Villous adenoma, Lynch, FAP, Peutz-Jeghers, Fearon-Vogelstein, surveillance intervals
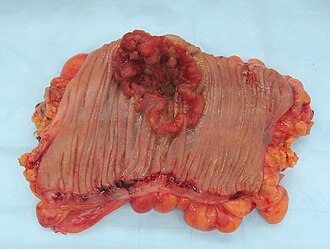
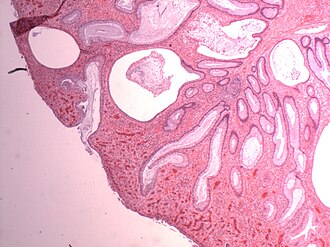
Watch the same crypt drift toward cancer. Bigger, more villous, more dysplastic means more risk. Size and villous architecture are the two things you actually act on.
Three polyps walk into a colonoscopy. One is a tubular adenoma, one is tubulovillous, one is villous. Which one do you watch? The answer you pick tells me everything about whether you understand the actual biology here. Not the name. The biology.
Tap a card to see the full profile.