into the muscles that hug the spine. Leaning forward stretches those muscles away from the pancreas, which is why patients curl into a ball.
The other choices borrow real concepts but apply them wrong. Gallstone pain hits the right shoulder via the phrenic nerve, not the back. The vagus carries afferent sensation but doesn't dump it into the lumbar spine. Memorize the address: retroperitoneal = back pain.
Clinical Photos
What the Pancreas Actually Looks Like
Tap any image to expand. These are the visual anchors for clinical practice.
🎯 ANATOMY · tap to expand
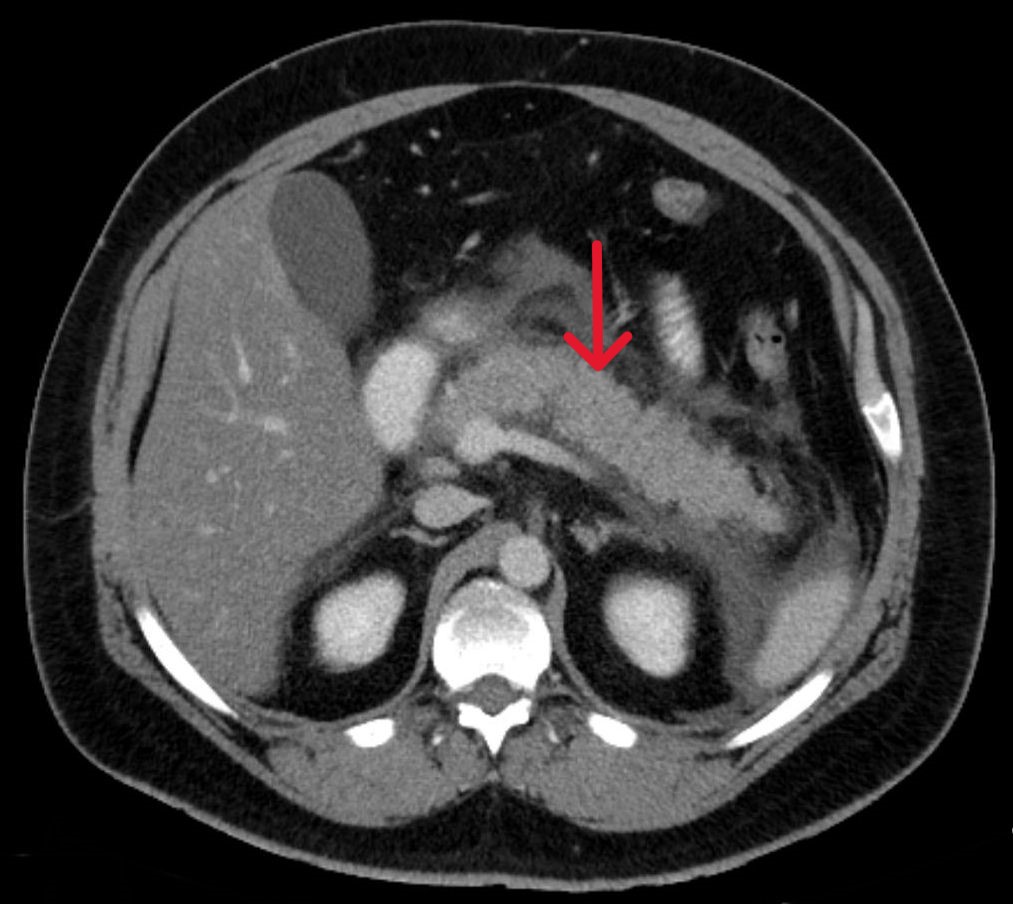
🧬 CT WITH NECROSIS · tap to expand
🪁 CULLEN SIGN · tap to expand
1 / 5
Section 2 of 5
Same Organ, Two Stories
A 7-year-old and a 47-year-old can both be wheeled in with the exact same pain pattern. Their backstories are nothing alike. Pick a patient.
The kid story. Pancreatitis in children is almost always something happened to the organ. They don't drink and they don't have gallstones, so the etiology list is short and sharp.
🔑Kid mnemonic: Trauma, Infection, Fat, Calcium. "TIFC" - kids get pancreatitis from the outside in.
1
Abdominal Trauma
Handlebar to the gut, MVA, NAT
▾
The single most common cause in kids. Bike handlebar to the belly. Car crash. Kicked in a fight. The pancreas sits in front of the spine, so a direct hit crushes it against bone. Enzymes leak out the bruised duct and start digesting the surrounding tissue. Suspect this in any kid with mid-epigastric pain after a fall, a sport, or unexplained bruising.
2
Infections
Coxsackie B, EBV, mumps
▾
Viruses with a taste for glandular tissue. Mumps is the classic; it's the same virus that swells parotid glands, and the pancreas is just another big secretory gland the virus can hit. Coxsackie B and EBV round out the trio. The kid has a viral prodrome (fever, fatigue, parotid swelling), then the belly lights up.
3
Hypertriglyceridemia
Genetic lipid disorder
▾
In kids this is almost always a familial hyperlipidemia, not diet. Triglycerides above ~1000 mg/dL turn the blood into a milky soup that the pancreas can't handle. Lipase tries to clear it and ends up activating inside the organ. The kid often has a family history of early pancreatitis or weird lipid labs.
4
Hypercalcemia
Calcium flooding the duct
▾
High calcium in the blood drives trypsinogen activationTrypsinogen is the inactive form of the master enzyme. Calcium snaps it on prematurely, inside the pancreas instead of inside the small intestine where it belongs. inside the duct itself. Once trypsin turns on early, every other enzyme follows like dominoes. Common pediatric causes of hypercalcemia: hyperparathyroidism (rare in kids), vitamin D toxicity, malignancy.
The adult story. Adults break their pancreas from the inside out. The big two own the entire list. If a stem doesn't mention either, you're hunting one of the smaller suspects.
🔑Adult mnemonic: G-A-T-C: Gallstones, Alcohol, Triglycerides, Calcium. The two biggest letters are G and A; everything else is a footnote.
1
Gallstones
Stone in the common duct
▾
The single most common adult cause. The pancreatic duct and the common bile duct dump into the duodenum through one shared opening. A gallstone wedges in that opening and bile backs up into the pancreas. The trapped enzymes activate early, and the cascade starts. Female, fertile, forty, fat = the classic gallstone risk profile, and the same patient who shows up with pancreatitis.
2
Alcohol
Direct toxic injury
▾
Ethanol is directly toxic to the pancreatic acinar cells. Chronic heavy use thickens pancreatic secretions, blocks small ducts, and triggers premature enzyme activation. The classic stem: middle-aged man, history of binge drinking, presents the morning after a bender with epigastric pain shooting straight to the back.
3
Hypertriglyceridemia
Triglycerides over 1000
▾
Same mechanism as the kid version, different cause. In adults it's usually acquired: uncontrolled diabetes, obesity, certain medications. When triglycerides crest 1000 mg/dL, lipase activity inside the pancreas itself starts cleaving them and the free fatty acids damage the organ.
4
Hypercalcemia
Think Multiple Myeloma
▾
In adults, the buzzword pairing is multiple myeloma. Myeloma's bone destruction floods the blood with calcium. Calcium then drives trypsinogen activation inside the pancreatic duct, lighting up the cascade. Stem clues: older adult, bone pain, anemia, renal dysfunction, plus the classic mid-epigastric pain shooting to the back.
2 / 5
Section 3 of 5
The Saponification Loop
This is the crown jewel concept. Step through it one beat at a time. Once the loop closes, the pancreas can't stop digesting itself.
Step 1 of 5
Damaged pancreatic cells release lipase. The enzyme was supposed to stay locked up until the small intestine; now it's loose inside the organ.
Why "saponification"? Saponification is literally how soap is made: fatty acids bond to a metal ion. Inside an inflamed pancreas, free fatty acids grab calcium and form
white, chalky deposits
in the fat around the organ. Patient labs:
low serum calcium because it's being eaten by FFAs and dropped into the pancreatic fat.
The deposits then irritate more pancreatic fat, which inflames more cells, which leak more lipase. The loop accelerates. That's why the disease can spiral so fast: it's a chemistry chain reaction the body can't shut off without intervention.
🔑Soap = Saponification. Fatty acid + calcium = soap. The pancreas is literally making soap in its own fat.
3 / 5
Section 4 of 5
Catching It in the Imaging
You won't see a "diagnose pancreatitis" question. You'll see a stem with the pain story and a list of imaging studies. Eliminate your way down.
You've got a 9-year-old who took a soccer kick to the gut. Mid-epigastric pain shooting to the back. You're picking the imaging. Eliminate the worst choice first.
Loading clue...
The full workup, in order. clinical medicine loves "what do you order first?" Don't jump to CT before you've justified it.
Abdominal XR · Cheap, fast, rules out free air or obstruction. May show a sentinel loop (distended bowel near the pancreas).
Ultrasound · Best first imaging for gallstones in adults. Painless, no radiation, kid-friendly.
CT scan · The definitive look at the pancreas itself. Used when the diagnosis is uncertain, complications are suspected (necrosis, abscess), or you need to confirm severity.
When It Gets Scary
Hemorrhagic Pancreatitis Signs
Two physical exam findings that mean bleeding into the retroperitoneum. 40% mortality. Recognize them on sight.
Grey Turner's sign: bruising along the
flanksSide of the body between the lower rib and the hip. Where you'd put your hand if you said "hand on my flank.".
Blood is leaking laterally from the retroperitoneum.
🔑Grey Turner = Going sideways. Bruise tracks to the flanks.
Cullen's sign: bruising around the
umbilicusBelly button. The blood tracks forward through tissue planes toward the front of the abdomen..
Blood is leaking forward and pooling at the belly button.
🔑Cullen = Center / belly button. C's line up.
4 / 5
Section 5 of 5
Cement the Loop
One clinical vignette at a time. Cross out with right-click or long-press, highlight with double-click or double-tap, then commit.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 1, 2026 at 10:03 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.