Ischemia stops oxygen delivery. Oxidative phosphorylation shuts down. The electron transport chain goes silent. The cell's ATP factory just closed.
Na/K-ATPase is the hungriest ATP consumer in the cell. It dies first. Na+ floods in, Cl- follows for charge balance, water follows by osmosis. The cell swells. Anaerobic glycolysis kicks in to compensate, but produces lactate and drops the pH.
These are the first visible changes on histology. The cell is bloated, protein synthesis is stalling, chromatin is clumping. But the membrane is still intact. Restore O2 now and the cell recovers.
The second pump to fail. Ca2+ accumulates in the cytosol. It activates phospholipases (shred membranes), proteases (destroy cytoskeleton), ATPases (burn remaining ATP), and endonucleases (cleave DNA). The cell is now under structural attack from the inside.
Lysosomes burst open. Acid hydrolases digest the cell from inside. The plasma membrane, weakened by phospholipases, breaks. Cytoplasm leaks. This is the point of no return.
Ca2+ floods into mitochondria and forces open the mitochondrial permeability transition (MPT) pore. The proton gradient collapses. That mitochondrion can never make ATP again, even if oxygen returns. Flocculent densities on EM are the death certificate.
Highest O2 demand in the body. Virtually no glycogen reserves. Na+ channels leak constantly, requiring the Na/K-ATPase to run nonstop just to maintain resting potential. Cut the supply and the neuron is dead before the heart even notices.
Hippocampal CA1 neurons and cerebellar Purkinje cells die first in global ischemia.
Continuous contractile work burns through glycogen fast. Moderate reserves buy time, but the heart cannot rest. Subendocardium (furthest from blood supply) dies first in coronary occlusion.
The liver is a glycogen warehouse. Hepatocytes can run anaerobic glycolysis on stored glycogen for a while. Dual blood supply (portal vein + hepatic artery) also provides redundancy.
Can idle at low metabolic rate. Glycogen stores plus low baseline demand mean skeletal muscle tolerates ischemia much longer than brain or heart.
Minimal ATP demand at baseline. These cells are metabolically quiet, which makes them the last to die. This is also why connective tissue survives when everything else is gone.
1. ROS burst: O2 returns to damaged mitochondria. The broken electron transport chain leaks electrons as superoxideSuperoxide, hydrogen peroxide, hydroxyl radical. Normally scavenged by superoxide dismutase and catalase, but the burst overwhelms defenses. instead of routing them to ATP synthase. Massive oxidative damage.
2. Neutrophil infiltration: Inflammatory cells arrive with the restored blood and amplify oxidative damage.
3. Ca2+ overload persists: The MPT pore stays open. Even with O2 back, cells with open MPT pores can never make ATP again. Some cells that were on the edge get pushed past the point of no return.
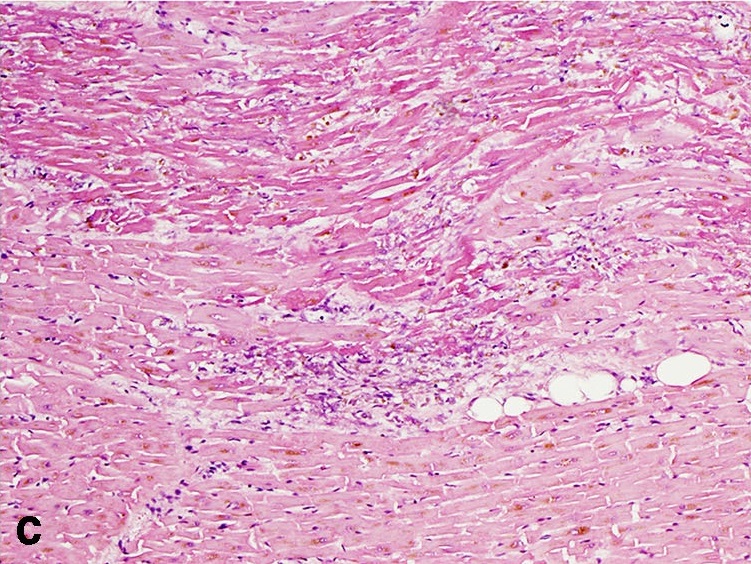
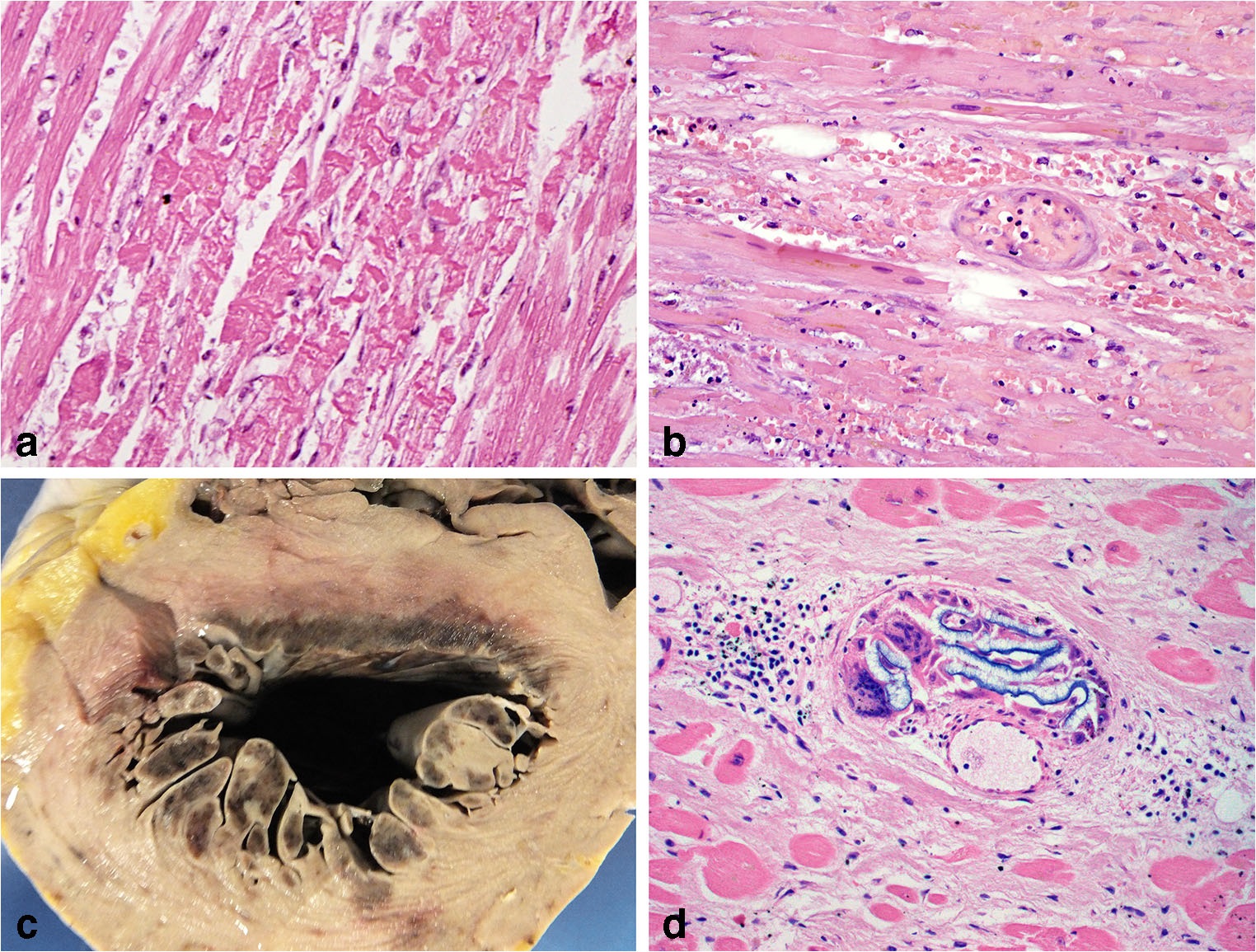
Contraction band necrosis on histology is the hallmark of reperfusion injury. Ca2+-driven hypercontraction of sarcomeres creates dense eosinophilic bands across cardiomyocytes. If you see contraction bands in a post-MI specimen, blood flow was restored before the cell was completely dead.