The two faces of IBD. One burrows deep. The other stays on the surface and bleeds. Knowing which does what is the entire game in clinical practice.
Scroll to continue
Before We Start
Clinical Images
📷 Crohn: transmural inflammation, skip lesions · tap to expand
📷 UC: continuous mucosal inflammation · tap to expand
A 28-year-old woman presents with chronic bloody diarrhea, abdominal pain, and a 10-lb weight loss. Colonoscopy shows continuous inflammation from the rectum to the splenic flexure with loss of haustra and pseudopolyps. Biopsy shows crypt abscesses limited to the mucosa. Which feature MOST strongly distinguishes this from Crohn's disease?
Good catch. Continuous inflammation starting at the rectum is the single strongest distinguisher. Crohn's is patchy (skip lesions) and can spare the rectum entirely. UC always starts at the rectum and extends proximally without gaps. Bloody diarrhea, weight loss, and pseudopolyps can appear in both.
Close, but not quite. That finding can appear in both Crohn's and UC. The key distinguisher here is continuous inflammation starting at the rectum · UC always begins at the rectum and extends proximally without skip areas. Crohn's is patchy and can spare the rectum. That pattern of involvement is the most reliable differentiator in clinical practice.
Side by Side
The Big Picture
Everything that makes them different, in one glance.
CROHN'S
LocationMouth to anus (anywhere in GI tract). Terminal ileum is most common.
PatternSkip lesions · patchy, discontinuous. Can spare the rectum.
DepthTransmural · full thickness, all layers of bowel wall.
Smoking paradox: Smoking worsens Crohn's but is protective against UC. This is one of the most tested board facts in IBD. The mechanism likely involves nicotine's effects on mucus production, colonic blood flow, and immune modulation.
Bloody diarrhea does NOT automatically mean UC. Crohn's colitis can also cause bloody stool. The distinguishing factor is the pattern of inflammation (continuous vs skip) and depth (mucosal vs transmural), not the presence of blood.
"UC is a SURFACE wound" · Superficial (mucosal only), Uninterrupted (continuous), Rectum always, Friable + pseudopolyps, Always bloody, Crypt abscesses, curable with colEctomy.
Sort It Out
Feature Sorting
Drag each feature into the right disease. Wrong guesses bounce back.
CROHN'S
UC
Flip the Cards
IBD Pattern Cards
Tap each card to flip and compare Crohn's vs UC on that feature. Lock the contrast, not the list.
DEPTH
Transmural vs Mucosal
How deep does it go?
tap to flip
Crohn'sTransmural (full thickness)
UCMucosal only (superficial)
Transmural = fistulas, abscesses, strictures possible. Mucosal = can't tunnel through wall. Explains ALL the complications.
PATTERN
Skip Lesions vs Continuous
Where is the inflammation?
tap to flip
Crohn'sSkip lesions (patchy)
UCContinuous (no gaps)
UC always starts at rectum, moves proximally. No skip. Crohn's can be anywhere, in patches. Can spare the rectum entirely.
GROSS
Cobblestone vs Lead Pipe
What it looks like
tap to flip
Crohn'sCobblestoning
UCLead pipe + pseudopolyps
Cobblestone = deep ulcers + islands of normal mucosa. Lead pipe = loss of haustra, smooth featureless colon. Both are late-stage findings.
HISTO
Granulomas vs Crypt Abscesses
What the biopsy shows
tap to flip
Crohn'sNon-caseating granulomas
UCCrypt abscesses
Granulomas only in 30-60% of Crohn's cases. If present, they confirm Crohn's. Crypt abscesses = neutrophils in crypts = UC signature.
SURGERY
Curative vs Not Curative
Can surgery fix it?
tap to flip
Crohn'sNOT curative
UCCurative (total colectomy)
UC = colon disease. Remove colon = cure. Crohn's = mouth to anus. Removing a segment doesn't stop recurrence at the anastomosis or elsewhere.
SMOKING
The Smoking Paradox
Protective or harmful?
tap to flip
Crohn'sSmoking worsens it
UCSmoking is protective
Highest-yield IBD fact. Nicotine affects colonic mucus production and immune modulation differently in each disease. Not a treatment recommendation.
The Tell That Locks It
The Perianal-Fistula Tell
One physical finding settles Crohn vs UC faster than any biopsy. Learn to read the tunnel.
New learning trick
A fistula and a sinus tract are hidden tunnels that burrow from inside the bowel out toward the skin near the anus. A fissure is a deep split in the same area. To carve a tunnel from the inside of the gut to the outside, inflammation has to eat through all four layers of the bowel wall. That all-the-way-through pattern has a name: transmural, which simply means full thickness. Only one inflammatory bowel disease goes that deep, so a draining perianal tunnel is a near-certain fingerprint of Crohn disease. Ulcerative colitis stays up on the surface lining only (the mucosa), so it bleeds and ulcerates the top layer but never tunnels.
Plain-word translation: fistula equals a tunnel that opens at two ends (gut to skin). Sinus tract equals a blind tunnel that dead-ends in tissue. Fissure equals a deep crack. Transmural equals through every layer. Mucosa equals the inner surface lining. A surface scrape cannot reach the outside world; a full-thickness burn can.
A patient has months of bloody diarrhea and now a small opening beside the anus that quietly drains pus, with a firm cord you can feel running back toward the bowel. Which process can carve a tunnel like that?
First, what actually IS a fistula, sinus tract, or fissure?A tunnel or a deep crack in the wall. A fistula connects two spaces (bowel lumen to skin). A sinus tract is a blind tunnel that dead-ends in tissue. A fissure splits the lining. All three are the wall being bored through, not just scratched.
How deep must inflammation go to reach the skin?Through every layer: mucosa, then submucosa, then muscle, then the outer coat. A surface-only injury physically cannot reach the outside. Full-thickness disease has a name: transmural.
Which disease is transmural, and which stays on the surface?Crohn is transmural, so it can tunnel: fistulas, sinus tracts, perianal fissures, strictures, abscesses. UC is mucosal only, so it cannot tunnel. It bleeds the surface but never bores a hole to the skin.
So the patient with a draining perianal tunnel has which disease, and which choice is right?Crohn disease. The tunnel is the tell. The right answer is the first option: full-thickness (transmural) inflammation. Warts sit ON the skin; a fistula bores THROUGH the wall.
Perianal fistula or sinus tract or fissure means full-thickness (transmural) disease, and that means Crohn. UC stays on the surface and never tunnels.
Do not get baited by condylomata acuminatum. Those are HPV (human papillomavirus) genital and anal warts: soft, raised, cauliflower-shaped growths sitting on top of the skin. They do not drain, they do not tunnel, and they have nothing to do with bowel inflammation. A wart sits on the surface; a fistula bores through the wall. Bloody diarrhea plus a draining perianal tunnel is Crohn, not a wart.
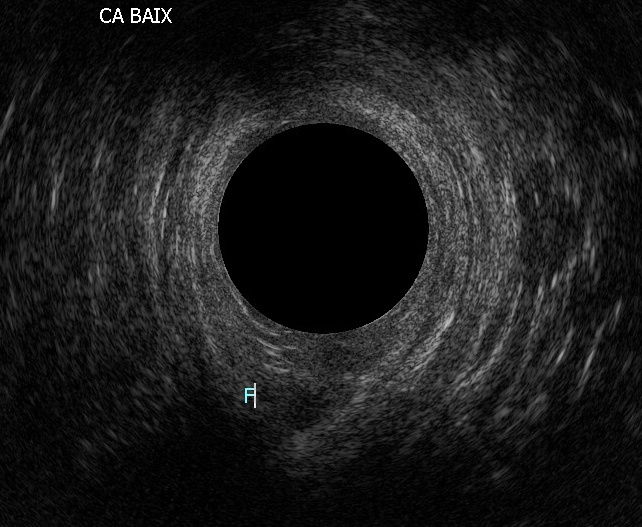
Endoanal ultrasound: the perianal fistula tract (F) tunnelling through the wall · tap to expand
Memory Hooks
Tap to Lock the Contrast
Yellow = hook. Tap to get the board rule. These are the differences that get tested most.
Crohn's goes transmuralFull thickness inflammation through ALL layers of the bowel wall. This is why Crohn's causes fistulas (tunnels through wall), strictures (scar tissue narrows lumen), and abscesses (infection in the wall). UC stays mucosal, so it physically cannot form fistulas. while UC stays mucosalUC inflammation stops at the submucosa. It never penetrates the muscularis propria or serosa. This is why UC can cause toxic megacolon (distension) but not fistulas or strictures. Superficial disease = superficial complications.. Crohn's has skip lesionsPatchy, discontinuous inflammation. Healthy bowel between diseased segments. UC has zero skip lesions. If you see skip lesions on colonoscopy, Crohn's wins. UC is always wall-to-wall from the rectum up. while UC is always continuous from the rectumUC begins at the rectum 100% of the time. It extends proximally in a continuous, uninterrupted pattern. Crohn's can spare the rectum. This is the single strongest distinguisher: rectum spared = Crohn's. Rectum involved + continuous = UC.. The smoking paradoxSmoking worsens Crohn's but is protective against UC. Most-tested IBD fact. Mechanism: nicotine affects mucus secretion in the colon differently than in the small bowel. Don't recommend smoking for UC. trips everyone up. And the PSC connectionPrimary Sclerosing Cholangitis is strongly associated with UC (70% of PSC patients have UC). PSC does NOT track with UC activity. It can progress even after total colectomy. Increases risk of cholangiocarcinoma. Board clue: UC patient + elevated alk phos + beading on MRCP = PSC. links UC to liver disease that doesn't track with bowel activity.
Hook 01
Why fistulas = Crohn's
Tap: Fistulas need full-thickness wallA fistula is an abnormal tunnel between two epithelial surfaces. Creating that tunnel requires the inflammation to burn through the ENTIRE bowel wall. UC can't do this because it only inflames the mucosa. Only transmural disease (Crohn's) has the penetrating power to form fistulas.
Hook 02
Why toxic megacolon = UC
Tap: Megacolon is a distension problemToxic megacolon is massive colonic distension (>6cm) from transmural inflammation of the wall itself. UC inflames the mucosal layer but the colonic wall still absorbs the systemic toxins and loses motor function. Crohn's colitis CAN cause it but it's far rarer. In a board question, toxic megacolon = UC until proven otherwise.
Hook 03
B12 only Crohn's
Tap: Terminal ileum = B12 zip codeB12 (cobalamin) is absorbed EXCLUSIVELY in the terminal ileum via intrinsic factor complex. UC is a colon-only disease. The terminal ileum is small bowel. So UC never causes B12 deficiency. Crohn's involving the TI does. If the vignette has IBD + B12 deficiency, the answer is Crohn's.
Hook 04
Histology as tiebreaker
Tap: Granulomas = Crohn's, alwaysNon-caseating granulomas are pathognomonic for Crohn's when found in the bowel. Even if the colonoscopy looks continuous (Crohn's colitis), the biopsy with granulomas locks in Crohn's. Location suggests; histology confirms. UC never makes granulomas.
Beyond the Gut
Extraintestinal Manifestations
Both can cause problems outside the GI tract. Some track with disease activity. Some don't.
Joints
Which gets arthritis?
Both. Peripheral arthritis tracks with disease activity (flares with gut). Ankylosing spondylitis does NOT track · it runs its own course.
Skin
Erythema nodosum vs Pyoderma gangrenosum?
Erythema nodosum = more common in Crohn's. Tracks with disease. Pyoderma gangrenosum = more common in UC. Does NOT track reliably.
Eyes
What eye problems?
Episcleritis tracks with disease activity (parallels gut flares). Anterior uveitis (iritis) is HLA-B27 linked, runs an independent course, and does NOT track · it groups with PSC and pyoderma gangrenosum. Both occur in UC and Crohn's. Red eye + IBD = think extraintestinal.
Liver
Which causes PSC?
Primary Sclerosing Cholangitis = strongly associated with UC (70% of PSC patients have UC). Does NOT track with disease · can progress even after colectomy. Increases cholangiocarcinoma risk.
Nutrition
Which causes malabsorption?
Crohn's · terminal ileum involvement impairs B12 and bile salt absorption. Also fat-soluble vitamin deficiency (A, D, E, K). UC doesn't usually cause malabsorption because the colon mainly absorbs water.
Stones
Gallstones or kidney stones?
Crohn's gets both. Gallstones: impaired bile salt reabsorption in terminal ileum. Oxalate kidney stones: unabsorbed fatty acids bind calcium, leaving free oxalate to absorb and crystallize.
PSC + UC = high-yield combo. 70% of PSC patients have UC. PSC does NOT improve after colectomy and independently increases cholangiocarcinoma risk. If a board question gives you a UC patient with elevated alk phos and bile duct beading on MRCP, that's PSC.
Finding
Crohn's
UC
Peripheral arthritis
Yes (tracks)
Yes (tracks)
Ankylosing spondylitis
Yes
Yes
Erythema nodosum
More common
Yes
Pyoderma gangrenosum
Yes
More common
Uveitis / Episcleritis
Yes
Yes
Primary Sclerosing Cholangitis
Rare
Strong association
Malabsorption (B12, fat-sol)
Yes (terminal ileum)
No
Gallstones
Yes (bile salt loss)
No
Oxalate kidney stones
Yes (fat malabsorption)
No
Work It Out
Diagnostic Decision Tree
A patient presents with chronic diarrhea and abdominal pain. Walk through it.
Is the diarrhea bloody?
Bloody diarrhea. Where is the inflammation on colonoscopy?
Non-bloody diarrhea. Where does imaging show the disease?
Continuous rectal inflammation. What does biopsy show?
Ulcerative Colitis. Continuous inflammation from rectum + mucosal-only + crypt abscesses = classic UC. Watch for toxic megacolon and increased colorectal cancer risk with duration.
That's unusual. Continuous rectal inflammation with granulomas is atypical. Consider Crohn's colitis (Crohn's limited to the colon) · it CAN look continuous in some cases, and granulomas are the histologic giveaway. This is a board trap: location suggests UC, but histology wins.
Patchy inflammation with possible skip lesions. What's the histology?
Crohn's Disease. Skip lesions + transmural + granulomas = textbook Crohn's. Even with bloody stool · Crohn's CAN bleed, especially Crohn's colitis. The skip pattern is the key.
Tricky. Patchy distribution with only mucosal changes. This is indeterminate colitis territory · about 10-15% of IBD cases can't be neatly classified. clinical medicine usually won't test this, but know it exists.
Terminal ileum involvement. Any complications?
Crohn's Disease. Terminal ileum + fistulas/strictures = Crohn's. These complications happen because the inflammation is transmural · it goes deep enough to create tunnels (fistulas) or narrow the lumen (strictures). UC can't do this because it stays superficial.
Crohn's Disease. Terminal ileum damage causes B12 deficiency (B12 is absorbed here) and bile salt malabsorption (leading to fat malabsorption and steatorrhea). UC doesn't cause these because it only affects the colon.
Patchy colonic disease with non-bloody stools. Key finding?
Crohn's colitis. Cobblestoning = alternating deep ulcers and normal mucosa creating a cobblestone pattern. Creeping fat = mesenteric fat wrapping around bowel. Both are transmural signs that UC cannot produce.
Crohn's Disease. Perianal disease (fissures, fistulas, skin tags) is a strong Crohn's clue. Happens in ~30% of Crohn's patients. UC does NOT cause perianal fistulas because it never goes transmural.
Crohn's colitis mimics UC. When Crohn's is limited to the colon, it CAN look continuous. The giveaway is histology: non-caseating granulomas + transmural inflammation = Crohn's regardless of location. Location suggests; histology confirms.
Elimination Game
Clinical Vignettes
Each clue eliminates one option. By the end, only the answer remains.
Decision Tree
IBD: Crohn's vs UC
Follow the branches. Tap a choice to reveal the next step.
Location of disease?
Think: Ulcerative Colitis
Symptoms: bloody diarrhea and tenesmus.
Colonoscopy: continuous mucosal inflammation, pseudopolyps, lead pipe colon on X-ray.
Treatment: 5-ASA for mild, steroids for moderate, biologics (anti-TNF, vedolizumab) for severe.
Think: Crohn's Disease
Symptoms: abdominal pain, weight loss, perianal disease.
Colonoscopy: cobblestone pattern, skip lesions, fistulae.
Treatment: steroids for flare, MTX or anti-TNF for maintenance, surgery for complications.
Check serology and biopsy
ANCA positive: favors UC. ASCA positive: favors Crohn's.
If indeterminate after biopsy: IBD-Unclassified (IBD-U).
Both UC and Crohn's can cause: uveitis, pyoderma gangrenosum, erythema nodosum. PSC (primary sclerosing cholangitis) is specifically associated with UC. Ankylosing spondylitis is more common with Crohn's.
Test Yourself
Quiz
4 random questions from a pool of 11. Shuffled answers. No timer.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 1, 2026 at 10:03 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.
clinical Walkthrough
clinical Walkthrough
Original clinical vignettes. Shuffled, never-repeat, full explanations for every choice.