Why the liver is the most common site for metastatic cancer, which tumors take which highway, and the CT finding you cannot miss in clinical practice.
Opening Challenge
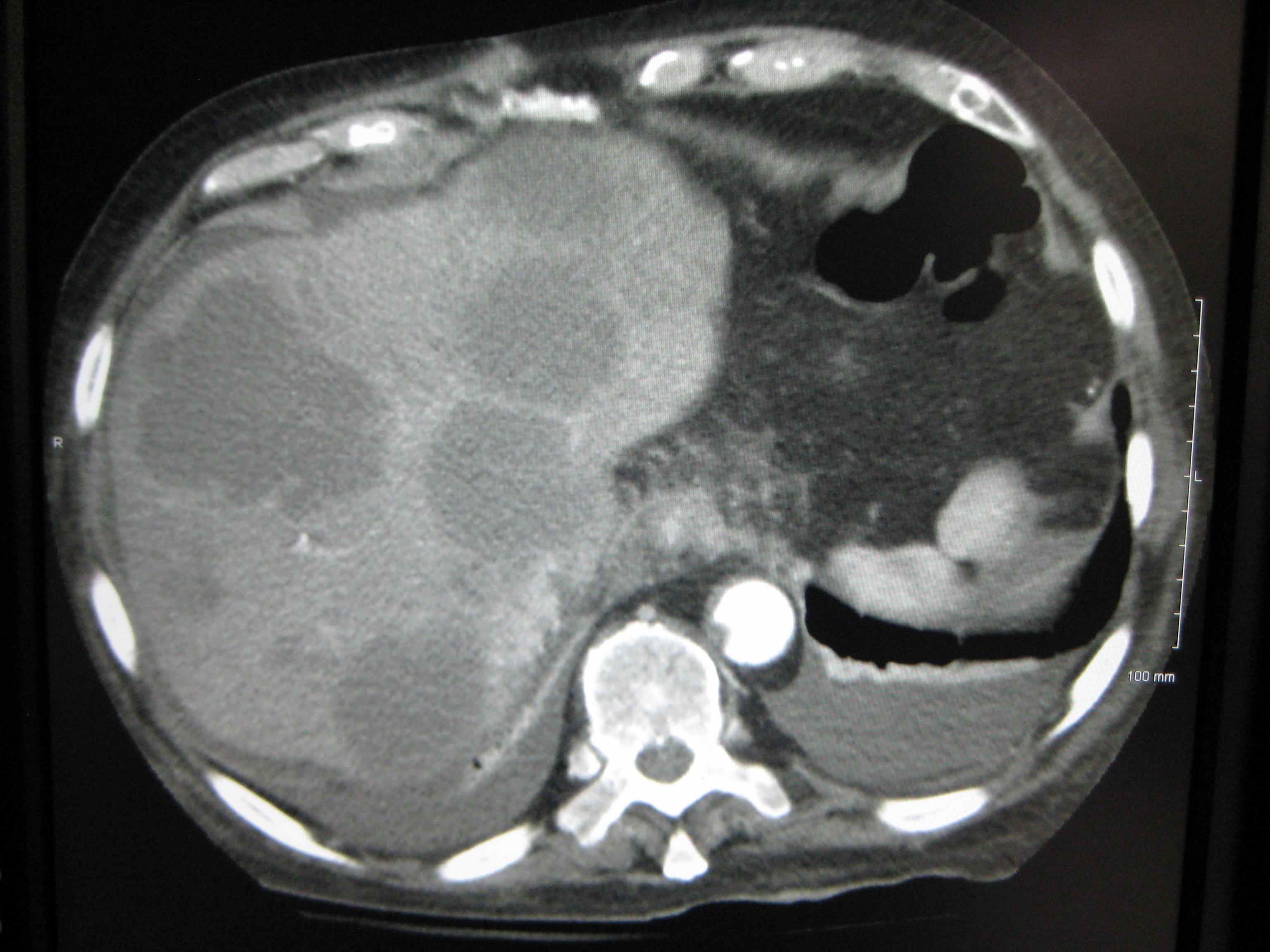
A 58-year-old man with a history of colon cancer presents for staging. CT abdomen shows multiple hypodense lesions scattered through both lobes of the liver, each with a hyperdense rim. ALP is elevated. Liver enzymes are mildly elevated. Which vessel most likely carried these cells to the liver?
A) Portal vein
B) Hepatic artery
C) Lymphatic channels
D) Hepatic veins
Portal vein is the highway for GI cancers. The colon drains into the portal venous system, which flows directly into the liver. Any tumor shed from the gut hits the liver's sinusoidal filter first, before reaching the systemic circulation. That is why colon cancer is the most common cause of liver mets in the US. The hepatic artery carries systemic blood, so lung, breast, and melanoma come in that way instead. GI primaries travel portal. Everything else travels arterial.
01 · The Two Highways
Portal vs Arterial
The liver has two blood supplies. Cancer exploits whichever one drains its home organ.
The Rule: If the primary tumor drains into the portal system (GI tract), cells hit the liver first. If the primary is elsewhere (lung, breast, melanoma, renal), cells enter systemic circulation, reach the heart, then travel via the hepatic artery. Portal first = GI tumors. Arterial = everyone else.
Portal Route (GI tract)
Colon / Rectal CA #1 in US
Gastric CA
Pancreatic CA
Small bowel CA
Carcinoid tumors
Arterial Route (systemic)
Lung CA
Breast CA
Melanoma
Renal Cell CA
Thyroid CA
A pancreatic head tumor sheds cells into venous drainage. Before those cells ever see the lungs, which filter do they hit first?
⚠️
clinical medicine Trap: Most Common vs Primary
Metastatic disease is far more common in the liver than primary HCC. If the stem says "multiple liver masses" with a known primary elsewhere, the answer is mets. HCC almost always arises in a cirrhotic liver with elevated AFP. Multiple lesions in a non-cirrhotic patient = mets until proven otherwise.
📺
Cannon Ball Mets
"Cannon ball" lesions on CXR (multiple large round bilateral pulmonary nodules) suggest renal cell carcinoma or thyroid cancer. These tumors also tend to give vascular, hypervascular liver mets. Not colon. Not breast.
02 · Vessel Map
Anatomy of the Trap
Two entry points. Two tumor populations. One organ that catches them both.
Portal route (GI tumors)
Arterial route (systemic tumors)
Met nodules
Pattern Card · Liver Metastases
Route
Portal (GI) · Hepatic artery (systemic)
Most Common
Colon CA (US) → Portal vein → Liver
CT Finding
Hypodense center, hyperdense rim ("target sign")
Lab Clue
Elevated ALP + GGT > AST/ALT (biliary obstruction pattern)
Surgery
Resection curative only for isolated colon CA mets
Tx (unresectable)
5-FU + bevacizumab (colon mets, first-line)
03 · Clinical Evidence
What It Looks Like
Histology and CT imaging are board-tested visual anchors. Know both.
📷 HISTOLOGY (H&E) · Infiltrating malignant glands · tap to expand
📷 CT ABDOMEN WITH CONTRAST · Hypodense lesions · tap to expand
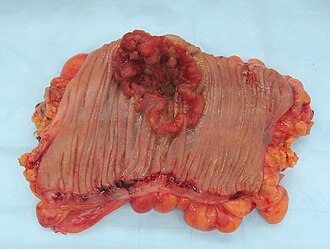
📷 COLORECTAL PRIMARY · Portal source tumor · tap to expand
CT target sign: Hypodense center (necrotic tumor) surrounded by hyperdense rim (viable cells + enhancement). This "target lesion" pattern on contrast CT is the classic imaging finding for liver mets, especially from colon CA. Not to be confused with the arterial enhancement of HCC ("washout" pattern).
04 · Active Game
Route Sorter
Drag each tumor to its metastatic highway. Know this cold and you will never miss a route question.
Route Sorter
Drag each primary tumor to its correct liver route. Portal = drains into portal venous system. Arterial = systemic circulation first.
Colon CA
Breast CA
Lung CA
Pancreatic CA
Renal Cell CA
Melanoma
Gastric CA
Thyroid CA
🌲 PORTAL ROUTE GI TRACT DRAINS HERE
🟧 ARTERIAL ROUTE SYSTEMIC CIRC FIRST
05 · Case Study
Staging Day
A patient with sigmoid colon cancer hits the CT scanner. Watch the cells move.
Carlos
Sigmoid Colon CA · Staging
"56-year-old. Sigmoid colon adenocarcinoma just diagnosed. Staging CT today. Where do the cells go first?"
The Portal Trap
Tap to trace the portal path
CT Report
Primary
Sigmoid colon adenocarcinoma
Route
Portal vein → hepatic sinusoids
CT
Multiple hypodense lesions, hyperdense rim
Labs
ALP ↑ GGT ↑ > AST/ALT
Next step
Biopsy → staging → resectability assessment
06 · Lock It In
Board Drill
Five patient scenarios. Route, imaging, lab pattern, primary vs metastasis, and treatment all get tested through the same button mechanism.
Q1 of 5
A 62 year old man treated 18 months ago for sigmoid colon adenocarcinoma returns with early satiety, dull right upper quadrant pressure, and an 8 lb weight loss. Temperature is 37.1 C, blood pressure is 126/78 mm Hg, pulse is 86/min, and respirations are 14/min. Examination shows mild hepatomegaly without ascites. Contrast CT shows multiple low attenuation hepatic lesions in both lobes with enhancing rims. Labs show ALP 420 U/L, GGT 310 U/L, ALT 55 U/L, AST 60 U/L, total bilirubin 1.4 mg/dL (normal: 0.1 to 1.2 mg/dL), AFP 5 ng/mL (normal: less than 10 ng/mL), and CEA 318 ng/mL (normal: less than 5 ng/mL). Which mechanism best explains the enzyme pattern?
Why B is right: ALP and GGT are the bile duct enzymes. When metastatic nodules press on small intrahepatic ducts, bile backs up, so ALP and GGT rise more than AST and ALT. The CT pattern and CEA tie the lesions to colorectal metastases riding the portal route.
Option A: Good instinct because tumor is inside the liver, but direct hepatocyte injury makes AST and ALT dominate. This stem makes the duct enzymes louder. AST/ALT dominant = hepatocyte injury; ALP/GGT dominant = cholestasis.
Option C: Portal hypertension is a pressure problem from scarred or blocked blood flow. It explains ascites and varices, not a duct enzyme pattern. Pressure signs point portal; ALP/GGT point bile duct compression.
Option D: Autoimmune hepatitis is an inflammatory hepatocyte attack, so AST and ALT would be the main abnormal labs. A metastatic nodule does not create anti smooth muscle disease just by existing. Do not invent autoimmune hepatitis when the cancer anatomy explains the labs.
Option E: Viral hepatitis would also be AST/ALT heavy and would not explain CEA 318 plus rim enhancing liver lesions. CEA plus colon history plus multiple liver lesions points to colorectal metastases.
Q2 of 5
A 58 year old postmenopausal woman is diagnosed with invasive ductal carcinoma of the breast. The tumor is ER positive, PR positive, and HER2 negative. Staging CT shows two discrete hepatic lesions measuring 2.3 cm and 1.8 cm, and biopsy confirms metastatic breast carcinoma. Vital signs are normal. She has no confusion, no coagulopathy, and no rapidly rising bilirubin. Which treatment approach is most appropriate for the liver disease at this point?
Why A is right: ER positive metastatic breast cancer is systemic disease that usually starts with endocrine therapy, not a local liver procedure, unless there is visceral crisis. The liver lesions arrived through systemic circulation and the hepatic artery, so treatment must reach the whole system.
Option B: This is the colorectal trap. Isolated colorectal liver metastases can be resected with curative intent; breast liver metastases usually represent systemic spread. Cutting out two visible seeds does not treat the invisible field. Curative liver met resection belongs to selected colorectal metastases, not routine breast metastases.
Option C: HAI floxuridine is a liver directed strategy validated mainly for colorectal liver metastases. It is the wrong tool for HR positive breast cancer. Match liver directed pumps to colorectal disease, not ER positive breast disease.
Option D: Whole liver radiation is palliative when options are exhausted. This patient is stable and has hormone sensitive disease. Do not use end stage palliation before systemic first line therapy.
Option E: Breast does not drain through the portal vein. It reaches the liver through systemic circulation and the hepatic artery. GI tumors ride portal; breast rides arterial.
Q3 of 5
A 70 year old man comes in because of 3 months of early satiety, fatigue, and an unintentional 14 lb weight loss. Temperature is 36.9 C, blood pressure is 132/82 mm Hg, pulse is 88/min, and respirations are 15/min. He drinks one glass of wine weekly and has no history of hepatitis, cirrhosis, or alcohol use disorder. Examination shows a firm liver edge. CT abdomen shows multiple hypodense lesions scattered throughout both lobes with a target appearance on contrast. AFP is 8 ng/mL (normal: less than 10 ng/mL). Which diagnosis is most likely?
Why C is right: Metastases are more common than primary cancer in liver, lung, bone, and brain. Multiple scattered lesions in a noncirrhotic liver with normal AFP are metastases until proven otherwise, even when the primary is still hidden.
Option A: HCC is the home grown liver cancer. It usually appears in damaged soil: chronic hepatitis, cirrhosis, aflatoxin exposure, or another major risk factor, and AFP often rises. Single mass plus cirrhosis plus AFP points HCC; multiple lesions plus normal AFP points metastases.
Option B: Hemangiomas are common benign vascular lesions, but their CT pattern is peripheral nodular enhancement with fill in toward the center. This stem says multiple target lesions with systemic symptoms. Target lesions with weight loss are not incidental hemangiomas.
Option D: Abscesses need an infection story: fever, leukocytosis, sepsis, biliary infection, or immunosuppression. This patient has cancer physiology, not pus physiology. No fever or leukocytosis means do not make multiple target lesions into abscesses.
Option E: Autoimmune hepatitis causes inflammatory liver injury and high AST/ALT, not multiple rim enhancing masses. Inflammation changes enzymes; metastases make masses.
Q4 of 5
A 64 year old man with painless hematuria and a 20 pack year smoking history develops progressive cough and dyspnea. Temperature is 37.0 C, blood pressure is 142/86 mm Hg, pulse is 92/min, and oxygen saturation is 95% on room air. Examination shows a ballotable left flank mass. Chest radiograph shows multiple large, round, well circumscribed nodules in both lungs. CT abdomen shows an enhancing left renal mass. Which route pattern best explains the lung finding?
Why A is right: Painless hematuria plus an enhancing renal mass points to renal cell carcinoma. RCC spreads hematogenously and classically gives large, round bilateral lung nodules called cannonball metastases. Thyroid cancer can also do this, but the kidney clues make RCC the answer here.
Option B: Colon cancer can later reach the lungs, but the first filter for colon drainage is the liver through the portal vein. It is not the classic cannonball pattern. Colon first seeds liver; RCC is the cannonball lung board image.
Option C: Pancreatic cancer commonly seeds liver first through portal drainage. Direct extension through the diaphragm is not how it produces bilateral round pulmonary nodules. Pancreas to liver is portal; cannonball lungs are hematogenous RCC or thyroid.
Option D: Breast cancer can metastasize to lung, liver, bone, and brain, but lymphatic spread does not explain multiple round vascular nodules in both lungs plus hematuria and renal mass. The kidney clues outrank a generic breast metastasis pattern.
Option E: HCC can invade vessels, but this patient does not have cirrhosis, hepatitis, AFP clues, or a primary liver mass. Do not choose HCC when the stem hands you RCC.
Q5 of 5
A 55 year old man had a left hemicolectomy for colon adenocarcinoma 14 months ago. Surveillance CT now shows three hepatic metastases confined to the right lobe, largest 3.1 cm. CT chest shows no pulmonary nodules. Peritoneal surfaces are clear. ECOG performance status is 0, bilirubin is 0.8 mg/dL (normal: 0.1 to 1.2 mg/dL), INR is 1.0 (normal: 0.8 to 1.1), and volumetric planning shows adequate future liver remnant. Which next step best matches the management principle tested here?
Why C is right: Selected colorectal liver metastases are the major exception: if all disease can be removed with clear margins, enough liver remains, and there is no unresectable extrahepatic spread, hepatic resection can be done with curative intent.
Option A: This is too fatalistic. Liver metastases often mean advanced disease, but isolated resectable colorectal liver metastases are not automatically terminal. Selected colorectal liver mets can be surgically curable.
Option B: 5-FU plus bevacizumab and FOLFOX based treatment are standard systemic options for unresectable colorectal liver metastases, and chemotherapy can downstage disease. But in a technically resectable patient, chemo alone is not the curative choice. Unresectable gets systemic therapy; resectable colorectal liver mets get a surgical conversation.
Option D: Radiation can palliate or treat selected local problems, but it is not the standard definitive approach for resectable colorectal liver metastases. For resectable colorectal liver disease, the knife beats whole liver radiation.
Option E: Transplant is for selected primary liver tumors such as HCC under criteria and for liver failure, not standard colorectal metastases. Immunosuppression after transplant is a bad setup for microscopic systemic cancer. Confined to liver does not make colorectal metastases a transplant disease.
Board Style Walkthrough
Board Style Walkthrough
Five shuffled patient scenarios. The engine never repeats a case until the set is exhausted and every choice teaches.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 1, 2026 at 10:03 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.