Three segments, three arteries, one surgical mnemonic that saves careers: "water under the bridge." Stone management thresholds, post-obstructive diuresis, and every board trap in between.
A 48-year-old woman presents to the emergency department with right flank pain and nausea that began 6 hours ago. She underwent a total abdominal hysterectomy for cervical carcinoma 3 days ago. Her postoperative course was initially unremarkable. Temperature is 37.8 C. Urinalysis shows trace blood. CT abdomen/pelvis reveals right hydronephrosis with a dilated collecting system and proximal ureter. No ureteral calculi are identified. The distal ureter is not visualized.
Which of the following is the most likely cause of this patient's hydronephrosis?
THE CLINICAL PHOTOS
Ureter Anatomy and Clinical Imaging
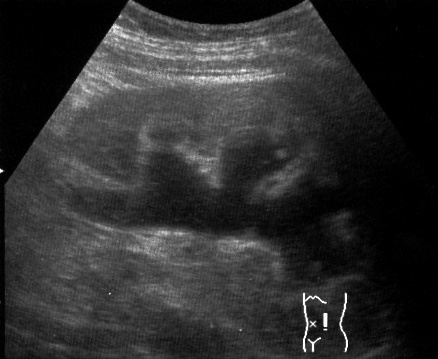
Kidney stones, hydronephrosis on ultrasound, and the surgical anatomy you need to visualize.
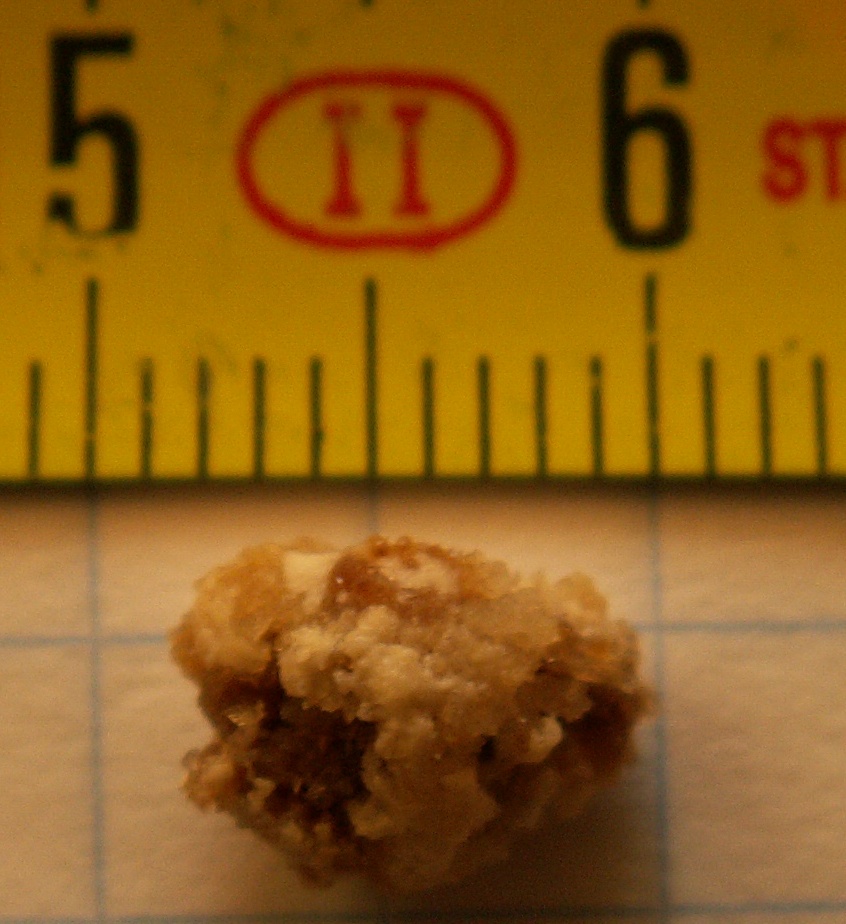
Ureteral Stone (gross)
Hydronephrosis (US)
Ureter Anatomy
Ureteral Stent (device)
The Core Facts
The ureter is a retroperitoneal muscular tube, approximately 25 cm long, that carries urine from the renal pelvis to the bladder. It has three segments, each with a different blood supply, and three natural narrowing points where stones love to get stuck.
Normal diameter: 5 mm. Stones 5 mm or smaller usually pass on their own.
Tamsulosin window: 5 to 8 mm. The alpha-blocker relaxes smooth muscle and can widen the ureter up to 8 mm.
Lithotripsy territory: above 8 mm. The stone will not pass without intervention.
01 · VASCULAR ANATOMY
The Ureter Map
Tap each segment to reveal its blood supply and clinical significance. Three zones, three sources, three places stones get stuck.
Proximal
Middle
Distal
Tap a segment above to see its blood supply and clinical significance
Three Narrowing Points
Stones get stuck where the ureter naturally narrows:
UPJ (ureteropelvic junction): where the renal pelvis funnels into the ureter
Pelvic brim: where the ureter crosses the iliac vessels at the pelvic inlet
UVJ (ureterovesical junction): where the ureter enters the bladder wall. This is the narrowest point and the most common site of stone impaction.
⚠️
Board Trap: "Water Under the Bridge"
The ureter passes under the uterine artery (in females) or vas deferens (in males) near the lateral cervix. During hysterectomy, the uterine vessels are clamped approximately 2 cm lateral to the cervix. The ureter runs right there. If you do not identify it first, you will ligate, kink, or transect it. This is the #1 structure at risk during hysterectomy.
02 · DIFFERENTIAL DIAGNOSIS
The Elimination Game
Eight clinical scenarios. Progressive clues knock out wrong answers until one survives. Tap cards to eliminate them as clues appear.
Scenario 1: The Post-Surgical Complication
A 45-year-old woman is 3 days post-hysterectomy. She develops right flank pain and low-grade fever. CT shows right hydronephrosis. No stones.
The surgeon is asking: what happened to the ureter?
Stone impaction
CT shows no stones
Iatrogenic ligation
"water under the bridge"
Retroperitoneal fibrosis
chronic, bilateral
Ureteral stricture
takes months
Iatrogenic ureteral ligation. "Water under the bridge" at the cardinal ligament.
Scenario 2: The Stone Size Decision
A 32-year-old man has a 4 mm stone in the proximal ureter with mild hydronephrosis. He is in pain but hemodynamically stable.
Which management is correct?
Immediate lithotripsy
overkill for 4 mm
Observation + fluids + pain control
5 mm or less = let it pass
Tamsulosin (medical expulsive)
5 to 8 mm window
Open ureterolithotomy
rarely indicated
4 mm is 5 or less. Let it pass. Fluids, NSAIDs, and patience.
Scenario 3: The Middle Third Blood Supply
A 6 mm stone is lodged at L4. The urologist asks: which artery is the primary blood supply to this segment of the ureter?
L4 is the middle third, between the renal pelvis and the pelvic brim.
Renal artery
proximal third
Gonadal artery
middle third supply
Superior vesical artery
distal third
Inferior mesenteric artery
hindgut, not ureter
L4 = middle third. Blood supply from the gonadal artery and common iliac branches.
Scenario 4: Post-Obstructive Diuresis
A patient had a large stone removed. In the first 4 hours postoperatively, urine output is 350 to 400 cc/hour.
Why is the patient making this much urine?
Diabetes insipidus
wrong mechanism
Diluted medulla (post-obstructive diuresis)
lost concentration gradient
IV fluid overload
output exceeds input
Renal tubular acidosis
does not cause massive output
Post-obstructive diuresis. The obstruction diluted the medulla, so there is no interstitium to concentrate urine. Replace with normal saline every hour.
Scenario 5: Bilateral Hydronephrosis Localization
Imaging shows bilateral hydronephrosis with bilateral ureteral dilation. Where must the obstruction be?
"If it's sitting in the ureter, that could only be on one side."
Right ureteral stone
explains only right side
Bladder or below
both ureters drain here
Left UPJ stricture
explains only left side
Renal artery stenosis
no hydronephrosis
Both ureters dilated = obstruction at the bladder or below. A ureteral stone can only block one side.
Scenario 6: Painless Hematuria
A 65-year-old male smoker presents with painless hematuria. No flank pain, no dysuria, no urgency.
"Cancer of the kidney, ureter, and bladder all present the same way. Painless hematuria."
UTI
dysuria + frequency
Urothelial carcinoma
painless hematuria = cancer until proven otherwise
Kidney stone
pain is the hallmark
BPH
obstructive symptoms
Painless hematuria in a smoker = urothelial carcinoma until proven otherwise. Start workup with cystoscopy and UA.
Scenario 7: The Tamsulosin Window
A 28-year-old man has a 7 mm ureteral stone. He asks: can this pass on its own?
"Between 5 and 8, you can use tamsulosin. It widens the ureter up to 8 mm."
Will pass spontaneously
7 mm is too big for that
Tamsulosin trial
7 mm is in the 5 to 8 window
Immediate lithotripsy
reserved for above 8 mm
Surgical ureterolithotomy
extreme measure
7 mm is in the tamsulosin window (5 to 8 mm). The alpha-blocker relaxes ureteral smooth muscle and can widen the lumen to 8 mm.
Scenario 8: Retroperitoneal Status
A surgeon is planning a retroperitoneal approach. Which structures will be encountered in this space?
The ureter is one of many structures that live behind the peritoneum.
Jejunum
intraperitoneal
Ureter + aorta + IVC
all retroperitoneal
Transverse colon
intraperitoneal
Stomach
intraperitoneal
The ureter, aorta, IVC, kidneys, adrenals, and pancreas (except tail) are all retroperitoneal. SAD PUCKER mnemonic.
03 · clinical WALKTHROUGH
The Walkthrough
25 clinical vignettes. Five answer choices each. Every wrong answer teaches you why it is wrong. Teaching chains reveal the reasoning step by step.
Medically reviewed by Kaitlyn Cocuzzo, MD and Fatima Ali, DO · Last updated July 3, 2026 at 4:30 PM ET
Bone Wizardry is an independent educational resource for visual learning in the medical sciences. It is not affiliated with, endorsed by, or sponsored by any licensing or examination board, contains no real or recalled examination questions, and does not guarantee any educational or examination outcome.